










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSA Orthopaedic Journal
versão On-line ISSN 2309-8309
versão impressa ISSN 1681-150X
SA orthop. j. vol.13 no.1 Centurion Jan./Mar. 2014
HIP
Stress fracture of the femoral neck (SFFN) as a consequence of an unusual occupation: A case report and review of the literature
Dr SS MukansiI; Dr EJ D'AltonII; Prof RG GoleleIII
IMBChB. University of Limpopo, Medunsa Campus
IIMMed(Orth). University of Limpopo, Medunsa Campus
IIIMBChB(Natal), MFGP(CMSA), MMed(Orth)Medunsa, FC(Orth). University of Limpopo, Medunsa Campus
ABSTRACT
Stress fractures of the femoral neck are as old as mankind.1 They affect all ages, young and old. They mostly affect those who are physically active such as military recruits, athletes, especially marathon runners, as well as dancers. We are reporting a case of a femoral neck stress fracture in a 33-year-old male working as a pneumatic drill operator. See also Figure 1.
Key words: stress fractures, unusual occupation, repetitive force, fatigue, insufficiency.
Case report
A 33-year-old male presented to Dr George Mukhari Hospital as a transfer from a peripheral hospital. His main complaint was pain in his left hip, which had been present for a period of 3 months.
The pain did not respond to conservative management which was administered prior to referral. The treatment that he initially received included paracetamol and ibuprofen and a walking stick. Upon systemic enquiry, he had not been on any drugs for conditions which included epilepsy and asthma and he had no history of trauma. He had not been in any military institution and he was not an athlete or dancer. He had worked as a pneumatic drill operator for a few years. However recently since the pain started he became a car salesman which does not require long standing hours.
On examination the left lower limb was 2 cm shorter than the right. There was an increased external rotation. The movements were all limited as a result of pain. All other systems which included blood pressure, chest and abdominal were normal.
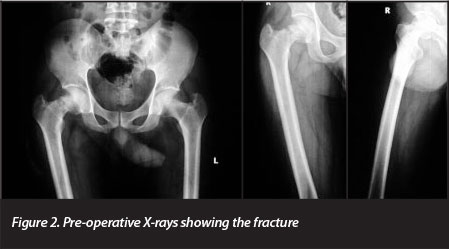
X-rays of the pelvis as well as AP and lateral views of the femur were done on admission. These showed a displaced left-sided fracture of the femoral neck (Figure 2).
Investigations which included FBC, urea and electrolyte, ESR and liver function enzymes were done and these were all within normal limits.
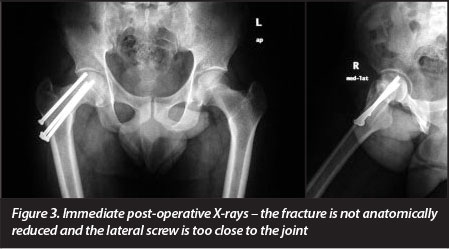
Two days after admission the patient was taken to theatre where a closed reduction and internal fixation was done under general anaesthesia. The fracture was fixed with three cannulated screws under fluoroscopic guidance and the screws were inserted in a triangular fashion. On post-operative X-ray controls, it was evident that an anatomical reduction had not been achieved (Figure 3). The proximal screw was too close to the joint. The patient refused to be taken back to theatre. He was then instructed to start mobilising non-weight bearing on crutches. However after three days he signed refusal of hospital treatment (RHT) forms.
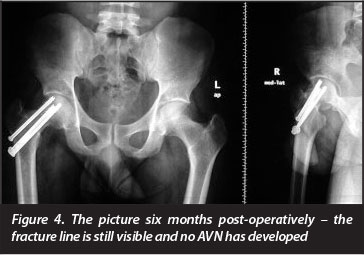
He returned to our outpatients' department six months later. He was pain free and was walking normally. The hip was non-tender and had a full range of motion (Figure 4).
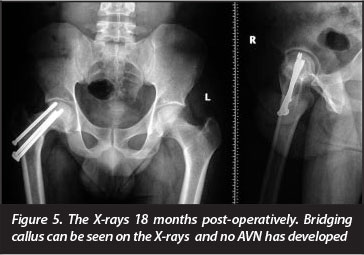
At 18 months post-operatively the patient was still walking without pain and without a limp.
X-rays showed no progression of fracture displacement and there was bridging callus subperiosteally. There were no signs of avascular necrosis (AVN) of the head of the femur (Figure 5).
Review of the literature
The incidence of femoral neck stress fracture is reported to be between 3.5% and 8% in the military population. No incidence for the civilian population is known. Fresh military recruits, dancers and marathon runners are commonly affected by stress fractures of the femoral neck. This usually happens early when an abrupt increase in physical activity is experienced.2
These events occur in normal bone that is subjected to abnormal repetitive exercise. Insufficiency fractures are stress fractures that occur in abnormal bone in the presence of metabolic disorders or osteoporotic bones in the elderly.3 The latter happens during normal activities of daily living and should not be confused with stress fractures that occur in normal bone during a period of abnormal activities.4-6
A typical history should result in one having a high index of suspicion: initially pain is felt after cessation of activity. Subsequently the patient usually feels the pain during the activity. Finally the pain is there all the time.
Imaging
Early in the disease process the X-rays may appear normal. During the advanced stage these fractures can be seen on normal X-rays. It is preferable to make a diagnosis before the stress fracture has reached this stage. Magnetic resonance imaging (MRI) will detect early bone changes that cannot be seen on plain X-rays. Although MRI is more sensitive than normal X-rays, it is very costly. CT scan is also more sensitive than plain X-rays and more cost-effective than MRI. Nuclear bone scan is sensitive but nonspecific.1,2,5,7-10 See also Table I.
Discussion
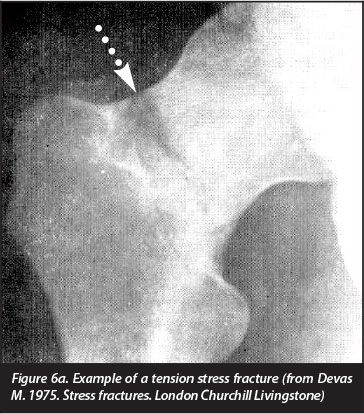
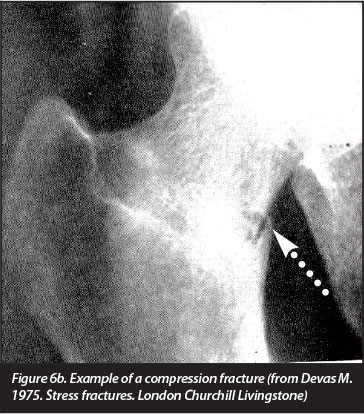
Stress fractures of the femoral neck start as an incomplete fracture, which may initially be difficult to see on standard X-rays (Figure 6a and b).1,10-12 Early X-ray signs include a sclerotic line transverse to the trabecular pattern.5-7 In the case where the fracture progresses there may be a fracture line that involves the femur neck partially. Callus may also be seen. Callus in a stress fracture may be exogenous which is subperiosteal callus formation, or endogenous which is callus formation on the inside of the bone.1,5,12 In cancellous bone the callus is often endogenous and shows a sclerotic line.5 In our patient the fracture was a complete fracture of the neck of the femur that was also displaced.
We did not achieve a perfect reduction of the fracture. Three cannulated screws were used in a triangular fashion percutaneously. Eighteen months post-operatively the original reduction of the fracture is still maintained and the patient is walking with a normal gait and is pain-free. The fracture is united. On X-rays there is bridging callus across the fracture line.
Lee et al report on the surgical treatment of displaced fracture of the femoral neck in military recruits.11 A concern in these fractures is avascular necrosis (AVN) of the femoral head- even after union has taken place.3,7 This may happen as late as 5 years after the initial injury was treated.
In our patient there are no signs of AVN 18 months after surgery (Figure 5). The screw on the superior surface is too close to the joint and has to be removed- but the patient is still undecided about undergoing another operation.
What is strange in our patient is that he developed a stress fracture without the usual predisposing factors. We wonder if being a pneumatic drill operator could have contributed to this.
The complications of femoral neck stress fractures are progression from undisplaced to displaced fractures- nonunion- mal-union and osteonecrosis. Our patient has developed a mal-union. Table I is a summary of the signs and symptoms and finding on investigations.
The gateway to the diagnosis is a high index of suspicion when the pain pattern and exercise pattern change. In the first two stages when MRI is normal the patient may be treated by weight relief and rest. As soon as the fracture is established with a clear line ORIF (open reduction internal fixation) is indicated. When surgery is indicated transcer-vical screws is the preferred method of treatment.10,12
When the stress fracture is diagnosed on the superior surface, which is the tension side of the neck of femur, then urgent surgery is indicated. When the stress fracture is on the inferior side of the neck, which is the compression side, care should be taken because an incomplete stress fracture has been shown to progress to a complete fracture with marked displacement when the patient is subjected to minimal trauma.4,5,10 For this reason others recommend that cannulated screws be inserted as soon as the diagnosis is made. When the fracture is complete and displaced, very urgent treatment is indicated.
When the plain X-rays are not diagnostic, MRI is the investigation of choice since it is specific, non-invasive and will differentiate stress fractures from other causes of anterior hip pain. See also Table I.
Although the history and findings in a stress fracture are almost diagnostic, one should consider osteoid osteoma/osteosarcoma round cell lesions (Ewing's sarcoma and Langerhans cell histocytosis).
Conclusion
Because the SFFN are rare, one should have a high index of suspicion when a young patient complains of hip pain. In these cases MRI and sometimes CT scans may be diagnostic.
References
1. Devas, M. Stress fractures. 1975. London Churchill Livingstone. [ Links ]
2. Brockwell J, Yeung Y, Griffith FJ. Stress fractures of the foot and ankle. Sports Med Arthosc. Rev Sept 2009;17(3). [ Links ]
3. Soubier M, Dubost JJ, Biosgard S, et al. Insufficiency fractures. A survey of 60 cases and review of literature. Rev Sept 2009;17(3). [ Links ]
4. Pihlajamaki HK, Ruohola JP, Kiuru MJ, Visuri TI. Displaced femoral neck fatigue fractures in military recruits. J Bone Joint Surg Am. Sep 2006;88(9):1989-97. [Medline] [ Links ]
5. Maffulli N, Longo UG, Denaro V. Femoral neck stress fractures. Oper Tech Sports Med 2009;17:90-93. Elsevier. [ Links ]
6. Bouchoucha S, Barsaoui M, Saied W, Trifa M, Khalifa SB, Bengachem M. Bilateral stress fractures of the femoral neck with no risk factor: A case report. La Tunisie Medicale 2011;89(3):295-97. [ Links ]
7. Spitz DJ, Newberg AH. Imaging of stress fractures in the athlete. Radiology Clin. AM 2002;40:P313-331. [ Links ]
8. Shocum KA, Gorna JD, Puckett MC, Jones SB. Resolution of Abn MR sign. Insensitive in patients with stress fractures of the femoral neck. AJR 1992;168:1295-99. [ Links ]
9. Provencher TM, Baldwing JA, Gorman DJ, Gould TM and Shin YA. Atypical tensile-sided femoral neck stress fractures. The value of magnetic resonance imaging. American Journal of Sports Medicine. 2004;32(6). [ Links ]
10. Truong TH, Chew SF. Femoral neck fracture imaging. http://emedicinemedscape.com/article/390598-overviewupdatedmay25,11 [ Links ]
11. Lee CH, Huang GS, Chao KH, Jean JL, Wu SS. Surgical treatment of displaced stress fractures of the femoral neck in military recruits: a report of 42 cases. Arch Orthop Trauma Surg. Dec 2003;123(10):527-33. [ Links ]
12. Boden BP, Osbahr DC. High risk stress fractures - evaluation and treatment. American Academy of Orthopaedic Surgeons. 2000. [ Links ]
 Correspondence:
Correspondence:
Dr SS Mukansi
Department of Orthopaedics University of Limpopo (Medunsa Campus)
PO Box 25
Medunsa 0204
Tel: 012 521 4049 Fax: 012 521 4284
Email: Leonie.Strauss@ul.ac.za
There was no third party involved in the preparation of this work. The sole motivation was to add to the body of knowledge on the subject.


{kind=link}
{kind=link}