










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSA Orthopaedic Journal
On-line version ISSN 2309-8309
Print version ISSN 1681-150X
SA orthop. j. vol.12 n.3 Centurion Sep. 2013
UPPER LIMB
Case report: Giant lipoma of the hand
L LisendaI; S van DeventerII; T PikorIII; M LukheleIV
IMBChB(BAO), MRCS Orthopaedic Registrar
IIMBBCh, FC(Orth)(SA) Consultant Orthopaedic Surgeon
IIIMBBCh, FC(Orth)(SA) Consultant Orthopaedic Surgeon
IVMBBCh, FC(Orth)(SA), MMed(Orth) Professor of Orthopaedics Hands Unit, Charlotte Maxeke Johannesburg Academic Hospital, University of the Witwatersrand
ABSTRACT
Giant lipomas of hand are rare lipomas that are larger than 5 cm. Comprehensive history and clinical examination is usually sufficient to make the diagnosis of lipoma but with giant lipoma, liposarcoma cannot be excluded. We report a case of giant lipoma in which we excluded liposarcoma by MRI and proceeded to do excisional biopsy. The histology confirmed our pre-operative diagnosis of lipoma, and post-operatively the patient did very well and returned to work with normal function of the left thumb.
Keywords: giant lipoma, hand
Introduction
Lipomas are common benign soft tissues of the upper extremity but are rare in hands.1 They consist of 5% of upper limb tumours and about 1-3% of benign tumours of hand.2,4 Mason classified lipomas of hand as endovaginal and epivaginal relative to the involvement of the tendon sheath.3 Giant lipomas have been described as those that are larger than 5 cm. The differential diagnosis of giant lipoma includes liposarcoma which requires a different treatment approach.1 MRI is therefore helpful in these cases, not only for defining the extent of neurovascular and tendon engulfment, but also the assessment of fat content and septal wall thickness.2 The decision must be done in concert with the clinical picture that is suggestive of malignant lesion, for example, a painful, fast-growing lesion would be suspicious. We report a case of giant lipoma on the first web space of the left hand.
Case report
Ms DM is a 23-year-old, right-handed, domestic worker who presented with a 10-year history of painless progressive swelling over the first web space of her left hand.
She denied any history of trauma. Examination revealed 10 χ 8 cm smooth, rounded, mildly tender swelling with prominent veins but normal temperature. The lesion was firm in consistency; no pulsation was present. Sensation was normal. Flexion, adduction and circumduction of the thumb were limited as the thumb was held in extension as shown in Figure 1.

The lesion was clearly demarcated on X-rays as a large homogenous soft tissue mass. No bony changes were noted (Figure 2). A MRI T1 sequence showed a hyperintense lesion with reduced signal fat suppression and a central area of necrosis (Figure 3). Thumb and flexor tendons were abutted but not encased while the digital vessels were encased and splayed within the mass.


Clinical and radiological findings supported the diagnosis of a giant lipoma.
MRI is helpful in these cases, not only for defining the extent of neurovascular and tendon engulfment, but also the assessment of fat content and septal wall thickness
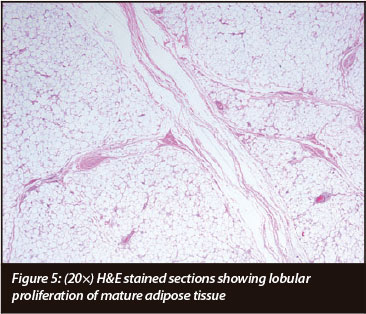
The operation was done under general anaesthesia and tourniquet. A modified Brunner incision was performed and the lesion was dissected and removed completely, preserving the neurovascular bundle. The tumour was a 12 χ 10 χ 8 cm lesion which weighed 291 grams (Figure 4). Histology revealed lobular proliferation of mature adipose tissue with slight variation of adipocyte size with no evidence of nuclear hyperchromasia features in keeping with giant lipoma (Figure 5). The patient was referred for occupational therapy. She had full return of function post-operatively and returned to work after 4 weeks (Figure 6).


Discussion
Giant lipomas have been described as those that are larger than 5 cm. They usually present as a slow painless mass with little functional disturbance leading to late presentation. Some cases present with neurological symptoms secondary to compression of the neurovas-cular bundle.5 X-rays reveal soft tissue mass without bone involvement. Ultrasound is also helpful but the MRI is the most sensitive and specific imaging modality. The T1 image reveals a hyperintense lesion and fat suppression. Central necrosis on some images of the MRI is suspicious of liposarcoma. The presence of less than 75% fat content and thick, enlarged septa after gadolinium injection is suggestive of a liposarcoma.2 The MRI also demarcates the neurovascular bundle and tendons and helps with pre-operative management.2,5 Lesions that are suspicious for malignancy require full tumour work-up and management as a malignancy.
Management consists of observation for small asymptomatic lesions to excisional biopsy.2,5 An indication for excisional biopsy includes pain secondary to compression on nerves, impaired function of hand and cosmesis. Outcome of surgery is excellent with most patients resuming full function within a few weeks. This was the outcome in our case.
Complications of untreated lipomas include: compression of neurovascular structures, functional impairment and potential for malignant transformation - the most common being liposarcoma. Complications of surgery are risk of injuring the neurovascular structures in addition to infection.5 There are currently no reported cases of recurrence for fully excised lipomas.
he presence of less than 75% fat content and thick, enlarged septa after gadolinium injection is suggestive of a liposarcoma
Conclusion
Our report emphasises that thorough history, clinical examination and focused investigation are essential for making correct decisions regarding uncommon clinical conditions. Giant lipomas can be safely removed with excellent functional and cosmetic outcomes.
Acknowledgements
Dr ED McAlpine and Dr R Wadee, Division of Anatomical Pathology, School of Pathology, Faculty of Health Sciences, University of the Witwatersrand and National Health Laboratory Services for doing the histology.
The content of this article is the sole work of the author. No benefits have been received from any commercial party. This case report was not submitted to the ethics committee.
References
1. Pagonis T, Givissis P, et al. Complications arising from a misdiagnosed giant lipoma of the hand and palm: a case report. Journal of Medical Case Reports 2011;5:552. [ Links ]
2. Decrouy-Duruz V, Kalbermatten DF, et al. Giant lipoma of the thumb. Eur J Plast Surg. DOI 10.1007 [ Links ]
3. Inaparthy P, Southgate GW. Giant lipoma of hand: a case report. Eur J Orthop Surg Traumatol 2006;16:251-52. [ Links ]
4. Gupta A, Singal R, et al. Report of two cases of subcutaneous lipoma over the finger and review of literature: case series. Musculoskelet Surg 2011;95:247-49. [ Links ]
5. Nadar MM, Bartoli CR, et al. Lipomas of the hand: a review and 13 patient case series. Open Access Journal of Plastic Surgery. Oct 25 2010. [ Links ]
 Reprint requests:
Reprint requests:
Dr L Lisenda
Division of Orthopaedics. Room 4M12
Wits Medical School 7 York Road 2193 Parktown
Email: lisendal@hotmail.com

