










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSA Orthopaedic Journal
On-line version ISSN 2309-8309
Print version ISSN 1681-150X
SA orthop. j. vol.12 n.3 Centurion Sep. 2013
UPPER LIMB
Multicentre retrospective study comparing outcome of pinning and locking plates for treating distal radius fractures
MJ DurransI; S PretoriusII; M WellsIII; A IkramIV
IMMed(Orth)(Stell), FCS(Orth)(SA) Orthopaedic Surgeon in private practice
IIMMed(Orth)(Stell), FCS(Orth)(SA) Consultant at Tygerberg Hospital and Orthopaedic Surgeon in private practice
IIIMMed(Orth)(Stell), FCS(Orth)(SA) Orthopaedic Surgeon in private practice
IVMBBS, FCS(Orth)(SA) Head of Hand Surgery at Tygerberg Hospital Department of Orthopaedic Surgery, Stellenbosch University, Tygerberg Hospital, Cape Town
ABSTRACT
BACKGROUND: Distal radial fractures are extremely common in the South African private and provincial sector, with intraarticular fractures making up a large portion of this group. Closed reduction is the cheapest method of treatment but the results are poor. Closed reduction and pinning is the next most cost-effective option with slightly better results. Plating of these fractures is another option. Volar locking plate systems have been shown to be the gold standard for fixation of these fractures with good to excellent objective and functional outcomes. The cost of these plating systems is, however, extremely expensive, and the need has arisen to identify patients that can be treated more affordably in the South African provincial healthcare system.
AIM: To compare the functional outcomes of patients with intra-articular distal radius fractures treated with volar locking plates, and of those treated with closed reduction and pinning.
METHODS: The multicentre retrospective study comprised two groups of patients: one group treated with volar locking plates; and the other treated with closed reduction and pinning. The functional outcome was our main objective, with objective outcomes and complications our secondary objectives.
RESULTS: Statistically the results showed that the two groups did the same functionally even though objectively there were more complications in the closed reduction and pinning group. The only statistically significant finding was that the time to functional pain-free independence was 6 weeks earlier in the plate group than in the Kirschner wire (K-wire) group.
CONCLUSIONS: Using these results we suggest that patients who have a good support system and/or can afford the time off work be treated with closed reduction and pinning. Those patients who have a poor support system and who cannot afford lengthy times away from work should be treated with volar locking plates. Further studies of this subject are needed.
Introduction1-4
Distal radius fractures account for one sixth of all fractures seen in the emergency room and 60% of them are intra-articular (Leung et al4). Abraham Colles1 first described this injury in 1814 and since then more than 4 000 articles have been published relating to distal radius fractures and their treatment. Methods for treatment of intra-articular distal radius fractures include cast immobilisation, pinning and casting, pinning and external fixation, dorsal plating, volar plating, volar and dorsal plating and finally the newest volar locking plates.
Volar locking plates have become the gold standard for fixation of distal intra-articular radius fractures. However in our trauma unit and in South Africa's public sector, budget restraints are a reality and resources need to be managed effectively. Volar locking plates are 500 times the cost of plaster and Kirschner wires (K-wires).
The purpose of this study is to compare the functional outcome of patients with intra-articular distal radius fractures (Figure 1a) who are treated with volar locking plates (Figure 1b) and those whose intra-articular radius fractures can be reduced and held reduced with pinning and casting (Figure 1c), in an attempt to give a cost effective guideline for treatment of patients.



Literature review
Anatomy (Figure 2)3,5-9

The distal radius is involved in two articulations: 1) the radiocarpal joint and 2) the distal radio-ulnar joint.
The proximal bony anatomy of the radiocarpal articulation is made up of the radial styloid laterally and progressing medially: the scaphoid fossa, lunate fossa and the triangular fibrocartilage complex (TFCC) overlying the distal ulna. The scaphoid, lunate and triquetram bones make up the distal bony anatomy. The dorsal and volar radiocarpal ligaments attach to the before-mentioned bones and play a role in displacement if fractured.
In South Africa's public sector, budget restraints are a reality and resources need to be managed effectively
The distal radio-ulnar joint bony anatomy is made up of the head of the ulna and the sigmoid notch of the distal radius held together by the TFCC and capsule.
The extensor surface has three grooves for the extensor carpi radialis longus and brevis, the extensor pollicis longus and the extensor digitorum communis and extensor indicis respectively. The second and third groove are separated by the dorsal radial tubercle of Lister.
The volar surface has a regular surface with no grooves or tubercles and is covered by the pronator quadratus and then by the flexor compartment.
Incidence4,5,7
Fractures of the distal radius make up 17% of all fractures seen in the emergency room, and 60% of these fractures are intra-articular.
Mechanism of injury3,5,7,8,10
The most common cause is fall onto an outstretched hand especially in osteoporotic patients, but high velocity trauma such as fall from a height, motor vehicle accidents and contact sports are other aetiological factors. Pathological fractures, except those in osteoporosis, are rare in the distal radius.
Classification2,3,5
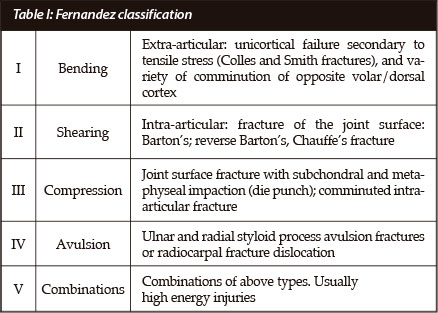
Numerous classifications exist. The Fernandez and Jupiter classification is based on the mechanism of injury (Table I). Type I fractures are extra-articular bending fractures such as the Colles and Smith fractures. Type II fractures are intra-articular and produced by shearing, and these include volar and dorsal Barton fractures and radial styloid fractures. Type III fractures are intra-articular and result from compressive forces that cause compression of metaphyseal bone. Type IV fractures are avulsion fractures caused by ligament avulsions and are associated with radiocarpal dislocations. Type V are high energy injuries due to combination of shear and extension forces. The Frykman classification (Table II) is an anatomical classification and based on the extent of involvement of the articular surface of the distal radiocarpal (DRCJ) and distal radio-ulnar (DRUJ) joints.

Type I is an extra-articular radius fracture; type II is an extra-articular distal radius fracture with an associated ulna styloid fracture; type III is an intra-articular fracture without an ulna styloid fracture; type IV is intra-articular fractures with an associated ulna styloid fracture; type V is a fracture that involves the radio-ulnar joint only; type VI is a fracture involving the radio-ulnar joint with a ulnar styloid fracture; type VII is an intra-articular fracture involving both the radiocarpal and the radio-ulnar joints without a radial styloid fracture; and type VIII is an intra-articular fracture involving both the radiocarpal and radio-ulnar joints and an associated ulnar styloid fracture.
The columnar classification is used for compression injuries and identifies four components: the radial shaft; the radial styloid; the posteromedial portion of the lunate facet of the distal radius; and the palmar medial portion of the lunate facet.
Patho-anatomy (Figures 3 and 4)2,5,7,9


Distal radius fractures with intra-articular extension result in shortening of the radius with malalignment of the distal radio-ulnar joint causing limited pronation and supination. Radial angulation of the fracture causes limited excursion of the extensor and flexor tendons and results in limited power grip. Dorsal and volar angulation in turn cause limited range of motion of the radiocarpal joint. Displaced intra-articular fractures, especially those extending into the scaphoid and lunate fossa, can cause accelerated osteo-arthritis of the radiocarpal joint and instability of the distal radio-ulnar joint.
Clinically5,7
Pain, swelling and deformity are the main complaints. One must be alert to symptoms and signs of forearm compartment syndrome especially in high velocity injuries, and also to acute carpal tunnel syndrome in any distal radius fracture.
The clinician must rule out scaphoid fractures, scapholunate instability, transscaphoid and/or perilunate dislocations, triangular fibrocartilage complex tears as well as radial head fractures in patients with distal radius fractures as these have treatment implications.
Imaging2,5,7,9
The standard AP and lateral radiographs comprise the imaging needed in such patients. Additional imaging may include traction radiographs to better delineate the fracture; stress radiographs to elucidate any wrist instabilities; and CT scanning to evaluate the congruity of the distal radiocarpal joint and any associated carpal fractures.
Management2,5,7,9,11-13
Management of these patients must include initial evaluation and immobilisation with a backslab, traction or temporary external fixator, depending on the extent of soft tissue swelling. Monitoring of the patient for compartment syndrome and/or median nerve compression is mandatory. Secondary management includes relevant imaging modalities and the specific reduction technique and/or fixation device needed to suit the patient's profile.
The goal of treatment modalities as with all intra-articular fractures is to obtain anatomical intra-articular reduction that is stable enough to withstand early mobilisation.
Kirk and Jupiter13 found that 91% of wrists that had greater than 1 mm of incongruity developed radiological evidence of degenerative joint disease (DJD) and 100% of wrists that had more than 2 mm of incongruity develop DJD after an average of 6.7 years. They proved that residual joint incongruity would lead to radiographic DJD in about 75% of wrists at an average of 7 years. However, this did not necessarily correlate with clinical evidence of DJD and functional status. Anatomical reduction with stable fixation is the treatment of choice for displaced, unstable fractures. The challenge, however, for all forms of treatment is the maintenance of reduction until bony union occurs.
In general, procedures involving long terms of immobilisation for intra-articular distal radial fractures lead to poor functional results. The operative tactic for compression fractures involves restoration of the four common fragments: the radial shaft, the radial styloid, the posteromedial portion of the lunate facet and the palmar medial portion of the lunate facet - in sequence. This can be accomplished by manipulative means alone via ligamento-taxis, with limited exposure of the fracture fragments and stabilisation with percutaneous K-wires or open reduction and internal fixation techniques.
Closed reduction5,7,10,14-17
Closed reduction of minimally displaced intra-articular radius fractures can be used in those not fit for or refusing surgical treatment, resulting in a fair to good functional outcome. However a large number of fractures displace using this method.
Closed reduction and pinning5,7,10,14-16
Minimally displaced fractures can be reduced and held with percutaneous pinning and casting but severely displaced fractures have a tendency to displace due to the inability to neutralise surrounding forces. Carlos Rodrigues-Merchan10 showed that closed reduction and pinning improved both anatomical and functional outcome compared to closed reduction and cast immobilisation alone. The Kapandji technique can also be used to help reduce lunate fossa impaction lesions otherwise known as 'die punch' lesions and other displaced fragments percutaneously, negating the need for open reduction.
Dorsal plating5,7,9,18
Dorsal plating has been used as a method of treatment of distal radial fractures but extensor tenosynovitis and extensor tendon rupture are common complications and have led to the introduction of volar locking plating systems.
External fixation5,7,19,20
Studies have shown that joint-bridging external fixation may maintain radial length; however, individual fracture fragments may still heal in displaced or angulated positions. Numerous authors also mention that prolonged immobilisation and overdistraction can lead to persistent loss of wrist motion.
Volar buttress plating5,7,9,21-23
The treatment of shearing type fractures usually demands a buttress-type plate, and displaced unstable fractures require a cross-wrist external fixator or a combination of volar and dorsal plating or the newer volar locking plate systems to maintain reduction. David et al21 compared volar and dorsal plating in the treatment of intra-articular radius fractures. They found that the DASH score was similar in the two groups but the Gartland and Werely score was better in the volar locking plate group. The dorsal plating group had a high rate of complications such as volar collapse, dorsal tenosynovitis and extensor tendon rupture and this has been shown in the majority of other studies.
Volar locking plates5,7,9,23-25
Trease et al25 stated in their study that the volar approach for plating is associated with fewer complications because the anatomy of the volar aspect of the wrist offers more cross-sectional area, and the implant is separated from the flexor tendons by the pronator quadratus. In their study they state that volar plating of distal radius fractures would be a reasonable alternative to prevent dorsal plate-related complications. They also mention that standard plates might not have sufficient strength when dorsal comminution exists.
Complications5,7,9,26,27
The complications of intra-articular radius fractures can be grouped into:
1) Pre-operative complications, which include median nerve compression, severe soft tissue swelling and the less common forearm compartment syndrome
2) Intra-operative complications, which include the inability to reduce the fracture due to comminution, nerve and vessel damage, and the inability to close the wound due to soft tissue swelling.
3) Post-operative complications, which can be grouped into early and late, and which include median nerve compression due to haematoma, radial nerve dorsal branch injury due to temporary or definitive K-wire placement, early wound infection and breakdown.
4) Late complications include loss of motion of the distal radio-ulnar and the radial carpal joint, flexor tendon tenodesis, extensor tendon synovitis, attrition and ultimate rupture due to dorsal prominence of the volar locking screws, prominent metal work alone, complex regional pain syndrome, complications associated with the removal of the fixation device and ultimately degenerative secondary osteo-arthritis.
Materials and methods
Study design
The study design was a retrospective multicentre study. The three units involved were the Tygerberg Orthopaedic Hand Department and two private orthopaedic hand surgeons.
Aims
The aim of the study was to attempt to identify a cost-effective treatment protocol for treatment of intra-articular radius fractures in the state hospitals in South Africa by comparing the functional outcome of patients treated with closed reduction and pinning to those treated with volar locking plates.
Objectives
The primary objective of the study was to compare the functional outcome of patients with intra-articular radius fractures treated with closed reduction and pinning and those treated with volar locking plates. Secondary objectives included objective outcomes, time till pain-free independent functioning, and complications between the two groups.
Patient selection
The inclusion criteria were:
• Patients aged 18 years and older
• Intra-articular distal radius fractures treated with closed reduction and pinning or volar locking plates
• Four months or more from the time of injury
Exclusion criteria were:
• Mental retardation or dementia
• Neuromuscular disease
• Previous forearm injuries or previously fractured distal radius
• Pathological fractures
• Open fractures
• Associated nerve injuries to the ipsilateral limb
• Associated Essex-Lopresti injury
Data capturing28,29
The three participating centre databases were scanned for intra-articular radius fractures treated with closed reduction and pinning and those treated with locking plates. Twenty-five closed reduction and pinning patients were found that met the inclusion and exclusion criteria of which only 13 were available for the investigation (one patient had bilateral fractures, and 12 patients were unable to be contacted). Forty-six locking plate patients were found that met the inclusion and exclusion criteria and from this group 32 patients were available for the study if needed. From these 32 patients, 13 patients were consecutively selected; there were 16 fractures (three patients had bilateral fractures). Informed consent was granted by each patient to be examined and have his or her data used in the study.
The fractures were classified using the Frykman classification as it is an anatomical classification and has good intra-observer reproducibility.
The patient's outcome was measured using the DASH score28 and the Gartland and Werely demerit scoring system.29
The Disabilities of the Arm, Shoulder and Hand (DASH) outcome measurement system was developed by the American Academy of Orthopedic Surgeons to measure the outcome of interventions used for the upper extremity. The main section of the DASH is a 30-item disability/ symptom scale that enquires about the patient's perception of his or her functional ability during the preceding week. Twenty-one items ask about the degree of difficulty in performing certain physical activities because of an arm, shoulder or hand problem. Five items relate to the symptoms of pain, activity-related pain, tingling, weakness and stiffness. Four items relate to the effect on social activities, work, and sleep and its psychological impact. Finally there are also two optional four-item scales that enquire about the patient's ability to perform sports and/or to play a musical instrument and the ability to work (the sport and work scale respectively). Each of the abovementioned items has a choice of five responses ranging from 'no difficulty or no symptom' to 'unable to perform activity or very severe symptom', and is scored on a 1- to 5-point scale. The sum of all the scores is used to calculate a scale score ranging from 0 (no disability) to 100 (severest disability).
The Gartland-Werely demerit-scoring system that was later modified by Sarmiento is an objective and subjective system that has four sections. The first section deals with the radiological outcome of the fracture, while the second section deals with the objective symptoms such as pain, loss of motion and functional limitation. The third section gives points for subjective outcome of motion, distal radial ulnar joint pain and grip strength of the wrist measured by the physician. Finally the fourth section gives points for complications such as osteo-arthritic changes on radiographs, nerve complications and finger function. The sum of the points is then used to give an outcome score. Zero to 2 is excellent, 3-8 is regarded as a good outcome, 9-20 is a fair outcome and finally >20 is regarded as a poor outcome.
Grip, pinch grip and key grip strength of each hand was measured.
Complications experienced by each patient were noted however minor or major they appeared to be.
Results
Closed reduction and pinning group (Figures 5 and 6)
The closed reduction and pinning group consisted of 13 patients: nine female and four male (one bilateral). The Frykman fracture types included two type III, two type IV, one type V, two type VI, three type VII and four type VIII. Two patients were left hand dominant. The mean age of the patients was 50 years (range 32-70 yrs). The time since injury was a mean of 36 months (range 4-200 months).
The mean DASH score was 11.9/ 11.6/ 0 (range 0-33.3/ 0-75/ 0-37.5). The mean Gartland-Werely score was 9.5 (range 1-25). Grip strength measurements (in kg) showed a mean of 12/18/16/12/13 for the right hand and 12/19/18/14/13 for the left hand. Pinch grip measurements (in kg) produced a mean of 4.5 for the right hand and 4.3 for the left hand. Key grip readings (in kg) showed a mean of 6.1 for the right hand and 5.7 for the left hand. The range of motion of the affected and unaffected wrists showed an average loss of 15° of extension (range 5-50°); pronation and supination showed a mean loss of 3° (range 0-50°); flexion showed a mean loss of 10° (range 0-35°); and radial deviation showed a mean loss of 1.1° (range 0-15°) and ulnar deviation by 0.2° (range 0-12°). Time till pain-free independence was a mean of 9 weeks (range 6-12 weeks).
Complications in the closed reduction and pinning group consisted of: one patient developed a mal-union with 30° volar tilt, DRUJ pain and radial shortening of 2 mm. One patient had extensor tendon tenodesis and migration of the K-wire to mid- forearm. One patient developed mild reflex sympathetic dystrophy (RSD); and one patient had decreased sensation to her third finger (unknown if was pre or post-operative). There were also two reported cases of neurapraxia of the dorsal branch of the radial nerve; three cases of asymptomatic DRUJ instability; and two cases with residual dorsal tilt of 5° and one case of an intra-articular 1 mm step.
Grip, pinch grip and key grip strength of each hand was measured
The volar locking plate group (Figures 7 and 8)

There were 16 fractures in 13 patients, three of whom had bilateral injuries. There were nine female (two bilateral) and four male (one bilateral) patients. The Frykman fracture patterns consisted of three type II, one type IV, one type V, six type VII and five type VIII. The mean age was 54.3 years (range 22-79 years). The mean time from injury was 12.6 months (range 4-20 months). Two patients showed left hand dominance. The mean DASH score was 9.77/ 12.5/ 28 (range 3.3-13.4/ 0-37.5/ 0-88). The Gartland-Werely score had a mean of 9 (range 1-18). The grip strength measurements (in kg) showed a mean of 16/20/21/17/14 for the right hand and 12/21/19/17/12 for the left hand. Pinch grips (in kg) produced a mean of 6.3 for the right hand and 5.9 for the left hand, and key grip strength (in kg) showed a mean of 7.4 for the right hand and 7.3 for the left hand.
The range of motion measurements of the injured and uninjured side showed an average loss of extension of 2° (range 0-25°); loss of flexion of 3° (range 0-55°); loss of pronation and supination of 1° (range 0-15°); loss of radial deviation of 1° (range 0-15°); and finally loss of ulnar deviation of 0° (range 0-15°). The mean time till pain-free independence was 4.6 weeks (range 1.5-18)
Complications encountered included: one patient developed early wound sepsis and bilateral post-operative carpal tunnel syndrome and limited pro- and supination of the right hand and had to undergo right carpal tunnel and DRUJ releases. One patient developed RSD and symptomatic DRUJ instability and an intra-articular step of 1 mm. Two patients developed late carpal tunnel syndrome. Other complications found were: two patients had prominent screws; two had extensor tenosynovitis; one patient had asymptomatic DRUJ instability; and one patient had an asymptomatic intra-articular 1 mm step.
Statistical analysis30,31
Statistical analysis of the results was conducted in conjunction with The Centre for Statistical Consultation, Stellenbosch University, using the STATISTICA data software program.31 Statistical interferential analysis of the two treatment groups was performed using the ANOVA F-test system and checked using the non-parametric Mann-Whitney testing system.
There were no statistical differences between the two groups with regard to age, time since injury (T1), gender, hand dominance, Frykman type of fractures, grip/pinch/ key-grip strengths of the injured and unaffected hand, all ranges of motion and the Gartland-Werely score as shown with their p-values all being above 0.005.
The one statistical relevant finding was the time to pain-free function (T2). The T2 for the plate group was found to be 4.8 weeks with a standard deviation of 3.7 weeks. The T2 for the K-wire group was 8.75 weeks with a standard deviation of 2.0 weeks
The graph in Figure 9 demonstrates the distribution of the patient's DASH scores along the expected mean value (red line).

Table III shows the comparison of DASH scores between the plate and K-wire group showing a p-value of 0.65299 that implies that the difference in results between the two groups is statistically insignificant.
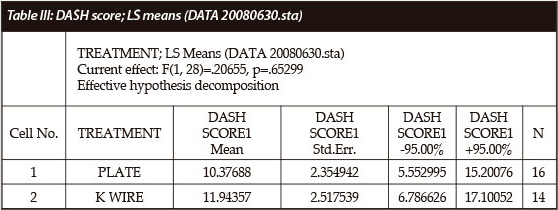
All except one group of results showed almost similar statistical distribution and relevance as shown by the highlighted DASH scores in Table III.
The one statistical relevant finding was the time to pain-free function (T2). The T2 for the plate group was found to be 4.8 weeks with a standard deviation of 3.7 weeks. The T2 for the K-wire group was 8.75 weeks with a standard deviation of 2.0 weeks. The p-value when comparing the two groups was 0.0029 which shows statistical significance.
The graph in Figure 10 shows the mean time to pain-free function in the plate and K-wire groups with the 0.95 confidence intervals of the two groups respectively.

Figure 11 gives a graphic representation of the distribution of patients' T2 results along the expected mean value (red line).
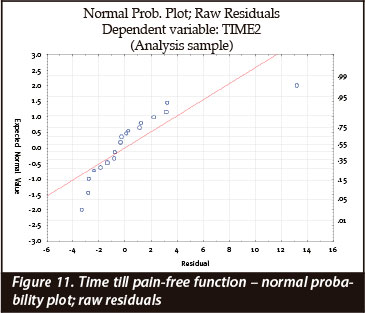
Table IV shows the different statistical methods used to test the variance of the results. The p-value is shown as 0.019 which indicates statistical significance.

The effective hypothesis decomposition of the T2 results with the current effect and p-values of the data is shown in Table V.
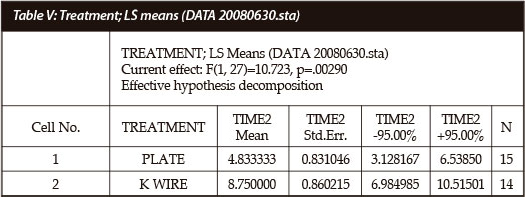
Table VI shows descriptive statistical analysis of the T2 results.

Discussion
Distal radius fractures are extremely common and intra-articular fractures make up a substantial number of these fractures.
In the displaced unstable distal intra-articular radius fractures that cannot be reduced and/or held reduced with closed reduction and pinning, volar locking plates have been shown by numerous studies to have a better outcome.
In our opinion, the other group, in which the fracture is displaced but stable, and in which closed reduction with pinning can achieve and hold a reduction, is the problem group as it is tempting to use a volar locking plate in these circumstances. This group was the target group for the study.
There are definitive limitations to this study: The study is a retrospective study and more accurate results could be generated by a prospective randomised study. The provincial database is poor; many patients are unable to be contacted; and lastly a large number of patients are non-compliant with clinic follow-up. The patient numbers were small especially in the K-wire group. The follow-up period was not adequate enough to study the long-term results of both groups.
There are studies that show that the objective outcomes of volar plates are better, but in our study we found that functional outcomes experienced by patients as shown by the DASH scores were the same in those patients treated with either closed reduction and pinning and those treated with locking plates. The objective outcomes between the two groups were similar as shown by the Gartland-Werely scores and the grip, pinch grip and key grip measurements.
The objective complication rates were higher in the pinning group and these were mainly residual dorsal angulation deformities on radiographs and asymptomatic DRUJ instabilities.
The main finding in this study was that patients treated with volar locking plates did return to pain-free independence 6 weeks (4.4 weeks if the two outlying patients' data are included in the calculation) earlier than those treated with closed reduction and pinning. We think this is an extremely relevant finding and could be used as a clinical tool by the surgeon to decide on the method of treatment for each patient group.
It is our opinion that highly functioning patients, especially office workers and also those patients who have a poor support system such as single mothers, elderly patients and homeless individuals, would benefit from locking plate fixation with the advantage of early return to independent function. On the other hand we suggest that patients who have a good support system or those that can afford time off work can be treated with less expensive implants with equal functional outcomes.
Conclusion
Unstable intra-articular radius fractures that cannot be reduced or held reduced with pinning should be treated with a locking plate system. Distal radius fractures that can be reduced and held reduced with closed reduction and pinning have been shown by this study to have equal functional outcomes compared to those treated with volar locking plates. The time to pain-free independent function was a secondary objective but proved to be an important result.
The patients treated with volar locking plates returned to pain-free independent function 6 weeks earlier than those treated with closed reduction and pinning.
Long-term, large patient number studies on this subject are recommended.
This study is the author's authentic idea and work and unless otherwise stated or referenced the format, text, tables and pictures are his own creation.
No benefits of any form have been received by the author or supervisor from a commercial party related directly or indirectly to the subject of this study.
References
1. Colles A. Historical paper on the fracture of the carpal extremity of the radius (1814). Injury 1970;2:48-50. [ Links ]
2. Fernandez DL, Geissler WB: Treatment of displaced articular fractures of the radius. J Hand Surg [Am] 1991;16:375-84. [ Links ]
3. Jupiter JB. Complex articular fractures of the distal radius: classification and management. J Am Acad Orthop Surg 1997;5:119-29. [ Links ]
4. Leung KS, Shen WY, Tsang HK, Chiu KH, Leung PC, Hung LK. An effective treatment of comminuted fractures of the distal radius. J Hand Surg 1990;15A:11-17. [ Links ]
5. Chapman MW. Chapmans Orthopaedic Surgery. Lippincott Williams and Wilkins Third edition 2001;1413-34. [ Links ]
6. Cooney WP III, Linscheid RL, Dobyns JH. External pin fixation of unstable Colles' fractures. J Bone Joint Surg 1979;61A:840-45. [ Links ]
7. Green DP, ed. Operative hand surgery. 5th ed. Philadelphia: Elsevier Churchill Livingstone, 2005:645-70. [ Links ]
8. Moore KL, Dalley AF. Clinical orientated anatomy. Lippincott Williams and Wilkins Fourth edition 1999; 773-830. [ Links ]
9. Nana AD, Joshi A, Lichtman DM. Plating of the distal radius. J Am Acad Orthop Surg 2005;13:159-71. [ Links ]
10. Carlos Rodrigues-Merchan E. Plaster cast versus percutaneous pin fixation for comminuted fractures of the distal radius in patients between 46 and 65 years of age. J Orthop Trauma 1997;11(3):212-27. [ Links ]
11. Carter PR, Frederick HA, Laseter GF. Open reduction and internal fixation of unstable distal radius fractures with a low profile plate: a multicenter study of 73 fractures. Journal of Hand Surgery 1998;23A:300-307. [ Links ]
12. Fuller DA, Barrett M, Marburger RK , Hirsch R. Carpal canal pressures after volar plating of distal radius fractures. Journal of Hand Surgery (British and European Volume, 2006) 31B(2):236-39. [ Links ]
13. Kirk JL, Jupiter JB. Intra-articular fractures of the distal end of the radius in young adults. J Bone Joint Surg [Am]. 1986;68(5):647-59). [ Links ]
14. Anzarut A, Johnson J, Rowe B, Lambert R, Blitz S, Majumdar S. Radiologic and patient-reported functional outcomes in an elderly cohort with conservatively treated distal radius fractures. J Hand Surg 2004;29A:1121-27. [ Links ]
15. Clancey G. Percutaneous Kirschner-wire fixation of Colles' fractures. J Bone Joint Surg (Am) 1984;66-A(7):1008-14. [ Links ]
16. Gupta M, Anil Reheja M, Umesh Godi M. Colles' fracture: management by percutaneous crossed-pin fixation versus Plaster of Paris cast immobilisation. Orthopaedics 1999;22(7):680-82. [ Links ]
17. Trumble TE et al. Intrafocal (Kapandji) pinning of distal radius fractures with and without external fixation. J. Hand Surg. 1998;23-A(3)(May):381. [ Links ]
18. Grewal R, Perey B, Wilmink M, Stothers K. Randomized prospective study on the treatment of intra-articular distal radius fractures: open reduction and internal fixation with dorsal plating versus mini open reduction, percutaneous fixation, and external fixation. J Hand Surg 2005;30A:764-72. [ Links ]
19. McQueen MM, Michie M, Court-Brown CM. Hand and wrist function after external fixation of unstable distal radial fractures. Clin Orthop 1992;285:200-204. [ Links ]
20. Rikli DA, Kupfer K, Bodoky A. Long-term results of the external fixation of distal radius fractures. J Trauma 1998;44:970-76. [ Links ]
21. David S, Ruch D, Papadonikolakis A. Volar versus dorsal plating in the management of intra-articular distal radius fractures. J Hand Surg 2006;31A:9-16. [ Links ]
22. Kamano M, Koshimune M, Toyama M, Kazuki K. Palmar plating system for Colles' fractures - a preliminary report. J Hand Surg 2005;30A:750-55. [ Links ]
23. Koshimune M, Kamano M, Takamatsu K, Ohashi H. A randomized comparison of locking and non-locking palmar plating for unstable Colles' fractures in the elderly. J Hand Surg (British and European Volume, 2005) 30B(5):499-503. [ Links ]
24. Musgrave DS, Idler RS. Volar fixation of dorsally displaced distal radius fractures using the 2.4-mm locking compression plates. J Hand Surg 2005;30A:743-49. [ Links ]
25. Trease C, McIff T, Toby B. Locking versus nonlocking t-plates for dorsal and volar fixation of dorsally comminuted distal radius fractures: a biomechanical study. J Hand Surg 2005;30A:756-63. [ Links ]
26. Cole D, Elsaidi G, Kuzma K, Kuzma G, Smith B, Ruch D. Distal radioulnar joint instability in distal radius fractures: The role of sigmoid notch and triangular fibrocartilage complex revisited. Int. J. Care Injured 2006;37:252-58. [ Links ]
27. Rozental T, Blazar P. Functional outcome and complications after volar plating for dorsally displaced,unstable fractures of the distal radius. J Hand Surg 2006;31A:359-65. [ Links ]
28. Atroshi I, Gummesson C, Andersson B, Dahlgren E, Johansson A. The disabilities of the arm, shoulder and hand (DASH) outcome questionnaire. Reliability and validity of the Swedish version evaluated in 176 patients. Acta Orthop Scand 2000;71(6):613-18. [ Links ]
29. Gartland JJ, Werley CW. Evaluation of healed Colles' fractures. J Bone J Surg 1951;33-A:895-907. [ Links ]
30. Dunn OJ, Clarke VJ (1987): Applied Statistics: Analysis of Variance and Regression.1987 (2nd Ed.) John Wiley and Sons, New York. [ Links ]
31. StatSoft Inc. (2007) STATISTICA (data analysis software system), version 8. www.statsoft.com [ Links ]
 Reprint requests:
Reprint requests:
Dr Matthew Durrans
Department of Orthopaedic Surgery Tygerberg Hospital
Cape Town, South Africa
Tel: 021-9384911
Email: mattdurrans@capeboneandjoint.com


{kind=link}
{kind=link}
{kind=link}