










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSA Orthopaedic Journal
On-line version ISSN 2309-8309
Print version ISSN 1681-150X
SA orthop. j. vol.12 n.1 Centurion Jan. 2013
BASIC SCIENCE
Controversies around modern bearing surfaces in total joint replacement surgery
PB OosthuizenI; CH SnyckersII
IMBChB. Senior Registrar. Department of Orthopaedic Surgery, University of Pretoria
IIMBChB, Dip PEC(SA), MMed(Orth), FCSA(Orth). Consultant in Arthroplasty. Department of Orthopaedic Surgery, University of Pretoria
ABSTRACT
Patients in need of total hip or knee arthroplasty are continuously getting younger which produce the need for bearing surfaces that can withstand both the high functional demand as well as the longevity of the patient. New developments are continuously flooding the market and the promotion of these products is directed towards patients themselves who, most of the time, will not have the necessary insight to choose the best possible product. Due to recent introduction into the market, these products all lack long-term independent clinical follow-up, but all have promising results in manufacturer-funded, short-term clinical trials and laboratory simulator trials. This leaves the surgeon with the dilemma of using new untested technology with potentially devastating results or keeping to the tried and trusted. Technological advances in bearing surfaces include modifications of known materials and the introduction of totally new materials, all in an attempt to find the perfect bearing coupling. This paper summarises the most important new developments in bearing surfaces and bearing couples in arthroplasty and puts emphasis on the dangers of using untested technology.
Key words: bearing surfaces, arthroplasty, clinical evidence, new technology
Introduction
It is common practice for company representatives to provide orthopedic surgeons with the latest technology in arthroplasty, often as their standard product. Most of these products lack adequate supportive literature and can therefore be considered experimental. Furthermore, it is commonplace for commercial 'research' that almost invariably has short follow-ups and small patient numbers, to be not only biased, but also statistically entirely unconvincing.
In the light of the recent problems with metal-on-metal bearing couplings it is certainly now time to question the efficacy and more importantly, the safety of every new implant that is introduced into the arthroplasty market. Companies develop their own minor modifications to basic principles in order to overcome copyright laws of pioneers in the industry. Even if the original technology has good long-term clinical data to support its efficacy, it does not imply that the modifications of these products will be as safe or effective as the original product.
Unfortunately, the surgeon is faced with a young, highly demanding and well-informed patient who demands a product that can withstand his or her needs. The dilemma is whether the surgeon should use 'safe' older, clinically validated technology when the newer technologies that possibly have improved outcomes, but potentially harmful side effects, are available.
This article summarises available bearing surface technology and emphasises their shortcomings.
Background
Multiple bearing surfaces were experimented with in the early history of hip arthroplasty. Boutin reported on the use of ceramics as a bearing surface in 1970.1 With the introduction of low friction arthroplasty using metal on polyethylene (PE), Sir John Charnley developed a reproducible and safe bearing couple for total hip arthroplasty (THA).2 Following these reports of 92% survival at seven years the development of total knee arthroplasty also adopted metal-on-PE as the standard bearing coupling. This bearing relies on cobalt chrome metal inlays articulating with standard PE.
- Although this bearing coupling has proven itself clinically over the years,2-4 there remain concerns about wear rates and particle creation in vivo over time. Sochart et al examined non-crosslinked PE wear of cemented sockets in patients younger than 30 years of age. At 19.5-year follow-up, the mean total linear wear averaged 2.1 mm (mean 0.12 mm/year).5
- For patients with PE linear wear rates less than 0.1 mm per year, the 25-year survivorship was 90%. In contrast, in those patients with a linear wear rate that exceeded 0.2 mm/year the survivorship was less than 30% at 20 years.5 The search continues for bearing materials with maximum wear potential. Our choice today is still limited to combinations of PE, metal and ceramics, in standard or modified form.
Polyethylene (PE)
The Australian Hip Registry noted in their annual report of 2010 that there has been increasing use of modified PE. The use of this material has been associated with a reduction in the risk of revision in primary total conventional hip replacement.6
Crosslinked PE has earned its place in arthroplasty with adequate clinical trials to warrant its use with confidence.7-11 This process of low radiation crosslinking was started in South Africa by Grobbelaar and co-workers who recently published the longest follow-up to date on crosslinked PE in THA. They reported a seven to eight times reduction in PE wear over a mean of 20 years. It has been shown in that series and various literature reports that up to 1 mm socket wear is acceptable. Thereafter the failure rate increases rapidly due to pain, interface failure and osteolysis. In the non-crosslinked PE form, this will take place in approximately ten years, but after crosslinking, the socket life expectancy is increased seven- to eight-fold. This confirms the absolute importance of PE crosslinking in total joint arthroplasty.11
The theoretical risk of fatigue cracking in melted HXLPE and in vivo oxidation of annealed HXLPE fuelled the latest modifications of HXLPE.12 These include antioxidant diffusion, mechanical deformation or sequential low dose irradiation with interspersed annealing. Collectively, these modifications show improved simulated wear, oxidation and mechanical strength compared to earlier HXLPE components. It is however important to realise that companies use the clinical data of their original HXLPE equivalents, combined with simulator data of recent modifications, as the foundation for motivating a good predicted outcome.
Locally the longest clinical follow-up of later modifications to HXLPE was presented by Dr Cakic at the 2010 South African Orthopaedic Congress in Port Elizabeth which showed 0.031 mm/year wear rate over 10 years and no measureable wear after 6 million cycles in simulator testing of inhomogeneous crosslinked PE (Gammalink Medical©).13
Table I summarises some of the new modifications of PE and is derived from data supplied by the industry. It puts emphasis on the short follow-up times and small sample sizes typically associated with commercial research. The five-year follow-up in 51 patients used for Stryker X3 poly as well as the three patients in seven years used for Biomet E-poly is not convincing enough to support the use of these products. Futhermore, work by Grobbelaar et al shows that irradiation doses of 50 KGy and 75 KGy used in ArcomXL and AOX respectively is unlikely to cause any significant crosslinking.14 According to the same author at least 100-140 KGy is required and if a company decides to deviate significantly from world experience, it should provide clinically significant data to support its methods.15-17 The data supporting these products is therefore statistically unconvincing, and the products can be considered experimental.
Metal
Cobalt alloys are being produced with newer modern techniques such as mould inoculation, forging and hot iso-static pressing which greatly reduce the shortcomings of cast cobalt-chrome. Cobalt-chrome overall has excellent wear and corrosion resistance, acceptable biocompatibility and generally satisfactory fatigue life.26,27
Latest advances now aim towards changing the surface of the metal component in order to achieve improved wear rates and fewer complications associated with metal debris. These include ceramified metals, ceramic coatings and ion treatments of the metal surfaces. Again these surfaces show promising results in simulator and early clinical trials, but still lack long-term clinical follow-up.
Oxidised zirconium (Smith and Nephew Oxinium®, 1995) is a zirconium implant where only the surface of the implant is ceramified. The Oxinium® surface theoretically provides abrasion and wear characteristics of ceramic components while the metal core provides mechanical characteristics of cobalt-chrome components.28-30 It is a concern that zirconia (zirconium dioxide) ceramics failed in earlier implants. The failure mechanism was related to the metastable behaviour of the tetragonal phase transforming under certain conditions to monoclinic phase and thereby causing the grains to swell and push-out while weakening the structural integrity. Hohls recently published a dissertation on 27 retrieved yttria-stabilised tetragonal zirconia cups after an average of 10.3 in vivo years. He showed an average of 53.6% monoclinic phase zirconia.31 The ceramic surface in Oxinium® devices is formed directly in the mon-oclinic phase and is theoretically not subject to metastable phase transformations and subsequent weakening. The company did announce a voluntary recall of all cementless knee implants utilising Oxinium® in 2003 which does raise a concern despite the reason for failure not being related to the bearing surface. Although the Australian Joint Registry of 2011 reported the lowest revision rates (2.2%) for the Oxinium® on HXLPE combination in hips, this was only over seven years in 238 patients. This is low volume, short-duration data and the same principles are applicable to the products as those listed in Table I.
Titanium-niobium-nitride ceramic-coated implants (Werkomed®, Biomet®, 2003) are another example of a metal surface modification. It is a micro-ceramic applied by a process of plasma vapour deposition on a cobalt-chrome-molybdenum prosthesis. The theory is to minimise metal particulate wear, prevent corrosion and to prevent metal ion release. Hamelynck and Woering summarised two-to-seven year clinical results motivating all these characteristics, but with only one patient at seven-year follow-up.32 In vitro studies also quoted in this article showed no delamination at 5 million cycles. No significant long-term trials with adequate patient numbers and implant years could however be found in the literature, which again makes this technology unproven and therefore experimental.
Low Friction Ion Treatment (LFIT) (Stryker® 1991) is also a metal surface modification where nitrogen ions are embedded into the metal surface under high energy. This theoretically increases wettability, improves lubrication and decreases wear. Clinical data is available only in 55 hips over a minimum of three years showing a 28% reduction in wear rates with LFIT femoral heads.33
Ceramic
Ceramic is an inorganic, non-metallic solid which is usually manufactured by oxidising metal and heating it to extreme temperatures. Ceramtec® is the company that supplies more than 80% of all the ceramic components to all the companies worldwide. Therefore, most companies have exactly the same ceramic technology. Proven efficacy with third generation alumina (aluminium oxide) ceramics is available in the literature,34,35 but the small risk of complications associated with this bearing triggered the development of fourth generation Delta® ceramic components.
The latest technology from Ceramtec is Biolox Delta® ceramic, a fourth generation ceramic.
- Biolox Delta® (2003)36
Biolox Delta® is an aluminum oxide matrix composite ceramic consisting of 75% alumina, 24% zirconia (ZrO2) and other trace elements.
Alumina ceramic provides the material's hardness and wear resistance, while zirconia, together with other additives, provides improved mechanical properties by counteracting crack formation and propagation.
The most significant improvement with the development of Biolox Delta® was the improved mechanical strength that allows manufacturing of component geometries that were not previously possible. These include ceramic knee components and thinner acetabular cups which provide the surgeon with much-needed stability when performing THA in the young active patient.
Clinical data is limited to short- and medium-term follow-up and is comparable to results of third generation alumina ceramics. Lombardi et al performed a prospective, randomised, US FDA investigational device exemption study on 44 patients using Delta ceramic femoral heads on alumina acetabular cups and compared it to a control group using alumina femoral heads on PE liners. The mean follow-up was six years and both groups performed equally.37
Hamilton et al recently published a prospective, randomised, multicentre trial on the early results of 264 hips using Delta ceramic components which showed 97% survivorship at 3.2-year follow-up.38
It is disturbing that, despite this short-term, small-sample size literature, Ceramtec® has sold 1.6 million ball heads and 700 000 liners worldwide since the launch of Biolox Delta®.
Advanced bearing couples
Classification
- Hard-on-soft bearing couples:
Metal on highly crosslinked PE
Ceramic on highly crosslinked PE
- Hard-on-hard bearing couples:
Metal-on-metal
Ceramic-on-ceramic
Hard-on-soft bearing couples
Metal on highly crosslinked polyethylene
Due to the significant difference in the manufacturing methods of all the new PE components it would be ideal to evaluate the performance of each component separately. It is unfortunately very difficult to obtain this in vivo, but in vitro data for each specific component does exist.
The big advantage of simulator studies is that it enables one to evaluate different components under exactly the same conditions, thereby removing all variables that could influence outcomes. The problem however with available simulator data is that not all companies test their products in a standardised fashion. Most of these studies differ in sample size, number of cycles, gait variability, presence of third-body wear and also the type of simulator used.
Before evaluating clinical data it is important to take note that osteolysis, loosening and revision rates are the dictating factors of a successful bearing and not only linear penetration or wear rates. Long-term clinical data clearly show that there remains a large difference between simulator data and clinical outcomes and retrieval studies, reflecting the multiple variables that exist in a biological system.
Collectively, all the laboratory simulator studies of the various companies showed drastically better results with regard to with delamination, wear and mechanical strength with highly crosslinked PE liners compared to conventional UHMWPE liners. The companies that compared modified HXLPE to standard highly crosslinked PE inserts also found significant reduction in wear and improvement in mechanical strength of the modified HXLPE inserts.39
Not many clinical studies are available that compare HXLPE to conventional PE. Kuzyk et al did a meta-analy-sis of randomised control trials of crosslinked versus conventional PE for total hip replacement (THR) over the past decade and found 12 studies in their inclusion criteria. They concluded that crosslinked PE liners had reduced radiological wear and osteolysis at a mean follow-up of 5.1 years, but there was no difference in revision rates between crosslinked and conventional PE liners. No early failures attributable to brittleness of the crosslinked PE were reported.40
Kurtz et al in their review identified two level 1 articles showing significant reduction in wear over a 7.2-year period that showed encouraging results with the use of crosslinked PE. They did however conclude that definite results await long-term follow-up.41
Grobbelaar et al recently published results of a cohort of patients with the longest follow-up on crosslinked PE. They reported a seven to eight times improvement in PE wear as well as 16 patients with post-arthroplasty improvement of the interface.11
In total knee replacement, Hodrick and Minoda both found no significant difference in clinical or radiographic outcome after six- and two-year follow-ups respectively. Both studies had good sample sizes of cruciate retaining and sparing primary knee arthroplasty with similar components in the conventional PE and HXLPE groups.42,43
Concern about the particle size and the dissemination of these particles with unknown effects has been raised, but it is still surrounded with controversy in the literature.39
Although the short-term clinical data on crosslinked PE is encouraging, only long-term studies truly take the patient and material-related factors into consideration when assessing any superiority of crosslinked PE over conventional PE liners. This is especially applicable when the main aim is to prove longevity in a young active patient.
Ceramic on highly crosslinked polyethylene
Ceramic bearings have tribologic advantages over metal bearings and result in lower wear and osteolysis rates. The main drawback of ceramic components is however the risk for fracture which, up to recently, limited the use of ceramic components mostly to hip implants and smaller femoral heads due to the need for thick acetabular components. It is these mechanical properties that led to the development of fourth generation ceramics, ceramified metals and ceramic surface coatings.
Clinical data:
- Kim et al recently reported on 73 consecutive hips using alumina on highly crosslinked PE. All patients were younger than 50 years of age with an average of 47 years. Mean follow-up was 8.5 years. Results showed no osteolysis or aseptic loosening using X-ray and CT scan.44
- Verilast® Technology is Smith and Nephew's trademark for the Oxinium®-HXLPE bearing couple. Knee simulator results of Verilast® technology showed an 81% reduction in mean volumetric wear and implant longevity of up to 30 years. These results are however inadequate to predict quantative wear results in vivo.45 The Australian joint registry did however show in their 2011 annual report that Verilast technology in THR surgery showed only 2.2% revision rate at seven years in 238 implants.
- Garvin et al reported on 56 THAs in a young, active patient population using oxidised zirconium on HXLPE. No patient had radiographic evidence of osteolysis and no patient had been revised for mechanical loosening or wear at an average of 30 months.46
- Wroblewski et al did a prospective clinical trial on 19 hips using 22 mm heads, showing an average of 0.022 mm annual wear rate in vivo and similar results in a simulator study. These results proved significantly lower wear rates than in UHMWPE and the value of a well-designed joint simulator.8
- Oonishi et al reported on clinical experience with ceramics in THR surgery and showed that alumina ceramics decreased wear compared to metal heads when combined with UHMWPE, but had similar wear rates as metal heads when crosslinked PE was used.47
- Hui et al showed in a prospective randomised control trial that there is no clinical, radiographic or subjective difference in 40 consecutive patients who received bilateral cruciate-retaining total knee arthroplasty. One knee was done using Oxinium® femoral components and the contralateral knee was done using cobalt-chromium components, both on highly crosslinked PE. There were also no adverse effects when using Oxinium® components. This study was done at only five-year follow-up, and longer-term follow-up is necessary to better evaluate the performance of oxinium.48
Hard-on-hard bearing couples
Metal-on-metal
Poor manufacturing techniques and excellent results with metal on UHMWPE caused metal-on-metal couplings to fall out of favour in the 1980s. In 1988, Müller and Weber introduced the first second generation chromium-cobalt alloy bearing under the brand name Metasul®. To date more than 140 000 units have been inserted.49 The most important difference is the improved manufacturing techniques used and this technology is now applied in resurfacing systems as well. These successes led to raised interest in the metal-on-metal bearing coupling.
After Du Puy® launched their ASR® metal-on-metal system in 2003 the early clinical results provided by the manufacturer were promising. O'Sullivan did a single surgeon prospective analysis on 340 consecutive hips with only three neck of femur fractures and one wound infection after an average of three years' follow-up. Data on file at Du Puy® indicated a 2.2% revision rate in 1 200 implants at two years. Cobb reported a three-year cumulative survival rate for all patients and all components of 97.4% in 1 030 patients. All these abovementioned studies are however unpublished and unobtainable data which was supplied on request from Du Puy South Africa.
Despite these excellent early results the ASR® ended up being recalled after devastating outcomes. The Australian Hip Registry concluded in its October 2010 annual report that the metal-on-metal bearing surfaces do not appear to be doing as well as the other bearing surfaces. This difference however was only apparent when the femoral head size used is larger than 32 mm.6 The British Hip Society released the following statement after their 2012 annual meeting:50
- Stemmed, large diameter metal-on-metal primary THRs using bearings of 36 mm or above should no longer be performed until more evidence is available, except in properly conducted and ethically approved research studies.
- This advice does not apply to hip resurfacing.
- Patients who already have metal-on-metal bearing implants should be followed up.
- The British Hip Society will continue to monitor the latest research in this field and will provide further guidance once more information becomes available.
Ceramic-on-ceramic
Ceramics are one of the most significant advances in total hip and recently total knee replacement surgery. Technological advances in manufacturing techniques are now enabling the manufacture of implants with geometries that were not possible previously.
The two most important concerns with ceramics are mechanical strength and bearing noise. Until recently the brittleness of ceramics limited their use to THR surgery, but still with a risk of fracturing (0.004%) and dislocation due to small head sizes in thick acetabular components.51 With the new Delta ceramics, companies can now manufacture not only thin acetabular cups with large femoral heads, but also knee surface components.
Bearing noise is a potential problem with an incidence ranging from 0.48% to 10%. The significance of squeaking remains unknown with no evidence to suggest that squeaking is a warning for implant failure.52 Stafford et al performed a retrospective analysis of 250 ceramic-on-ceramic hip replacements in a young group of patients in a single centre over 59 months. No patients reported squeaking or radiological evidence of osteolysis or migration of the components. They noted that surgical technique and implant placement was extremely important. The total revision rate was 2.4% with half of them being for impingement-related problems and only one for ceramic fracture.53
Petsatodis et al retrospectively analysed 85 first generation alumina-on-alumina THAs in young patients and found a survival rate of 84.4% after 20 years. Six hips in this study needed revision and all were for aseptic loosening. Not one case of bearing noise or fracture was reported. These fairly good results were achieved with old ceramic technology which provides a promising future for ceramic bearings.54
Recently Lee et al reported a 99% survival rate for any cause after ten-year follow-up with third generation ceramics in 86 patients. Two of their patients needed a change of the ceramic heads after fracture and 13 reported episodes of bearing noise. They concluded that excellent results are obtainable with this bearing surface but patients need to be counselled about the risk for fracture and bearing noise.55
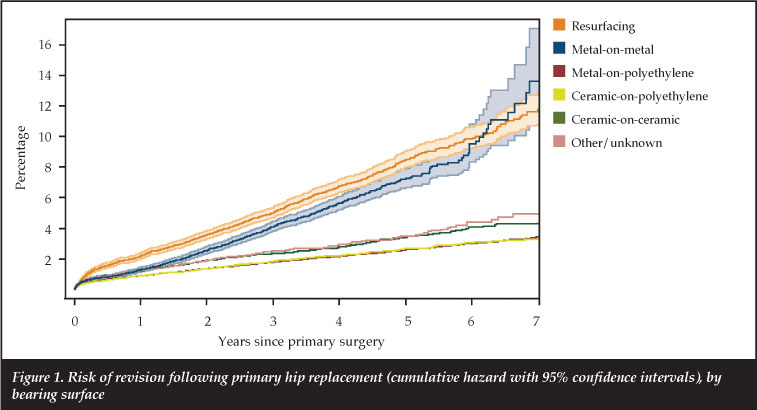
The above graph (Figure 1) obtained from the National Joint registry for England and Wales however show minimally higher revision rates for ceramic-on-ceramic bearing surfaces than ceramic-on-PE, but with metal-on-PE remaining the best performing combination with regard to with revision rates.56
Conclusion
The development of cutting edge technology in bearing surfaces is driven by the quest to find the ideal bearing couple that can withstand the demand of the young active patient in need of total joint arthroplasty. These patients are continuously getting younger with increased demand. We are in the midst of an information-driven society and companies are using 'direct-to-patient' marketing strategies to promote their products. It is therefore of utmost importance that the arthroplasty surgeon is familiar with new developments in order to guide patients in the right direction to avoid sales gimmicks and rather base decisions on evidence.
However, the rate of new developments is faster than the rate at which we can perform adequate long-term follow-up clinical trials. This leaves us with the situation where we have to choose between using evidence-based 'old' technology when potentially better implants are available, or using new technology with the risk of devastating results.
Furthermore, new technology costs money which ultimately comes from the patient's pocket. Society demands value for money and this is now enforceable by the Consumer Protection Act which has an effect on everybody in the supply chain including the surgeon. We simply do not have the evidence to justify massive expenditure on advanced implants without clinical data supporting their improved outcome compared to traditional bearing surfaces.
The content of this article is the sole work of the authors. No benefits of any form have been received from a commercial party related directly or indirectly to the subject of this article.
References
1. Boutin P. Total hip arthroplasty using a ceramic prosthesis. Pierre Boutin (1924-1989). Clinical Orthopaedics & Related Research 2000 Oct(379):3-11. [ Links ]
2. Charnley J. The long-term results of low-friction arthroplasty of the hip performed as a primary intervention. Journal of Bone & Joint Surgery - British Volume 1972 Feb;54(1):61-76. [ Links ]
3. Callaghan JJ, Albright JC, Goetz DD, Olejniczak JP, Johnston RC. Charnley total hip arthroplasty with cement. Minimum twenty-five-year follow-up. Journal of Bone & Joint Surgery - American Volume 2000 Apr;82(4):487-97. [ Links ]
4. Berry DJ, Harmsen WS, Cabanela ME, Morrey BF. Twenty-five-year survivorship of two thousand consecutive primary Charnley total hip replacements: factors affecting survivorship of acetabular and femoral components. Journal of Bone & Joint Surgery - American Volume 2002 Feb;84-A(2):171-77. [ Links ]
5. Sochart DH, Porter ML. Long-term results of cemented Charnley low-friction arthroplasty in patients aged less than 30 years. J.Arthroplasty 1998 Feb;13(2):123-31. [ Links ]
6. Australian Orthopedic Association. Australian National Joint replacement Registry: 2010 Annual Report. 2010; Available at: http://www.dmac.ade-laide.edu.au/aoanjrr/publications.jsp?section=reports2010. Accessed 6/11, 2012. [ Links ]
7. Jacobs CA, Christensen CP, Greenwald AS, McKellop H. Clinical performance of highly cross-linked polyethylenes in total hip arthroplasty. Journal of Bone & Joint Surgery - American Volume 2007 Dec;89(12):2779-86. [ Links ]
8. Wroblewski BM, Siney PD, Dowson D, Collins SN. Prospective clinical and joint simulator studies of a new total hip arthroplasty using alumina ceramic heads and cross-linked polyethylene cups. Journal of Bone & Joint Surgery - British Volume 1996 Mar;78(2):280-85. [ Links ]
9. Oonishi H, Kim SC, Takao Y, Kyomoto M, Iwamoto M, Ueno M. Wear of highly cross-linked polyethylene acetabular cup in Japan. J.Arthroplasty 2006 Oct;21(7):944-49. [ Links ]
10. Oonishi H, Kadoya Y, Masuda S. Gamma-irradiated cross-linked polyethylene in total hip replacements-analysis of retrieved sockets after long-term implantation. J.Biomed.Mater.Res. 2001;58(2):167-71. [ Links ]
11. Grobbelaar CJ, FA Weber FA, du Plessis TA. Thirty three years of clinical experience with crosslinking of polyethylene in cemented total hip replace ment. SA orthop. j. 2011 Autumn;10(1). [ Links ]
12. Dumbleton JH, D'Antonio JA, Manley MT, Capello WN, Wang A. The basis for a second-generation highly cross-linked UHMWPE. Clinical Orthopaedics & Related Research 2006 Dec;453:265-271. [ Links ]
13. Cakic JN. South African experience with cross-linked ultrahigh molecular weight polyethylene in total hip arthroplasty. Ph.D.,Dept. of Orthopaedic Surgery, Faculty of Health Sciences, University of the Witwatersrand, 2009. 2009-10-21T09: 57:50Z (http://hdl.handle.net/10539/7382). [ Links ]
14. Grobbelaar CJ, du Plessis TA, Marais F. The radiation improvement of polyethylene prostheses. A preliminary study. Journal of Bone & Joint Surgery - British Volume 1978 Aug;60-B(3):370-74. [ Links ]
15. Asano T, Akagi M, Clarke IC, Masuda S, Ishii T, Nakamura T. Dose effects of cross-linking polyethylene for total knee arthroplasty on wear performance and mechanical properties. Journal of Biomedical Materials Research. Part B, Applied Biomaterials 2007;83(2):615-22. [ Links ]
16. Muratoglu OK, Bragdon CR, O'Connor DO, Jasty M, Harris WH, Gul R, et al. Unified wear model for highly crosslinked ultra-high molecular weight polyethylenes (UHMWPE). Biomaterials 1999 Aug;20(16):1463-70. [ Links ]
17. Oonishi H, Kadoya Y. Wear of high-dose gamma-irradiated polyethylene in total hip replacements. Journal of Orthopaedic Science 2000;5(3):223-28. [ Links ]
18. Stryker. Stryker X3 Bearing Technology. 2010; Available at: http://www.stryker.com/en-us/products/Orthopaedics/HipReplacement/PrimaryAcetabular/Polyethylene/ PolyethyleneX3/index.htm. Accessed 6/11, 2012. [ Links ]
19. D"Antonio JA, Capello WN, Ramakrishnan R. Second-generation Annealed Highly Cross-linked Polyethylene Exhibits Low Wear. Clin Orthop Relat Res 2012;470(6):1696-1696 - 1704. [ Links ]
20. Muratoglu OK, Bragdon CR, O'Connor D, Perinchief RS, Estok DM, 2nd, Jasty M, et al. Larger diameter femoral heads used in conjunction with a highly cross-linked ultra-high molecular weight polyethylene: a new concept. J.Arthroplasty 2001 Dec;16(8 Suppl 1):24-30. [ Links ]
21. Muratoglu OK, Bragdon CR, O'Connor DO, Jasty M, Harris WH. A novel method of cross-linking ultra-high-molecular-weight polyethylene to improve wear, reduce oxidation, and retain mechanical properties. Recipient of the 1999 HAP Paul Award. J.Arthroplasty 2001 Feb; 16(2):149-60. [ Links ]
22. Oral E, Muratoglu OK. Vitamin E diffused, highly crosslinked UHMWPE: a review. Int.Orthop. 2011 Feb;35(2):215-23. [ Links ]
23. Jarrett BT, Cofske J, Rosenberg AE, Oral E, Muratoglu O, Malchau H. In vivo biological response to vitamin E and vitamin-E-doped polyethylene. Journal of Bone & Joint Surgery - American Volume 2010 Nov 17;92(16):2672-81. [ Links ]
24. Biomet. ArCom XL® Highly Crosslinked Polyethylene. 2012; Available at: http://www.biomet.com/orthopedics/productDetail.cfm?category=2&product=211. Accessed 6/11, 2012. [ Links ]
25. DePuy Orthopaedics I. Altrx: Altra-linked polyethylene; a better alternative. 2008; Available at: http://www.bizwan.com/_mydoc/depuy/hiptech/DPY_AltrX_Brochure_0612-77-506_rev1.pdf. Accessed 6/11, 2012. [ Links ]
26. Grubl A, Marker M, Brodner W, Giurea A, Heinze G, Meisinger V, et al. Long-term follow-up of metal-on-metal total hip replacement. Journal of Orthopaedic Research 2007 Jul;25(7):841-48. [ Links ]
27. Eswaramoorthy V, Moonot P, Kalairajah Y, Biant LC, Field RE. The Metasul metal-on-metal articulation in primary total hip replacement: clinical and radiological results at ten years. Journal of Bone & Joint Surgery -British Volume 2008 Oct;90(10):1278-1283. [ Links ]
28. Smith and Nephew. Oxinium. 2012; Available at: http://global.smith-nephew.com/us/OXINIUM_URGEON_INFO_24890.htm. Accessed 6/11, 2012. [ Links ]
29. Sheth NP, Lementowski P, Hunter G, Garino JP. Clinical applications of oxidized zirconium. Journal of Surgical Orthopaedic Advances 2008;17(1):17-26. [ Links ]
30. Hallab N, Merritt K, Jacobs JJ. Metal sensitivity in patients with orthopaedic implants. Journal of Bone & Joint Surgery - American Volume 2001 Mar;83-A(3):428-36. [ Links ]
31. Hohls, AC 2010, Investigation into phase transformation of Yttria stabilized zir-conia femoral heads, MEng dissertation, University of Pretoria, Pretoria, viewed yymmdd < http://upetd.up.ac.za/thesis/available/etd-07112011-163318/E11/320/gm> [ Links ].
32. Hamelynck KJ WR. Ceramic Surface Engineered Metal-on-Metal Hips system for Total Hip Arthroplasty and Resurfacing Hip Arthroplasty. Ceramic Surface Engineered Metal-on-Metal. The design rationale, pre-clinical testing and interim report on 2- 7 years of clinical results. 2009; Available at: https://docs.google.com/viewer?a=v&q=cache:EBPtvmCYBRgJ:www.accis.nl/resources/ White%2520Paper%2520Ceramic%2520Engineering%2520by%2520Dr% 2520Hamelynck% 2520.pdf+Ceramic+Surface+Engineered+Metal-on-Metal+ Hips+system+for+Total+Hip+Arthroplasty+and+Resurfacing+Hip+ Arthroplasty .+Ceramic+Surface+Engineered+Metal-on-Metal.+The+design+rationale,+preclinical+testing+and+interim+report+on+2+7+ years+of+clinical+results&hl=en&gl=za&pid=bl&srcid=ADGEESh7eoWFW TedFx1t1Gh7AUYdES5L8Cwb 1J6IqI4YeM0RCclvIZzpUCj8kx3vkyqEbnugDj6KiYtToSpSeT2X0KggCUS8dIXL6kELV p6fP1j0wS7_KcpdwaQjmVJP8ajfdmLRsUs&sig=AHIEtbQdmpqBG405xjWS_ien8IUko-NlQ. Accessed 6/11, 2012. [ Links ]
33. Maruyama M, Capello WN, D'Antonio JA, Jaffe WL, Bierbaum BE. Effect of low-friction ion-treated femoral heads on polyethylene wear rates. Clinical Orthopaedics & Related Research 2000 Jan(370):183-91. [ Links ]
34. Lusty PJ, Tai CC, Sew-Hoy RP, Walter WL, Walter WK, Zicat BA. Third-generation alumina-on-alumina ceramic bearings in cementless total hip arthroplasty. Journal of Bone & Joint Surgery - American Volume 2007 Dec;89 (12):2676-83. [ Links ]
35. Capello WN, D'Antonio JA, Feinberg JR, Manley MT, Naughton M. Ceramic-on-ceramic total hip arthroplasty: update. J. Arthroplasty 2008 Oct;23(7 Suppl):39-43. [ Links ]
36. Ceramtec. Increased fracture strength and excellent wear properties. Biolox Delta. 2012; Available at: http://www.ceramtec.com/ceramic-materi-als/biolox/delta/. Accessed 6/11, 2012. [ Links ]
37. Lombardi AV,Jr, Berend KR, Seng BE, Clarke IC, Adams JB. Delta ceramic-on-alumina ceramic articulation in primary THA: prospective, randomized FDA-IDE study and retrieval analysis. Clinical Orthopaedics & Related Research 2010 Feb;468(2):367-74. [ Links ]
38. Hamilton WG, McAuley JP, Dennis DA, Murphy JA, Blumenfeld TJ, Politi J. THA with Delta ceramic on ceramic: results of a multicenter investiga-tional device exemption trial. Clinical Orthopaedics & Related Research 2010 Feb;468(2):358-66. [ Links ]
39. Lachiewicz PF, Geyer MR. The use of highly cross-linked polyethylene in total knee arthroplasty. J.Am.Acad.Orthop.Surg. 2011 Mar;19(3):143-51. [ Links ]
40. Kuzyk PR, Saccone M, Sprague S, Simunovic N, Bhandari M, Schemitsch EH. Cross-linked versus conventional polyethylene for total hip replacement: a meta-analysis of randomised controlled trials. Journal of Bone & Joint Surgery - British Volume 2011 May;93(5):593-600. [ Links ]
41. Kurtz S, Medel FJ, Manley M. Wear in highly crosslinked polyethylenes. Current Orthopaedics 2008 Dec;22(6):392-99. [ Links ]
42. Hodrick JT, Severson EP, McAlister DS, Dahl B, Hofmann AA. Highly crosslinked polyethylene is safe for use in total knee arthroplasty. Clinical Orthopaedics & Related Research 2008 Nov; 466(11):2806-12. [ Links ]
43. Minoda Y, Aihara M, Sakawa A, Fukuoka S, Hayakawa K, Tomita M, et al. Comparison between highly cross-linked and conventional polyethylene in total knee arthroplasty. Knee 2009 Oct;16(5):348-51. [ Links ]
44. Kim YH, Choi Y, Kim JS. Cementless total hip arthroplasty with aluminaon-highly cross-linked polyethylene bearing in young patients with femoral head osteonecrosis. J.Arthroplasty 2011 Feb;26(2):218-23. [ Links ]
45. Smith and Nephew. Verilastsntm technology for knees. 2012; Available at: http://global.smith-nephew.com/us/VERILAST_Knee_14531.htm. Accessed 6/11, 2012. [ Links ]
46. Garvin KL, Hartman CW, Mangla J, Murdoch N, Martell JM. Wear analysis in THA utilizing oxidized zirconium and crosslinked polyethylene. Clinical Orthopaedics & Related Research2009 Jan; 467(1):141-45. [ Links ]
47. Oonishi H, Wakitani S, Murata N, Saito M, Imoto K, Kim S, et al. Clinical experience with ceramics in total hip replacement. Clinical Orthopaedics & Related Research 2000 Oct(379):77-84. [ Links ]
48. Hui C, Salmon L, Maeno S, Roe J, Walsh W, Pinczewski L. Five-Year Comparison of Oxidized Zirconium and Cobalt-Chromium Femoral Components in Total Knee Arthroplasty: A Randomized Controlled Trial. J Bone Joint Surg Am. 2011 Apr;93(7):624-30. [ Links ]
49. Zimmer. Metasul, the stregth of metal on metal. 2011; Available at: http://www.zimmer.com/ctl?template=MP&template=&op=global&action=1&id=7888. Accessed 6/11, 2012. [ Links ]
50. The British Hip Society. BHS statements on Large Diameter Metal on Metal bearing Total Hip Replacements. 2012; Available at: http://www.british-hipsociety.com/MoM%20Update.htm. Accessed 6/11, 2012. [ Links ]
51. Willmann G. Ceramic femoral head retrieval data. Clinical Orthopaedics & Related Research 2000 Oct(379):22-28. [ Links ]
52. Manley MT, Sutton K. Bearings of the future for total hip arthroplasty. J.Arthroplasty2008 Oct;23(7 Suppl):47-50. [ Links ]
53. Stafford GH, Islam SU, Witt JD. Early to mid-term results of ceramic-on-ceramic total hip replacement: analysis of bearing-surface-related complications. Journal of Bone & Joint Surgery - British Volume 2011 Aug;93(8):1017-20. [ Links ]
54. Petsatodis GE, Papadopoulos PP, Papavasiliou KA, Hatzokos IG, Agathangelidis FG, Christodoulou AG. Primary cementless total hip arthroplasty with an alumina ceramic-on-ceramic bearing: results after a minimum of twenty years of follow-up. Journal of Bone & Joint Surgery -American Volume 2010 Mar;92(3):639-44. [ Links ]
55. Lee YK, Ha YC, Yoo JJ, Koo KH, Yoon KS, Kim HJ. Alumina-on-alumina total hip arthroplasty: a concise follow-up, at a minimum of ten years, of a previous report. Journal of Bone & Joint Surgery- American Volume 2010 Jul 21;92(8):1715-19. [ Links ]
56. Department of Health and Welsh Assembly Government. The NJR 8th Annual Report. 2011; Available at: http://www.njrcentre.org.uk/njr-centre/default.aspx. Accessed 6/11, 2012. [ Links ]
 Reprints requests:
Reprints requests:
beyersoost@cybersmart.co.za


{kind=link}
{kind=link}