










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSA Orthopaedic Journal
versión On-line ISSN 2309-8309
versión impresa ISSN 1681-150X
SA orthop. j. vol.11 no.4 Centurion ene. 2012
CLINICAL ARTICLE
Clinical assessment of the flexor digitorum superficialis muscle to the fifth finger -accuracy of common tests
James WM KigeraI; Alfred KatusimeII
IMBChB MMed. Department of Orthopaedics, College of Health Sciences, Makerere University, Kampala, Uganda / Orthopaedics Rehabilitation Unit, PCEA Kikuyu Hospital, Kikuyu, Kenya
IIMulago Paramedical Schools, Kampala, Uganda
ABSTRACT
INTRODUCTION: There are several tests described to determine the presence of the flexor digitorum superficialis (FDS) muscle in the fifth digit, though it is unclear which of them is most accurate. We conducted a study to determine the accuracy of three common tests.
METHODS: A prospective study was conducted comparing three common clinical tests among patients and students in a large teaching hospital in East Africa to determine their accuracy in ascertaining the presence of the FDS in the fifth digit.
RESULTS The modified test was the most accurate in detecting the FDS, followed by the new test. The most inaccurate test was the standard test.
DISCUSSION The modified test was the most accurate test and is recommended in clinical studies trying to demonstrate the FDS function to the fifth digit.
Key words: flexor digitorum superficialis, fifth digit, tests
Introduction
The flexor digitorum superficialis (FDS) is an extrinsic muscle that flexes the proximal interphalangeal joints and indirectly flexes the metacarpal phalangeal (MP) joints of the hand.1 There is variation in the FDS to the fifth digit.1-3
The absence of the FDS may influence clinical examination in injured hands.4 There are a number of clinical tests described to demonstrate the activity of this muscle; however, it is unclear which of these tests is better. We conducted a study to determine which of three common tests is better at demonstrating activity of the FDS in the fifth digit.
Methods
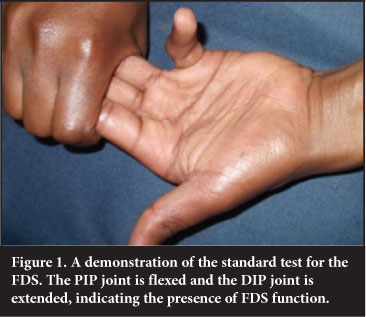
We conducted a prospective study of students of the paramedical and nursing schools and of patients attending the orthopaedic surgical outpatient clinic. Participants were randomly selected from these groups and informed of how the study would be conducted. We administered three tests to detect the presence of the FDS on the fifth digit. First the subject's hands were taken through range of motion to detect the maximum joint motion. The standard test involved allowing the fifth digit to flex while preventing flexor digitorum profundus action by preventing flexion of the interphalangeal joints of the other fingers (Figure 1). The modified test involves allowing the fifth and the fourth digits to flex together (Figure 2). The FDS is considered present if the proximal interphalangeal (PIP) joint of the fifth digit was able to flex to within 20° of maximum joint motion and the distal interphalangeal (DIP) joint was not in flexion. To confirm that the FDP was not influencing the test, the investigator ensured that the DIP was able to passively extend and flex freely. The new test was conducted by asking the participant to press the pulps of all fingers against the proximal palm (Figure 3). Extension or hyperextension of the distal interphalangeal joint with full flexion of the proximal interphalangeal joint indicates presence of the FDS while flexion of the distal interphalangeal joint was taken to indicate its absence.5


The FDS was considered absent if it was not detected by any of the tests and present if at least one test was able to demonstrate it. A test was considered to have missed detection of the FDS if it did not detect the FDS and the FDS was demonstrated by any of the other two tests. The tests were conducted by a clinical officer student (equivalent of a physician's assistant) and they were supervised by an orthopaedics resident. This was preceded by a period of training where 50 hands were examined in the presence of the resident and any errors in the method of conducting the tests were corrected.
Patients with obvious hand and wrist deformities, previous hand and wrist injuries and previous surgery to the hand and/or wrist were excluded. Participants provided written informed consent and assent was sought from the next of kin in the case of those aged below 18 years. The study was approved by the Mulago Hospital ethics board and permission was granted by the Mulago Paramedical School authorities.
Data was collected by a questionnaire and entered into Epidata program and exported to SPSS v 11.5 (SPSS Inc., Chicago, Illinois)
Results
We examined 800 subjects (1 600 hands), the majority (76.1%) of whom were students and right handed (94.4%). There were 391 (48.9%) males and 409 (51.1%) females. The subjects' ages ranged from 12 to 70 years with a mean age of 25 years.
The overall prevalence of the FDS to the fifth digit was 97.5% giving a prevalence of agenesis as 2.5%. The modified test was the most accurate, followed by the new test described by Mishra. The standard test was the least accurate (Table I).
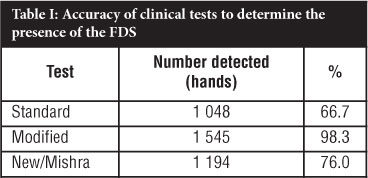
The first column indicates the different tests compared against each other. The second column shows the number of hands that had the FDS functioning that the test was able to detect and the third column indicates the percent- age.
Discussion
The modified test was the most accurate test for the demonstration of the FDS in the fifth digit. This test allows for the testing of the FDS to the fifth digit in conjunction with that of the fourth digit. This may indicate that the FDS, in a good number of cases, is functionally dependent of the FDS to the fourth digit due to anatomical connections to the FDS of that digit.3 Though there may be a possibility that the high accuracy of the modified test may be due to the effect of the FDP action, this is minimised by accurately conducting the tests. This may also represent the subjectivity of clinical tests and inter-observer variability. The use of just one investigator conducting the tests may be a weakness of the study.
Studies aiming at detecting the presence of the FDS would be more accurate were they to use the modified tests.
There are several weaknesses of the study. The lack of correlation with a radiological study (e.g. ultrasound or MRI) and the inter-observer variability are the main weaknesses. The subjectivity of the clinical tests conducted is also a weakness. Having many tests used on the same participant gives confidence that the possibility of detecting the FDS function, if present, is increased. The large number of participants is a strength because the investigators get enormous experience and skill by conducting so many examinations. The use of a training period also increases the accuracy of conducting the tests.
Conclusion
The modified test is most accurate and is recommended for the clinical testing of the FDS to the fifth digit.
Acknowledgments
We are greatly indebted to the authorities of Mulago Paramedical School for allowing us to conduct the study. We also acknowledge all study participants without who the study would not have come to fruition.
References
1. Puhaindran ME, Sebastin SJ, Lim AY, Xu WX, Chen YM. Absence of flexor digitorum superficialis tendon in the little finger is not associated with decreased grip strength. J Hand Surg Eur 2008;33:205-207. [ Links ]
2. Thompson NW, Mockford BJ, Rasheed T, Herbert KJ. Functional absence of flexor digitorum superficialis to the little finger and absence of palmaris longus - is there a link? J Hand Surg Br 2002;27:433-34. [ Links ]
3. Austin GJ, Leslie BM, Ruby LK. Variations of the flexor digitorum superficialis of the small finger. J Hand Surg Am 1989;14:262-67. [ Links ]
4. Townley WA, Swan MC, Dunn RL. Congenital absence of flexor digitorum superficialis: implications for assessment of little finger lacerations. J Hand Surg Eur 2010;35:417-18. [ Links ]
5. Mishra S. A new test for demonstrating the action of flexor digitorum superficialis (FDS) tendon. J Plast Reconstr Aesthet Surg 2006;59:1342-44. [ Links ]
 Reprint requests:
Reprint requests:
Dr JWM Kigera
PO Box 7062
Kampala Uganda
Email: jameskigera@yahoo.co.uk

