










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSA Orthopaedic Journal
On-line version ISSN 2309-8309
Print version ISSN 1681-150X
SA orthop. j. vol.11 n.3 Centurion Jan. 2012
CASE REPORT AND REVIEW OF THE LITERATURE
The contralateral hip in SCFE: prophylactic pinning complicated by a subtrochanteric fracture
UNF UkundaI; GB FirthII; AJF RobertsonIII
IMD (L'shi), FC(Ortho)(SA) Division of Orthopaedics, University of the Witwatersrand
IIMBBCh, (Orth), MMed(Orth)(Rand) Division of Orthopaedics, University of the Witwatersrand
IIIMBBCh(Wits) MMed(Orth)(Wits) Division of Orthopaedics, University of the Witwatersrand
ABSTRACT
The management of the contralateral unaffected hip in the unilateral slipped capital femoral epiphysis (SCFE) remains controversial. This is a report of two cases of subtrochanteric femoral fracture following prophylactic pinning. These two cases illustrate that prophylactic pinning is not devoid of complications as the literature might suggest, and should be highlighted as a potential post-operative complication.
Key words: SCFE, contralateral hip, subtrochanteric fracture, prophylactic pinning
Introduction
The management of the contralateral hip in unilateral slipped capital femoral epiphysis (SCFE) remains controversial.
Although relatively uncommon, subtrochanteric fractures, after in situ fixation of the unilateral SCFE, have been reported in the literature.
The first report of this complication was published in 1985 by Schmidt et al, following a call to collect cases of subtrochanteric fracture following multiple pin fixations at the 1983 annual meeting of the members of the Pennsylvanian Orthopedic Society, and subsequently by members of Pediatric Orthopedic Society of North America (POSNA). They collected and reported on ten cases following multiple pin fixations.1 Canale et al, in 1994 reported four subtrochanteric fractures through unused drill holes below screw fixation of the slipped hip.2 Ilchmann et al, in 2006 reported two adolescents who respectively sustained a subtrochanteric fracture 5 and 7 weeks after hardware removal.3 It is important to note that none of these cases occurred on the prophylactically pinned unaffected hip.
We describe two cases of subtrochanteric femoral fracture following prophylactic pinning.
Case report 1
A 13-year-old girl presented with a three-month history of a limp and painful left hip worsening ten days prior to presentation.
Clinical examination revealed an increased body mass index (26.23). There was a 2 cm shortening of the left leg above the knee. The left hip was fixed in 20° external rotation. Radiographs of the pelvis confirmed the SCFE on the left hip (Figure 1A). The SCFE was classified as acute-on-chronic, severe and unstable.

The patient underwent a single screw in situ pinning of the left hip as well as prophylactic pinning of the contralateral hip. During the operation more than one attempt was made when placing the single screw for the prophylactic pinning. Post-operative radiographs confirmed the screws to be appropriately positioned (Figure 1B). She was discharged three days later with protected weight bearing of the left leg using crutches.

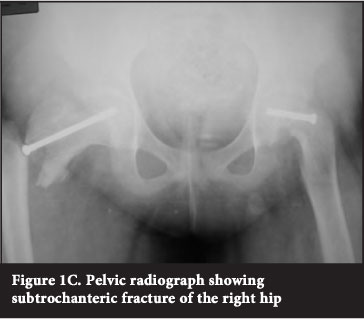
Three weeks later, she fell and returned with a painful right hip, and inability to weight bear. Radiographs revealed a subtrochanteric femoral fracture on the right (Figure 1C).
The patient underwent removal of screw and intramedullary fixation of the right proximal femur using a short intramedullary reconstruction nail (Figure 1D). She was subsequently discharged three days later on crutches.

At last follow-up, 22 months post-operatively, the patient reported occasional right groin pain. Clinical examination revealed normal right hip range of movements but the left hip showed sequellae of SCFE, with reduced internal rotation and increased external rotation. She was not tender on either hip. The radiographs taken at 22 months post-operatively confirmed that the right subtrochanteric fracture had healed and the left hip proximal physis had fused with no complications of chondrolysis or osteonecrosis (Figure 1E).

Case report 2
A 14-year-old boy presented with a three-week history of a limp and left knee pain, as well as inability to weight bear.
The left hip was in 25° of external rotation. Radiographs and CT scan of the pelvis confirmed the SCFE. The SCFE was classified as acute-on-chronic, severe and unstable. The patient stayed far from the hospital facility and it was doubted if the guardian understood the early signs of a slip.
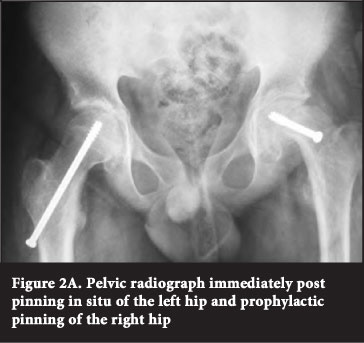
The patient underwent single screw in situ pinning of the left hip as well as prophylactic pinning of the contralateral hip (Figure 2A). He was discharged three days later on crutches and protected weight bearing of the left hip.
Five weeks later he returned following a fall, with a painful right hip and inability to weight bear. Radiographs revealed a subtrochanteric femoral fracture of the right hip.
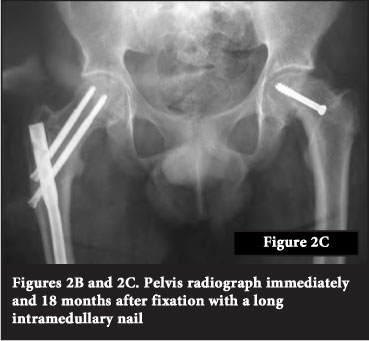
The following day, he underwent removal of the screw and intramedullary fixation of the proximal right femur using a long intramedullary reconstruction nail (Figures 2B and 2C). On day 3 post-op, he was discharged home on crutches.

At 18 months' follow-up, he was asymptomatic with a normal gait, negative Trendelenburg test and full range of movement on the previously fractured right femur. The slipped side was asymptomatic but had increased external rotation and no internal rotation.
Radiographs at 18 months' follow-up confirmed fracture union with no evidence of osteonecrosis or chondrolysis on the left hip (Figure 2D).
Discussion
Controversy still exists regarding prophylactic pinning versus observation.4-9 Schultz et al reported the risk of a contralateral slip developing in a patient with a unilateral SCFE to be 2.3 times higher than the risk of initial slip.10 Hágglund et al in their long-term follow-up, found that up to 65% of slips can be bilateral.11
Jerre et al, in their long-term follow-up reported that if all contralateral hips are pinned in unilateral SCFE about half of the operations will be unnecessary. They found no statistically significant evidence that the incidence of osteoarthritis in the contralateral hip was related to the occurrence of slipping or to management by pinning in situ.6
Vince et al agreed and reported in their long-term review of prophylactic pinning of the normal hip in SCFE that prophylactic pinning has the potential for complications, including post-op fracture, but none of their patients fractured before pin removal.12 However, these complications may not affect the future outcome, and should decrease with modern techniques of cannulated single screw insertion. Vince et al had a total of 75 patients who were pinned on the affected side. Six had pin complications that required further early surgery, and one had features suggestive of osteonecrosis that did not progress. There were 11 complications after pin removal, including one post-op fracture. There was no clear correlation between early complications and later arthrosis to justify prophylactic pinning.12
Schmidt et al reported that the majority of the subtrochanteric fractures in affected hips occurred at 35 ± 10 days after surgery for pinning in situ. All fractures healed without significant problems.1 In our study the two patients presented at three and five weeks post-operatively.
Loder et al reported on the risk of fracture on the affected unilateral SCFE, through an unused pinhole. This can be avoided with the use of fluoroscopy to position the guide pin correctly on the first attempt and by entering the guide wire proximal to the lesser trochanter.13 Loder and other authors also suggested avoiding additional screw holes as the best way to prevent this complication and advocated surgical treatment in the form of compression hip screw as a modality of choice.1,2,14-16
Loder et al advise using sound clinical judgment before recommending prophylactic pinning of the contralateral hip. Consideration must be given to the patient's age, sex, and endocrine status, as well as the preferences of the patient and family.13 Poor access to health facilities with long distances to travel and any suspicion of lack of compliance and poor understanding of early symptoms and signs to detect early slip would tend to favour doing prophylactic pinning, which was the case in our patient population.
Close analysis of initial post-op radiographs revealed evidence of multiple pinholes on the lateral cortex of the proximal femur resulting in a stress-riser effect and subsequent fracture. The entry point of both cannulated screws was just below the level of the lesser trochanter. These two risk factors have both been mentioned by Loder et al.13
Conclusion
While there are some reports on subtrochanteric fractures complicating the affected SCFE we did not find any reports on the prophylactic pinning side. Although extremely rare, it is essential, before recommending prophylactic pinning of the contralateral hip, to consider and counsel the parents and patients on possible complications, including subtrochanteric femur fracture. There is no substitute for accuracy of initial guide-wire placement, for the success of this operation.
No benefits of any form have been derived by the authors from any commercial party related directly or indirectly to the subject of this article.
References
1. Schmidt R, Gregg JR. Subtrochanteric fractures complicating pin fixation of slipped capital femoral epiphysis. Abstract. Pediatric Orthopedic Society of North America 1987:497. [ Links ]
2. Canale ST, Azar F, Young J, Beaty JH, Warner WC, Whitmer G. Subtrochanteric fracture after fixation of slipped capital femoral epiphysis: a complication of unused drill holes. J Pediatr Orthop 1994;14(5):623-26. [ Links ]
3. Ilchmann T, Parsch K. Complications at screw removal in slipped capital femoral epiphysis treated by cannulated titanium screws. Arch Orthop Trauma Surg 2006;126:359-36. [ Links ]
4. Maclean JGB, Reddy SK. The contralateral slip: An avoidable complication and indication for prophylactic pinning in SUFE. J Bone Joint Surg 2006;88B:1497-501. [ Links ]
5. Mininder S Kocher, Bishop JA. Prophylactic pinning of the contralateral hip after unilateral SCFE. J Bone Joint Surg 2004;86A:2658-65. [ Links ]
6. Jerre R, Billing JR, Hansson G, Wallin J. The contralateral hip in patients primarily treated for unilateral slipped upper femoral epiphysis. Long-term follow up of 61 hips. J Bone Joint Surg 1994;76B:563-67. [ Links ]
7. Larson AN, McIntosh AL, Trousdale RT, Lewallen DG. Avascular necrosis most common indication for hip arthroplasty in patients with slipped capital femoral epiphysis. J Pediatr Orthop 2010; 30(8):767-73. [ Links ]
8. Dickson KF, Bennett JT, Warren FH, Mast JW, Mayo KA, Darling J. Nonunion of femoral neck fracture and trochanteric osteotomy after a pinned, slipped capital femoral epiphysis: a case report. Am J Orthop (Belle Mead NJ) 2003;32(11):551-55. [ Links ]
9. Baynham GC, Lucie RS, Cummings RJ. Femoral neck fracture secondary to in situ pinning of slipped capital femoral epiphysis: a previously unreported complication. J Pediatr Orthop 1991;11(2):187-90. [ Links ]
10. Schultz WR, Weinstein JN, Weinstein SL. Prophylactic pinning of the contralateral SCFE: Evaluation of long-term outcome for the contralateral hip with use of decision analysis. J Bone Joint Surg Am 2002;84A:1305-14. [ Links ]
11. Hagglund G, Hansson LI, Ordeberg G, Sandström S. Bilaterality in slipped femoral epiphysis. J Bone Joint Surg 1988;70B:179-81. [ Links ]
12. Vince AS, Dunn TRC. Long-term review of prophylactic pinning of normal hip in SCFE. J Bone Joint Surg 1999;81B Suppl: 294. [ Links ]
13. Loder RT. Controversies in slipped capital femoral epiphysis. Orthop Clin North Am 2006;37(2):211-21. [ Links ]
14. Loder RT, Richards BS, Shapiro PS, Reznick LR, Aronson DD. Acute Slipped Capital Femoral Epiphysis: The importance of physeal stability. J Bone Joint Surg 1993;75A:1134-40. [ Links ]
15. Aronson DD, Loder RT. Slipped capital femoral epiphysis. Current concepts. J Am Acad Orth Surg 2006;14:666-79. [ Links ]
16. Canale ST, Casillas M, Banta JV. Displaced femoral neck fractures at the bone-screw interface after in situ fixation of slipped capital femoral epiphysis. J Pediatr Orthop 1997;17(2):212-15. [ Links ]
 Reprint requests:
Reprint requests:
Dr UNF Ukunda
Division of Orthopaedic Surgery
Wits Medical School
P O Box 1092 Benoni1500
Email: christ@netactive.co.za
Cell: 082 851 6864

