










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSA Orthopaedic Journal
versión On-line ISSN 2309-8309
versión impresa ISSN 1681-150X
SA orthop. j. vol.11 no.2 Centurion abr. 2012
CASE REPORT AND REVIEW OF THE LITERATURE
Neonatal compartment syndrome of the forearm
D ThompsonI; R SmitII; F GhimentonIII; O MahomvaIV; M AnnamalaiV
IFRCS, Department of Orthopaedics, Grey's Hospital, Pietermaritzburg, University of KwaZulu-Natal
IIFCS(Orth), Department of Orthopaedics, Grey's Hospital, Pietermaritzburg, University of KwaZulu-Natal
IIIFCS, Department of Paediatric Surgery, Grey's Hospital, Pietermaritzburg, University of KwaZulu-Natal
IVFCS (Plastic Surgery), Department of Plastic Surgery, Grey's Hospital, Pietermaritzburg, University of KwaZulu-Natal
VFCP (Paeds), Department of Paediatrics Grey's Hospital, Pietermaritzburg, University of KwaZulu-Natal
ABSTRACT
We present a clinical case of a neonate with a cellulitic appearance of the forearm. We discuss the differential diagnosis and the clinical features that led us to the diagnosis of forearm compartment syndrome. Early surgical decompression in this case resulted in a favourable outcome. To the best of our knowledge, this is the first case reported in the African literature.
Key words: Neonatal, forearm, compartment syndrome, decompression, cellulitis
Introduction
We report on a day-old neonate referred with forearm cellulitis (Figure 1).

Although cellulitis is not that unusual, the diagnosis of an acute neonatal forearm compartment syndrome is. Early recognition and surgical decompression in this case, resulted in an excellent outcome.
Compartment syndrome in the neonate presents differently to that in adults. Our review of the literature revealed that the diagnosis is most often made retrospectively when secondary complications have already occurred.
We discuss key diagnostic features that should aid in the early recognition of forearm compartment syndrome in a neonate presenting with a swollen erythematous limb.
Case report
A term male baby was referred to the Neonatal ICU at Grey's Hospital with possible cellulitis of the left arm.
This neonate (birth weight 2.5 kg) was born to a 23-year-old primigravida mother who delivered spontaneously and unattended in the passage of her local district hospital before help could arrive.
Maternal medical history was not significant. She tested negative for HIV and syphilis and no other cause for congenital infection was found.
Upon arrival at Grey's NICU, the patient was confirmed to be a normal looking infant, haemodynamically stable, not in respiratory distress and with no obvious systemic signs of infection. His left forearm was oedematous and erythematous with associated patchy areas of intense skin discolouration and blistering (Figures 2 and 3). In addition, the limb was warm and tender to touch. Active movement below the shoulder joint was absent. Passive movements of the limb and digits seemed neither to induce pain, nor to be limited. Capillary filling time of the fingers was adequate at less than one second. Pulses were of good volume and symmetrical in all the limbs. There was another erythematous lesion on the left side of the forehead. Caput moulding of the skull was present.


A peripheral venous line was established for intravenous fluid administration. Blood work up included a full blood count, C-reactive protein and blood cultures. The cutaneous blisters were aspirated and their content sent for microbiological tests and bacterial cultures. Broad-spectrum antibiotics were commenced while still awaiting bacterial culture results. All microbiological testing later yielded no organisms.
The infant underwent an urgent duplex-Doppler vascular assessment of the left upper limb. No abnormalities in either the arterial or the venous systems were demonstrated.
As the infant was stable and the affected limb was deemed viable, it was decided to keep the limb elevated and to reassess the infants condition and the status of the forearm the following morning. Overnight, the infant remained stable but the condition of the forearm did not improve.
A clinical diagnosis of a compartment syndrome of the forearm was made and consent was obtained for a surgical compartment release.
At surgery the blisters were aspirated and deroofed. A lazy S incision was made over the volar aspect of the forearm. There was significant subcutaneous oedema but the volar superficial compartment appeared normal with pink and reactive muscles. The deep compartment however was ischaemic, poorly reactive to electric stimulation and with associated spots of intramuscular haemorrhage (Figure 4).

The deep compartment including the carpal tunnel was completely released. The wound was not sutured and a protective moist dressing was applied.
In the days following the decompression the limb condition continued to improve, the oedema with the associated erythema subsided and the areas of patchy discoloured skin regained normal appearance.
The postoperative period was uneventful and split skin grafting of the cutaneous defect was performed on day 17 after admission. The duration of hospital stay was three weeks. The infant attended regular follow-up assessments and showed improvement in function at each visit. At three months, no clinical difference could be elicited in the function between his upper limbs.
Differential diagnosis
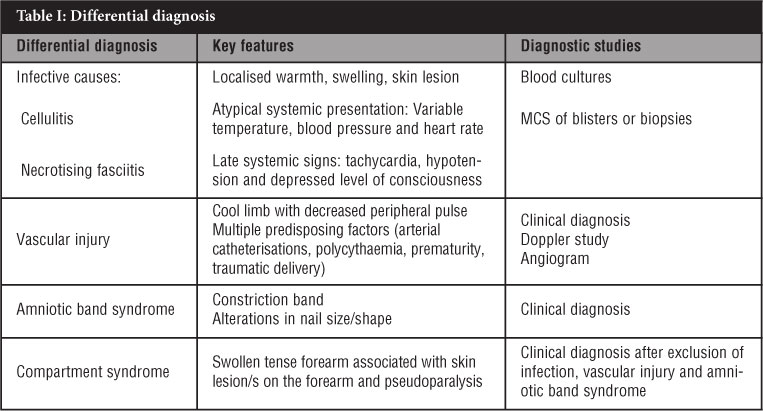
A neonate presenting with a cellulitic appearance of the forearm is not all that uncommon, and a wide differential diagnosis exists (Table I).
Infective causes can be excluded by examining the mother, by finding no general or local signs of infection and by finding negative cultures, growth and microscopy from the blisters or other tissue.
Necrotising fasciitis involves the superficial layers of skin and subcutaneous tissue, and can easily be mistaken for a compartment syndrome. It is confirmed at operation and treated by excision, not fasciotomy.
Cham et al1 also includes congenital varicella (dermatomal cicatricial lesions), epidermolysis bullosa (skin fragility and bullae) as well as aplasia cutis congenital (ulcerated lesions mostly on the scalp and other areas) in the differential diagnosis.
Vascular injuries are often associated with brachial plexus lesions, and although they present with forearm cellulitis, the absence of pulses clinically and on Doppler studies, confirms this diagnosis.
An amniotic band syndrome is easily seen clinically, but can cause necrosis and a cellulitic area.
It has also been noted by Kline and Moore2 that compartment syndrome may be initiated before delivery, but in our case there were no predisposing conditions such as prematurity, oligohydramnios, polycythaemia or maternal diabetes.
We feel that the compartment syndrome in our neonate was caused by a compound presentation where the left forearm had been caught between the rim of the mothers pelvis and the skull. A CT of the brain and skull showed a left parietal bone fracture and the associated skin lesion over this site supported this conclusion (Figure 5).

Discussion
The diagnosis of compartment syndrome of the forearm was made after excluding other causes of a cellulitic looking limb. An excellent outcome was achieved as a result of recognition and early surgical decompression.
Ragland et al3 reporting retrospectively on 24 cases over a 20-year period, found that only one case had a favourable outcome, and that was the only case of this group where a decompression had been performed. They also noted that a cellulitic or necrotic skin lesion was the common, salient feature in all cases. We would concur.
Kline and Moore2 discuss two cases treated early with good clinical outcomes and suggest that compartment syndrome should be considered in any neonate presenting with a motionless limb. This was not the reason for referral in our case.
The findings of forearm erythema, skin bullae and necrosis were also noted by Aydin et al4 to be the predominant feature in their study.
Ischaemic contracture is a late manifestation of an untreated or incompletely treated forearm compartment syndrome as discussed in most of the articles reviewed.1,5,6-8
This did not occur in our case. A long-term sequela of epi-physeal damage with bone shortening was also reported in these late cases, and it remains to be seen if we have avoided this complication.
Some of the classical symptoms of compartment syndrome such as pain at rest, pain on passive stretch and sensory abnormalities are not useful in the new-born and other signs need to be considered.
Conclusion
We present a case of neonatal forearm compartment syndrome as a result of birth trauma during an unassisted vaginal delivery. We believe a swollen, tense forearm associated with a skin lesion and pseudoparalysis in the absence of infection, arterial injury or amniotic band syndrome is the most likely presentation of compartment syndrome in the new-born. We further believe that, as with adult compartment syndrome, early surgical decompression is the preferred treatment and most likely to result in a good outcome.
The content of this article is the sole work of the authors. No benefits in any form have been or are to be received from a commercial party related directly or indirectly to the subject of this article. Informed consent was received from the affected family. An ethical committee has approved this article.
References
1. Cham PMH, Drolet BA, Segura AD, Esterly NB. Congenital Volkmann ischaemic contracture; a case report and review. Br J Dermatology 2004; 150(2):357-63. [ Links ]
2. Kline SC, Moore JR. Neonatal compartment syndrome. J Hand Surg Am 1992;17(2):256-59. [ Links ]
3. Ragland R, Moukoko D, Ezaki M , Carter PR, Mills J. Forearm compartment syndrome in the newborn: report of 24 cases. J Hand Surg Am 2005;30(5):997-1003. [ Links ]
4. Aydin A, Bicer A, Basaran K, Keklik B. Neonatal forearm compartment syndrome: case report. Balkan Medical Journal 2010; 27(2):192-94. [ Links ]
5. Cauette-Laberge L, Bortoluzzi P, Egerszegi EP, Marton D. Neonatal Volkmann's ischemic contracture of the forearm: a report of five cases. Plast Reconstr Surg 1992;90(4):621-28. [ Links ]
6. Leaute-Labreze C, Depaire-Duclos F, Sarlangue J, Fontan D, Sandler B,Maleville J, Taieb A. Congenital cutaneous defects as complications in surviving co-twins. Aplasia cutis congenital and neonatal Volkmann ischaemic contracture of the forearm. Arch Dermatol 1998;134:1121-24. [ Links ]
7. Tsujino A, Hooper G. Neonatal compression ischaemia of the forearm. J Hand Surg Br 1997;22(5):612-14 [ Links ]
8. Silfen R, Amir A, Sirota L, Hauben DJ. Congenital Volkmann-Lesser ischaemic contracture of the upper limb. Ann Plast Sur 2000;45(3):313-17. [ Links ]
 Reprint requests:
Reprint requests:
Dr D Thompson
Department of Orthopaedics
Grey's Hospital Pietermaritzburg
Private Bag 9001
Tel: (033) 897-3299
Fax: 086 5784 1 00
Email: david.thompson@kznhealth.gov.za


{kind=link}