










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSA Orthopaedic Journal
On-line version ISSN 2309-8309
Print version ISSN 1681-150X
SA orthop. j. vol.10 n.4 Centurion Jan. 2011
LETTERS TO THE EDITOR
Dupuytren's contracture
Dr JP Driver-JowittI; S OlmesdahlII
IFRCS (orthopaedic surgeon)
IIBSc Med (student)
We support the concept of avoiding straight incisions, and particularly straight axial incisions, in the management of Dupuytren's contracture.1
Likewise we applaud using skin hooks instead of toothed forceps, which practice we have found reduces pain, scarring and postoperative infection significantly.
However the multiple Zplasties suggested by Mennen produces a problem in that there is shortening of the transverse axis of the palm. At times this results in difficulty flattening the palm.
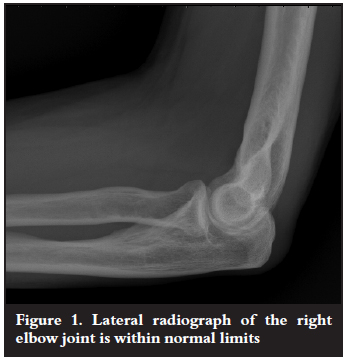
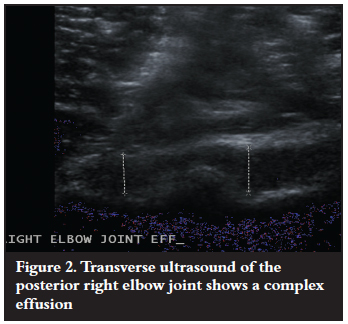
Therefore, over the last 40 years the technique of 'detour incisions' has been used, whereby the incisions follow only the skin creases in the hand. The incidence of recurrence has been comparable to that reported by Mennen. Further, it has not been our practice for some years to splint the hand post-operatively (Figures 1 and 2).
It is also our policy to restrict diathermy2 to the minimum and then to use not more than 8 watts power.
We have found that copious washing of the wounds throughout the procedure reduces both infection3 and (inflammatory) pain.
References
Mennen U. Dupuytren's contracture: the zfactor, South African Orthopaedic Journal, 2010;8(3):7982. [ Links ]
Lowe D, . doi: 10.1016/j.otohns.2008.08.025 Otolaryngol Head Neck Surg January 2009;140(1):23-28. [ Links ]
Gustilo RB, Anderson JT. Prevention of infection in the treatment of one thousand and twentyfive open fractures of long bones. Journal of Bone and Joint Surgery (Am) 1976;58(4):453-58. [ Links ]
16 August 2011
(This letter was written in response to Mennen, U. 2010. Dupuytren's contracture: the z-factor, South African Orthopaedics Journal, vol 8 (3) p 79-82.)
Dear Editorial Board of the SA Orthopaedic Journal
Please find enclosed the manuscript 'Letter to editor: Evaluation of periarticular aggressive benign bone tumours treated with cementation and a locked plate' by Sanjay Meena to be submitted as a letter to editor in the SA Orthopaedic Journal.
I believe that our observation could be of interest to readers of this journal.
Sincerely yours,
Sanjay Meena
23 September 2011, New Delhi
Corresponding author: Sanjay Meena, MBBS, MS, Registrar, All India Institute of Medical Sciences (AIIMS), New Delhi 110029, India
Sir,
I read with interest the article 'Evaluation of periarticular aggressive benign bone tumours treated with cementation and a locked plate'.1 I must congratulate the authors for the research which is highly relevant in developing country like ours. The availability of indigenous affordable prosthesis may enthuse many a young surgeon to advocate excision and replacement in large or recurrent GCTs. A megaprosthesis is an excellent option in well-selected cases but this enthusiasm must be tempered by the fact that, because GCT is a benign lesion, the patient is likely to have a normal lifespan and a biological reconstruction may in the long term prove to be a more durable option, especially keeping in mind the socio-economic strata to which most of our patients belong. The authors may have used the sandwich technique in their patients to maintain the smoothness of articular cartilage and prevent early osteoarthritis. In this technique, allograft/autograft is packed adjacent to the subarticular surface. A layer of gelfoam is layered over this and the remaining cavity is packed with cement.2 This helps reduce heat damage from the curing cement, and the subarticular bone graft after consolidation should theoretically prevent articular degeneration.3 Another perceived advantage is that, should recurrence occur, the danger of damage to articular cartilage during removal of cement is reduced.
Liquid nitrogen was used as a further adjunct whenever feasible in this study. Cryosurgery using liquid nitrogen first propagated by Marcove, is associated with a high incidence of local wound and bone complications.4 I once again congratulate the author for this excellent study.
References
Pikor TD, Kyte, RD. Evaluation of peri-articular aggressive benign bone tumours treated with cementation and a locked plate. SA Orthop Journal. 2011;10(2):48-55. [ Links ]
Salgia A, Biswas SK, Agrawal R, Goyal V. Multicentric giant cell tumour around the knee. Indian J Orthop 2007;41:151-53. [ Links ]
Chen TH, Su YP, Chen WM. Giant cell tumours of the knee: Subchondral bone integrity affects the outcome. Int Orthop 2005;29:30-34. [Pubmed] [Full text] [ Links ].
Malawer MM, Bickels J, Meller I, Buch RG, Henshaw RM, Kollender Y. Cryosurgery in the treatment of giant cell tumor. A long-term follow up study. Clin Orthop Relat Res 1999;359:176-88. [ Links ]

