










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSA Orthopaedic Journal
versión On-line ISSN 2309-8309
versión impresa ISSN 1681-150X
SA orthop. j. vol.10 no.3 Centurion ene. 2011
CLINICAL ARTICLE
Functional outcome of bicondylar tibial plateau fractures treated with the Ilizarov circular external fixator
N FerreiraI; ME SenogeII
IBSc, MBChB(Stell), HDip Orth(SA), FCOrth(SA). MMed Student, UKZN
IIMBChB, FCS Orth(SA). Head of Department. Tumour, Sepsis and Reconstruction Unit, Department of Orthopaedic Surgery, Grey's Hospital, University of KwaZulu-Natal, Pietermaritzburg, South Africa
ABSTRACT
BACKGROUND: Bicondylar tibial plateau fractures are often associated with severe soft tissue injuries that can frequently result in compartment syndrome and are frequently open fractures. Operative management of these injuries is invariably complicated by the condition of the soft tissue envelope of the proximal tibia.
METHODS: Between July 2008 and March 2009, 13 consecutive patients who sustained bicondylar tibial plateau fractures were treated with Ilizarov fine wire circular external fixators. These 13 patients were reviewed with regard to their functional outcome and any complications incurred during the management period.
RESULTS: Eleven patients met the inclusion and exclusion criteria. All patients achieved bony union and had good functional results without serious complications. No osteomyelitis, septic arthritis, loss of reduction or wound dehiscence occurred. Superficial pin tract infection was the most common complication encountered, but in all cases pin site care and oral antibiotics were sufficient to eradicate the problem and no pins or wires needed to be removed or resited.
CONCLUSION: The treatment of bicondylar tibial plateau fractures with the Ilizarov circular external fixator is safe and effective, and produces good functional results without serious complications.
Key words: Tibial plateau fracture, external fixator, functional outcome
Introduction
Tibial plateau fractures comprise a diverse group of injuries to a major weight-bearing joint, and are frequently associated with functional impairment.1 The most widely used classification system for these fractures was proposed by Schatzker,2 and divides these fractures into two groups, namely lowenergy and high-energy fracture patterns.
High-energy fractures pose a significant challenge to the orthopaedic surgeon tasked with their reconstruction. Schatzker type-V and VI injuries involve both the medial and lateral tibial condyles, with varying amounts of articular surface comminution. The soft tissue typically reflects the underlying bony damage, and can often present as open fractures. Reported incidences of open fractures range from 25% to 37%, with a high percentage of the remaining fractures associated with significant closed soft tissue injuries.3-11
Although the ideal method of fixation of these fractures remains controversial, a biological approach to the soft tissue envelope of the proximal tibia can help minimise some of the complications that often follow surgical intervention.
The purpose of this study is to evaluate the management of these complex injuries with the Ilizarov tensioned fine wire circular external fixator. Particular attention is paid to the functional outcome of, and complications associated with, this treatment method.
Materials and methods
Between July 2008 and March 2009, 13 consecutive patients with high-energy bicondylar tibial plateau fractures were managed with the use of the Ilizarov circular external fixator. These 13 patient records were reviewed. Inclusion criteria were patients of skeletal maturity with bicondylar tibial plateau fractures that were treated with the Ilizarov circular external fixator. Patients were excluded if they had any of the following: (1) a condition that would impede the rehabilitation process of the patient - for example, acetabular fractures that would require prolonged immobilisation; (2) concomitant injuries that could alter the functional outcome of the patient - for example, ipsilateral femoral shaft fractures; (3) previous major trauma, surgery or deformity of the affected knee. Eleven patients met these criteria (Table I). One patient was excluded due to severe concomitant injuries, including head injury, blunt abdominal trauma, and a contralateral Gustilo-Anderson IIIB compound tibia fracture with 4 cm bone loss that also required an Ilizarov circular external fixator. The second patient was excluded because of a concomitant ipsilateral acetabulum fracture that required open reduction and internal fixation.
The records of these patients were reviewed, and information was extracted regarding patient demographics, mechanism of injury, injury classification (bony and soft tissue), operative procedures, complications and follow-up Knee Society Clinical Rating Scale scores.12
All radiographs were reviewed. The fractures were classified using the Schatzker classification on the preoperative radiographs. Postoperative films were assessed for method and adequacy of reduction. The maintenance of reduction and union was evaluated on later follow-up radiographs.
Of the 11 patients, eight were male and three female. The median age was 40 years, ranging from 19 to 59 years. Mechanism of injury included pedestrian vehicle accidents (n = 4), occupants in motor vehicle accidents (n = 3), fall from height (n = 3) and assault (n = 1). Ten patients had Schatzker VI fractures and one patient had a Schatzker V fracture.
Open fractures were found in three cases and classified according to the Gustilo and Anderson classification as grade IIIA in one case, and IIIB in two cases (Figure 1 and 2).13 The remaining eight cases were all associated with extensive closed soft tissue injuries and were graded according the classification proposed by Tscherne and Gotzen.14 All open fractures were initially treated with debridement, irrigation and antibiotics. One of these patients was also found to have compartment syndrome and underwent emergent fasciotomy at the time of initial debridement. One patient with an open fracture had an initial joint spanning monolateral external fixator applied after debridement. All three patients with open fractures required an additional soft tissue procedure: split skin graft, fasciocutaneous flap, and a myocutaneous flap respectively (Table II).


Three patients had associated musculoskeletal injuries. Contralateral femoral shaft fractures (n = 2) were treated with antegrade femoral nailing. One patient had bilateral tibial plateau fractures. His contralateral plateau fracture (Schatzker IV) was treated with a lateral locking plate at the time of Ilizarov application.
The average time to surgery was 10.1 days, ranging from 2 to 22 days. The delay in definitive management was as a result of a combination of factors including: delay in referral from peripheral centres, delays in acquiring CT scans, and lack of theatre time availability.
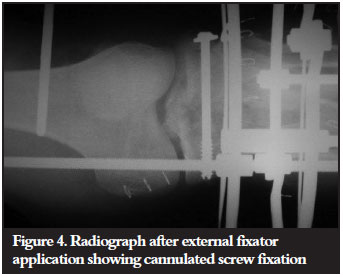
All the definitive surgeries were performed by the primary author, and the Ilizarov system (Smith & Nephew) was used in all cases. A four-ring construct was employed, with a 5/8 ring proximally to allow greater knee flexion. For proximal ring block fixation, 1.8 mm tensioned wires were used and a combination of 1.8 mm tensioned wires and hydroxyapatite half pins were used in the distal ring block. One case required an initial aboveknee Ilizarov extension for 6 weeks, in order to allow a soft tissue flap anterior to the knee to heal, prior to allowing knee mobilisation (Figure 3). All 11 patients had limited open reduction and eight patients had additional percutaneous cannulated screw fixation (Figure 4). One patient had iliac crest bone graft at the time of frame application, and another required iliac crest bone graft for a metaphyseo-diaphyseal non-union.

Pin site care comprised initial absorbent dressings for five days post surgery, followed by twice-daily cleaning with saline or soapy water until the skinpin interface had healed. If pin site infection occurred, the patient was instructed to recommence the pin site cleaning and a course of oral antibiotics was prescribed.
Particular attention was paid to anatomical safe zones with wire placement, and no intra-operative iatrogenic nerve or vascular injury occurred. Ankle equinus deformity was prevented by meticulous wire placement technique, active joint mobilisation post-operatively and splinting of the foot in a neutral position.
Early range of movement exercises for the knee and mobilisation with crutches was encouraged in all cases. Weight bearing was delayed for approximately six weeks after which proprioceptive retraining was commenced and progressive weight bearing encouraged until full weight bearing with or without walking aids was achieved.
After discharge, patients attended the orthopaedic outpatient clinic. On these follow-up visits patients were assessed for any complications, including soft tissue complications, infection or loss of reduction. Functional outcome was also determined using the Knee Society Clinical Rating Score. The external fixator was removed once radiographic evidence of union was established.
Results
All fractures united at a median of 22 weeks, ranging from 17 to 39 weeks. One patient required additional iliac crest autologous bone graft for a metaphyseo-diaphyseal non-union at 24 weeks. The bone grafting was performed without adjustment of the external fixator and union was achieved 15 weeks later after which the external fixator was removed.
During visits to the orthopaedic outpatient department, follow-up radiographs were taken. No loss of reduction occurred after frame application.
Knee Society Clinical Rating scores ranged from 62.5 to 97, translating into a good result on average (Table III). Based on the scores, six outcomes were excellent, two good and three fair (Figure 5 and 6). Average range of motion of the knee was 109º (range 90º to 125º). Seven of the patients ambulated without support while four required a cane to aid mobilisation.


Pin site infection was a common complication, diagnosed in six of the eleven patients (66%). However, all these cases responded to pin site care and oral antibiotics, and none of the pins or wires needed to be removed or resited. No cases of wound dehiscence, infection, osteomyelitis or septic arthritis were encountered, and no patient required removal of the external fixator prior to fracture union.
Discussion
The treatment goal for bicondylar tibial plateau fractures is to obtain a stable, aligned, painless and mobile knee and to minimise the risk of post-traumatic osteoarthritis. In order to achieve this outcome the value of early joint mobilisation has been well established by the work of Apley.15,16 Fracture reduction and stable fixation is required to allow early joint motion.
Traditionally dual plating was considered to be the best mechanical method of stabilisation for these fractures, as it addresses both the medial and lateral columns to achieve reduction and stability.2 However, this is fraught with complications as it requires extensive soft tissue dissection in order to place these plates, and this in an environment that is already compromised due to the high-energy trauma sustained. Consequently, a high rate of complication remains associated with this open technique.10,11,17,18 Jiang et al. reported a deep infection rate of 4.7% with dual plating and 7.3% if a less invasive stabilisation system (LISS) was used.19
In order to overcome this complication, less invasive techniques with external fixators were introduced as a strategy to minimise the iatrogenic soft tissue injury. Monolateral fixators have been used in this regard and, although they have been successful in reducing the rate of the soft tissue complications,20,21 the mechanical stability of this technique is not adequate, and loss of reduction has been reported.21
The inherent mechanical disadvantage of a monolateral fixator arises from the cantilever loading forces which they are subjected to, producing increasingly less stable fixation further away from the fixator. Ring fixators, like the Ilizarov system, with tensioned fine wires, utilise beam loading to create uniform support for the joint and stable fracture immobilisation to achieve fracture union.
Recent biomechanical studies proved that fine-wire fixators provide adequate mechanical stability for the fixation of bicondylar tibial plateau fractures.22,23 Watson et al. demonstrated that four olive wires combined with a lag screw provided the most stability, even when compared to dual plating.23 This allows for early joint mobilisation without risking loss of reduction.
Several published studies have shown decreased complications when treating bicondylar tibial plateau fractures with fine-wire external fixators. Kataria et al. reported on a series of 38 patients treated with small-wire external fixators and had no incidences of non-union or septic arthritis.24 Ali et al. reported on 20 patients treated with a hybrid external fixator, in which all patients achieved bony union and no patients developed osteomyelitis or septic arthritis.3 In a series by Dendrinos, 24 patients were treated with the Ilizarov circular fixator, and there was no incidence of osteomyelitis or septic arthritis.25 Chin et al. reported similar results of 18 patients, none of whom developed wound dehiscence, infection, osteomyelitis or septic arthritis.26 The current series is comparable to these studies in that no cases of wound dehiscence, infection, osteomyelitis or septic arthritis were encountered.
The functional outcome of this series compares favourably to other published studies, achieving an average Knee Society Clinical Rating Score of 84.2. Several published papers have confirmed these good functional results, with average Knee Rating scores raging from 65.9 to 80.2.9,26-29 Many of these studies included polytrauma patients that resulted in lower average scores. In a recent study, Katsenis showed satisfactory functional results at a minimum fiveyear follow-up, confirming that these good early results can be maintained over the mediumtolong term.8
From these results it appears that a fine-wire external fixator with or without limited open reduction, succeeds in providing stable fixation for these complex injuries without imparting added trauma to an already compromised soft tissue envelope.
Limitations of this paper include the small number of cases and the retrospective nature of the review. Also, the exclusion of patients with certain concomitant injuries could lead to a selection bias, possibly omitting patients with more severe injuries.
Conclusion
Ilizarov circular external fixation is a safe, effective treatment option for bicondylar tibial plateau fractures, with good functional results. This technique is very attractive in patients with severe damage to the soft tissue envelope of the proximal tibia which would make open reduction with extensive surgical dissection less desirable.
Seeing as these patients often suffer articular surface damage at the time of injury, it might be reasonable to expect that a large proportion might require knee arthroplasty at a later stage. A possible further advantage of this treatment modality is the fact that minimal dissection is performed, and minimal metal ware is left in situ. This might prove advantageous at the time of arthroplasty surgery.
Further research in this regard is necessary.
References
1. Gaston P, Will EM, Keating JF. Recovery of knee function following fracture of the tibial plateau. J Bone Joint Surg [Br] 2005;87-B:1233-36. [ Links ]
2. Schatzker J, McBroom R, Bruce D. The tibial plateau fracture. The Toronto experience 1968-1975. Clin Orthop Relat Res 1979;138:94-104. [ Links ]
3. Ali AM, Burton M, Hashmi M, Saleh M. Outcome of complex fractures of the tibial plateau treated with beam-loading ring fixation system. J Bone Joint Surg [Br] 2003;85-B:691-99. [ Links ]
4. Benirschke SK, Agnew SG, Mayo KA, Santoro VM, Henley MB. Immediate internal fixation of open complex tibial plateau fractures: treatment by a standard protocol. J Orthop Trauma 1992;6:78-86. [ Links ]
5. El Barbary H, Abdel Gani H, Misbah H, Salem K. Complex tibial plateau fractures treated with Ilizarov external fixator with or without minimal internal fixation. International Orthopaedics (SICOT) 2005;29:182-85. [ Links ]
6. ElWahab MA. Treatment of tibial plateau fractures by Ilizarov external fixator. Benha M J 2009;26:233-45. [ Links ]
7. Faldini C, Manca M, Pagkrati S, Leonetti D, Nanni M, Grandi G. Romagnoli M, Himmelmann M. Surgical treatment of complex tibial plateau fractures by closed reduction and external fixation. A review of 32 consecutive cases operated. J Orthopaed Traumatol 2005;6:188-93. [ Links ]
8. Katsenis D, Dendrinos G, Kouris A, Savas N, Schoinochoritis N, Pogiatzis K. Combination of fine wire fixation and limited internal fixation for high-energy tibial plateau fractures: functional results at minimum 5-year follow-up. J Orthop Trauma 2009;23:493-501. [ Links ]
9. Katsenis D, Vasilis A, Panayiotis M, Minos T, Lambiris E. Minimal internal fixation augmented by small wire transfixion frames for high-energy tibial plateau fractures. J Orthop Trauma 2005;19:241-48. [ Links ]
10. Young MJ, Barrack RL. Complications of internal fixation of tibial plateau fractures. Orthop Rev 1994;23:149-54. [ Links ]
11. Barei DP, Nork SE, Mills WJ, Bradford Henley M, Benirschke SK. Complications associated with internal fixation of high-energy bicondylar tibial plateau fractures utilizing a two-incision technique. J Orthop Trauma. 2004;18:649-657. [ Links ]
12. Rationale of The Knee Society Clinical Rating System. Clin Orthop. 1989;248:13-14. [ Links ]
13. Gustilo R, Mendoza R, Williams D. Problems in the management of type III (severe) open fractures: a new classification of type III open fractures. J Trauma 1984;24:742-46. [ Links ]
14. Tscherne H, Gotzen L. Fractures with soft tissue injuries. Berlin: Springer;1984. [ Links ]
15. Apley AG. Fractures of the lateral tibial condyle treated by skeletal traction and early mobilization: a review of sixty cases with special reference to the long-term results. J Bone Joint Surg [Br] 1956;38-B:699-708. [ Links ]
16. Apley AG. Fractures of the tibial plateau. Orthop Clin North Am. 1979;10:61-74. [ Links ]
17. The Canadian Orthopaedic Trauma Society. Open reduction and internal fixation compared with circular fixator application for bicondylar tibial plateau fractures. Results of a multicenter, prospective, randomized clinical trial. J Bone Joint Surg 2006;88:2613-23. [ Links ]
18. Lee JA, Papadakis SA, Moon C, Zalavras CG. Tibial plateau fractures treated with the less invasive stabilisation system. International Orthopaedics (SICOT) 2007;31:415-18. [ Links ]
19. Jiang R, Luo C, Wang M, Yang T, Zeng B. A comparative study of Less Invasive Stabilization System (LISS) fixation and two-incision double plating for the treatment of bicondylar tibial plateau fractures. Knee 2008;8:139-43. [ Links ]
20. Ries MD, Meinhard BP. Medial external fixation with lateral plate internal fixation in metaphyseal tibia fractures. A report of eight cases associated with severe soft tissue injury. Clin Orthop 1990;215-23. [ Links ]
21. Marsh JL, Smith ST, Do TT. External fixation and limited internal fixation for complex fractures of the tibial plateau. J Bone Joint Surg Am 1995;77:661-73. [ Links ]
22. Ali AM, Yang L, Hashmi M, Saleh M. Bicondylar tibial plateau fractures managed with the Sheffield hybrid fixator. Biomechanical study and operative technique. Injury, Int J Care Injured 2001;32:S-D-86-S-D-91. [ Links ]
23. Watson JT, Ripple S, Hoshaw SJ, Fyhrie D. Hybrid external fixation for tibial plateau fractures: Clinical and biomechanical correlation. OrthopClin North Am 2002;33. [ Links ]
24. Kataria H, Sharma N, Kanojia RK. Small wire external fixation for high-energy tibial plateau fractures. J Orthop Surg 2007;15(2):137-43. [ Links ]
25. Dendrinos GK, Kontos S, Katsenis D, Dalas A. Treatment of high-energy tibial plateau fractures by the Ilizarov circular fixator. J Bone Joint Surg [Br] 1996;78-B:710-17. [ Links ]
26. Chin TYP, Bardana D, Bailey M, Williamson OD, Miller R, Edwards ER, Esser MP. Functional outcome of tibial plateau fractures treated with the fine-wire fixator. Injury, Int. J. Care Injured 2005;36:1467-75. [ Links ]
27. Mikulak SA, Gold SM, Zinar DM. Small wire external fixation of high-energy tibial plateau fractures. Clin Orthop Relat Res 1998;365:230-38. [ Links ]
28. Kumar A, Whittle AP. Treatment of complex (Schatzker type VI) fractures of the tibial plateau with circular wire external fixation: retrospective case review. J Orthop Trauma 2000;14(5):339-44. [ Links ]
29. Subasi M, Kapukaya A, Arslan Huseyin, Ozkul E, Cebesoy O. Outcome of open comminuted tibial plateau fractures treated using an external fixator. J Orthop Sci 2007;12:347-53. [ Links ]
 Reprint requests:
Reprint requests:
Dr N Ferreira
Department of Orthopaedic Surgery Grey's Hospital Private bag X9001
Pietermaritzburg 3201
Tel: +27 033 897 3299 Fax: +27 33 897 3409
Email: drnferreira@telkomsa.net
The content of this article is the sole work of the authors. No benefits of any form have been received or will be received from a commercial party related directly or indi rectly to the subject of this article. The research has been approved by an ethical committee.

