










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSA Orthopaedic Journal
versión On-line ISSN 2309-8309
versión impresa ISSN 1681-150X
SA orthop. j. vol.10 no.2 Centurion ene. 2011
BASIC MEDICAL SCIENCE ARTICLE
Vitamin D and health - a historical overview
EJ RaubenheimerI; CEE NoffkeII
IMChD, PhD, DSc. Professor
IIMSc(Odont). Associate Professor. Faculty of Health Sciences, Medunsa Campus, University of Limpopo, South Africa
ABSTRACT
Awareness of the importance of skin exposure to UV rays for normal bone growth and systemic health increased with landmark scientific discoveries over the past century. Several Nobel-prize laureates unravelled the steps involved in the activation of 7-dehydrocholesterol to 1,25 (OH)2 vitamin D (or vit D3) which is rapidly becoming the most important medical discovery in the past decade. Recent developments in our understanding of the impact of vit D on the immune system, carbohydrate metabolism, and cardiovascular and neoplastic diseases are briefly highlighted.
Key words: vitamin D, cholecalciferol, ergocalciferol, phototherapy, UV light
Historical perspective
Before 1890 it was noticed that children who grew up along the coast in Europe (where sunshine and fresh air are more prevalent) manifested with less stunted skeletal growth and bowing of weight-bearing bones than those dwelling in cities. Niels Ryberg Finsen, a native of the Faroe Islands (south of Iceland) and a medical graduate of the University of Copenhagen in 1890, suffered from Pick's disease which is characterised by progressive thickening of the membranes of the heart, spleen and liver. He lived in a house facing north and believed that his progressive tiredness and ascites were the result of a lack of sunlight. From his early appointment as a tutor in anatomy he collected data on animals seeking sunlight, with a firm conviction of the as yet undiscovered benefits thereof. In simple experiments Finsen demonstrated that rays from the sun and an electrical arc may have strong antimicrobial effects and stimulate tissue health. He proved convincingly the benefit thereof for patients suffering lupus vulgaris (skin tuberculosis) and smallpox (which spread in epidemic proportions through Europe at the time). Finsen soon became known as the father of phototherapy for which he received the Nobel Prize in 1903.1 His name was immortalised with other Nobel Prize laureates like Emil von Behring 1901 (serum therapy), Ronald Ross 1902 (malaria infection), Ivan Pavlov 1904 (physiology of digestion) and Robert Koch 1905 (tuberculosis research) who laid significant foundations for modern medicine during the first decade of the twentieth century. Phototherapy clinics where chronic infectious diseases (mainly tuberculosis) and rickets were treated arose in sunny locations such as high in the Alps and high altitude states like Michigan. One such example is the Battle Creek Sanatorium, a health resort for permanently disabled soldiers of the American wars, which was rebuilt by John Harvey Kellog in 1902 after a devastating fire.
A change of two letters transformed 'sanatorium' to 'sanitarium' and a new word emphasising wellness was added to the English language. The phototherapy and thermotherapy department, accommodating the first electric light bath, treated notable patients like CW Post (founder of Post Cereals), Amelia Earhart (first female aviator across the Atlantic ocean), Johnny Weissmuller (famous for acting Tarzan), Henry Ford and Mary Lincoln, wife of President Lincoln.2 It was soon discovered that sun exposure was as effective as cod liver oil in the treatment of rickets and that glass filtered out the 'health' benefits thereof. (Today we know that glass neutralises the β-fraction of ultraviolet (UV) light required for activation of the precursors of vitamin D.)
The build-up to the discovery of vitamin D (vit D) had a long history and involved many research teams, all of which cannot be acknowledged due to a lack of space. A key experiment was performed in 1922 by McCullum et al3 who showed that heated cod liver oil lost its antixerophthalmic effect which was known to be the result of a factor A (later named vitamin A) but retained its capacity to cure rickets in rats. Because the water soluble factors discovered at the time were termed vitamin B and the anti-scurvy factor vitamin C, they named the newly discovered factor vit D. A Nobel Prize laureate in 1928 and physician trained in Berlin, Adolf Windaus, who dedicated his scientific career to sterol biochemistry, discovered a plant steroid from ergot (mushrooms) which, when irradiated, cured rickets in rats.4
The irradiated product of ergosterol was purified by Windaus and other research teams5 and was named vitamin D2 which in sub-microgram concentrations demonstrated potent anti-rachitic properties. One question however remained. Ergosterol does not occur in humans. How do humans obtain the active form of vit D through exposure to sunlight? In 1937 after exhaustive work and long after his Nobel award, Windaus and Bock6 identified 7-dehydrocholesterol in skin of several species. This substance, which was also present in whole milk and liver, was converted to an anti-rachitic agent through irradiation. The irradiated product was named vit D3 or cholecalciferol. The complete photochemical reaction of ergosterol and cholecalciferol was deciphered in 1955 by Vellus et al.
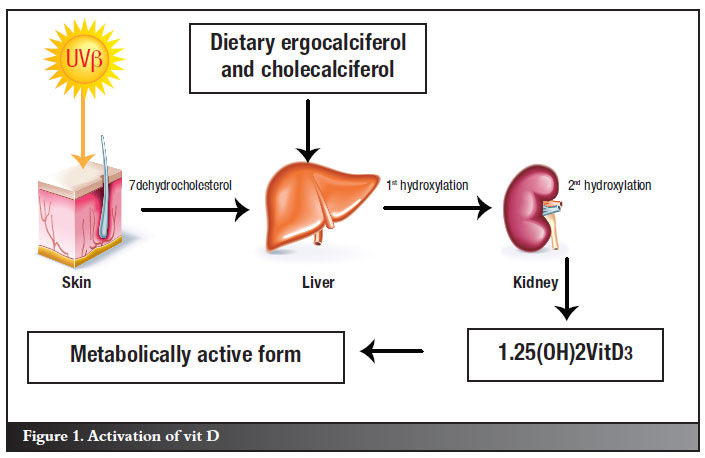
Metabolic activation
A detailed account of the biochemical processes involved in the activation of vit D does not fall within the scope of this article. It is however clear from the diagram presented in Figure 1 that the activation follows a multi-step pathway involving UV irradiation of the skin and two phases of hydroxylation to 25(OH) vit D (vit D2) and 1,25(OH)2 vit D (vit D3) in the liver and kidney respectively. The metabolically active form is vit D3. Vit D is a fat-soluble substance with a half-life of approximately three weeks in the 25(OH) vit D stage and only several hours as 1,25(OH)2 vit D. Its fat solubility results in higher dosages required to achieve normal blood levels in obese persons compared to those with a normal body fat composition.
The melanin content of the skin is another determinant of the efficiency of the first step in the activation of the biochemical cascade. It has been demonstrated that 18 millijoule UV per cm2 lightly pigmented irradiated skin produces the same concentration vit D3 as 5-10 times more irradiation of a heavily pigmented skin.8,9 Melanin pigment is one of the important regulators of vit D activation. This may serve as an explanation for the different susceptibilities for diseases between races as well as the geographic distribution of races, where most of the lighter pigmented races populate the northern hemisphere (UV deficient) and the darker races the tropics where sun exposure is significantly more intense and protection is required in order to prevent over-activation of vit D.
A question arises on whether vit D is indeed classifiable as a vitamin. The generally accepted definition of a vitamin is that it is a chemical substance in food which in minute quantities is essential for metabolism. It is clear that vit D does not fulfil these criteria but rather those for a hormone which is defined as a chemical substance produced in one part of the body and which stimulates functional activity in another.10 A more intriguing question is how furred and feathered animals activate 7-dehydrocholesterol, where UV is blocked from reaching the skin. It has been demonstrated that vit D is generated in the oily secretions on the fur and feathers, activated by the UV rays of the sun and harvested orally during grooming.11
Research into the biochemical actions of vit D3 in the human body has been an area of intense interest during the past decade. The list of diseases allegedly associated with vit D deficiency is subsequently rapidly expanding. This comes as no surprise as it has been demonstrated that vit D3 influences the functions of over 200 genes of the human genome directly, increasing the susceptibility to a wide range of abnormal tissue reactions when deficient. Besides the vit D3 receptors in the intestine and bone, vit D3 receptors have been demonstrated in the brain, prostate, breast, colon, cells of the immune system, vascular smooth muscle and cardiac muscle cells.12-14 The following brief overview focuses on recent advances and controversies in the study of disease states associated with a vit D deficiency.
Bone health
The role of vit D in the maintenance of the calcium balance of the skeleton is the classical activity which has been researched exhaustively over the past 70 years. The mechanisms entail its promotion of calcium absorption in the intestine and facilitation of proper function of parathyroid hormone thereby maintaining basic metabolic activities requiring adequate serum calcium and phosphate concentrations. The impact of a vit D deficiency is well publicised and manifests as rickets in children and osteomalacia after skeletal growth has ceased. It is not the purpose of this paper to elaborate on skeletal biochemical changes associated with vit D deficiency states and readers are referred to other publications for this purpose.15
Immune system
Vit D3 enhances the phagocytic capacity of macrophages through mitochondrial activation. It also stimulates killer T-lymphocytes through the activation of vit D3 receptors on their cell surfaces thereby improving their antigen neutralising capacity.16-18 Vit D3 furthermore increases the production of an antimicrobial peptide, cathelicidin, in response to a microbial trigger.18,19 This provides scientific evidence for the successes achieved by Niels Finsen more than 100 years ago in applying phototherapy to patients suffering from smallpox and lupus vulgaris. A lower concentration of vit D3 due to lack of UV exposure may be one of the reasons for the higher incidence rate of influenza infection during the winter.20 Evidence points to an association between vit D deficiency and multiple sclerosis in women21 due to vit D's alleged autoimmune suppressive effect.22 In a study on 206 patients with early inflammatory polyarthritis an inverse relation between 25(OH) vit D concentrations and the Activity Score 28-joint Assessment Scale was found.23 Preliminary findings on the associations between vit D deficiency and autoimmune diseases like autoimmune interstitial lung disease, lupus and rheumatoid arthritis are promising.24 More research is however required in order to verify the scientific basis of these observations.
Glucose metabolism
In a study of more than 10 000 children, daily vit D supplementation with doses of 2 000 IU was found to be associated with a 78% reduced risk of developing type 1 diabetes compared to supplementation with lower doses.25 A metaanalysis of four studies of a large cohort of children receiving vit D supplementation demonstrated a 29% reduction in the risk for developing type 1 diabetes compared to non-supplemented children.26 A ten-year study of 524 non-diabetic adults demonstrated an inverse relationship between serum 25(OH) vit D concentrations, future hyperglycaemia and insulin resistance.27 The link between hypo-vitaminosis D and adiposity, diabetes and calcified atherosclerotic plaque has recently been demonstrated.28 It may partly be explained by the propensity for vit D to dissolve in body fat, rendering low concentrations of free vit D available for metabolic activation in obese patients.
Cardiovascular disease
A report of the National Health and Nutrition Survey which was based on nearly 5 000 participants, found that low concentrations of 25(OH) vit D were associated with an increased risk for peripheral arterial disease.29 Although still clouded in controversy, several studies demonstrated a link between low 25(OH) vit D concentrations and cardiovascular events in hypertensive patients,13 myocardial infarction30 and all-cause cardiovascular mortality.31 Knowledge in this field will undoubtedly progress in the near future.
Malignant disease
An increasing number of studies associate vit D deficiency with a higher risk of developing certain malignancies. Analysis of a large number of cases found a significantly lower risk for breast cancer in women with normal serum 25(OH) vit D concentrations.32,33 In a separate study, vit D supplementation has been reported to reduce the risk for breast cancer.34 Vit D mediated facilitation of the immune response against transformed cells, the direct binding of vit D to receptor sites on transformed cells or other as yet undisclosed mechanisms may be implicated. Molecular evidence in support of epidemiological studies on large numbers of cancer patients that indicate significant reductions in the risks for colon, ovarian, kidney and breast cancers when normal serum concentrations of 25(OH) vit D is maintained,35 is certain to be an exciting field of research in the future. Not all agree with these preliminary findings and question statistical methodologies, non- randomised patient selection and lack of data as major flaws in some of the reports not cited in this overview. Although population genetics should not be negated, the different risks for the development of malignancies in geographic regions that experience less sun exposure may well be the result of lower population averages of serum 25(OH) vit D concentrations in such regions. It should be cautioned however that there is an undisputed risk for the development of malignancies of the skin with chronic sun and sun-bed exposure36 and as with many other aspects of life, a balanced approach to sun exposure is required in order to remain within safe limits. Before vit D supplementation is universally accepted as a preventative measure for malignant diseases, detailed mapping of the metabolic actions of vit D3 is required.
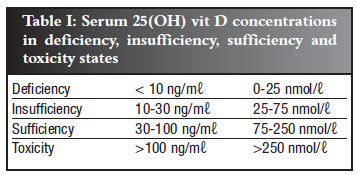
Normal serum concentrations
Vit D status is assessed by measuring the serum concentration of 25(OH) vit D. The normal concentrations and reference ranges are reflected in Table I. An estimated one billion people worldwide do not reach the minimum optimal serum concentration of 30 ng/ml.12 Vit D supplementation should not be prescribed unless the serum concentration has been found to be deficient or insufficient (Table I).
Vitamin D-containing food
Although vit D is synthesised and activated in the body as outlined, several external sources are available that would reduce the need for UV activation of 7-dehydrocholesterol in the skin in order to meet the adult requirement of 2 000 IU 25(OH) vit D per day. (Breastfed infants should receive 400 IU per day until weaned. The same dosage is recommended for children and teens who drink less than 500 ml vit D fortified milk per day.) These recommendations are constantly updated by the Institute of Medicine's Food and Nutrition Board of the USA. The external sources of vit D (cholecalciferol and ergocalciferol) are briefly listed below:37
• Cholecalciferol tablets (available in a wide range of concentrations of up to 50 000 IU per tablet)
• Wild salmon
• Mushrooms (ergocalciferol) particularly those that were exposed to UV
• Mackerel (particularly those that are caught wild. Breeding in captivity reduces its value as a source of vit D)
• Cod liver oil (beware of vit A toxicity)
• Tuna and sardines
• Milk, yogurt, beef or calf liver and egg yolks
Vit D toxicity
Vit D toxicity has not been reported to result from exposure to natural sunlight due to the intricate activation pathway with its negative feedback mechanisms. Vit D toxicity is however theoretically possible by taking chronic daily excessive amounts (in the order of 40 000 IU per day or more8 ) of vit D orally or using UV devices. Little information is however available on the effects (if any) of vit D toxicity. The National Institute of Health set the maximum upper limit of the serum concentration of 25(OH) vit D arbitrarily on 100 ng/m (Table I) and the daily intake on 2 000 IU for adults. This value will undoubtedly be increased as 30 minutes of full body sun exposure is alleged to produce 10 000 IU vit D. 37
(Table I) and the daily intake on 2 000 IU for adults. This value will undoubtedly be increased as 30 minutes of full body sun exposure is alleged to produce 10 000 IU vit D. 37
References
1. http://nobelprize.org/nobel_prizes/medicine/laureates/1903/finsen-bio.html [ Links ]
2. http://en.wikipedia.org/wiki/Battle_Creek_Sanitarium [ Links ]
3. McCullum EV, Simmonds N, Becker JE, Shipley PG. Studies on experimental rickets. XXI. An experimental demonstration of the existence of a vitamin which promotes calcium deposition. J Biol Chem 1922;53:293-312. [ Links ]
4. Windaus A, Hess A. Sterine und antirachitisches Vitamin. Nachrichten von der Gesellschaft der Wissenschaften zu Gottingen: 175-84. [ Links ]
5. http://jn.nutrition.org/cgi/content/full/134/6/1299 [ Links ]
6. Windaus A, Bock, F. Über das provitamin aus dem Sterin der Schweineschwart. Z Physio Chem 1937;245:168-70. [ Links ]
7. Vellus L, Amiard G, Goffinet B. Le précolciferol. Structure et photochimie. Son role dans le genése di calciferol, et des photoisoméres de l'ergostérol de l'ergostérol. Bull Soc Chim France 1955;22:1341-48. [ Links ]
8. http://www.solarcsystems.com/vitamin-d-phototherapy-faq.htlm [ Links ]
9. Hollis BW. Seminar on 25 OH Vitamin D: From bone to general health. Midrand. 22 October 2009. [ Links ]
10. Sykes JB (ed). The Concise Oxford Dictionary of current English. Oxford: Oxford University Press; 1979 [ Links ]
11. Stout SD, Agarwal SC, Stout SD. Bone loss in osteoporosis: an anthropological perspective. New York: Kluwer Academic/Plenium Publishers; 2003: 203-79. [ Links ]
12. Holick MF. Vitamin D deficiency. N Engl J Med 2007;357:266-81. [ Links ]
13. Wang TJ, Pencina MJ, Booth SL, Jaques PF. Vitamin D deficiency and risk of cardiovascular disease. Circulation 2008;117:503-11. [ Links ]
14. http://www.ox.ac.uk/media/news_stories/2010/240810.html [ Links ]
15. Smith R, Wordsworth P (eds). Clinical and biochemical disorders of the skeleton Oxford: University Press; 2008: 141-3. [ Links ]
16. Gombart AF, Borregaard N, Koeffler HP. Human cathelicidin antimicrobial peptide (CAMP) gene is a direct target of the vitamin D receptor and is strongly upregulated in myeloid cells by 1,25-dihydroxyvitamin D3. FASEB J 2005;19:1067-77. [ Links ]
17. Von Essen MR, Kongsbak M, Schjerling P, Olgaard K, Ødum N, Geisler C. Vitamin D controls T cell antigen receptor signaling and activation of human T cells. Nat Immonol 2010;11:344-49. [ Links ]
18. Martineau AR, Wilkinson RJ, Wilkinson KA, Newton SM, et al. A single dose of vitamin D enhances immunity to mycobacteria. Am J Resp Crit Care Med 2007;176:208-13. [ Links ]
19. Muhe L, Lulseged S, Mason KE, Simoes EA. Case control study of the role of nutritional rickets in the risk of developing pneumonia in Ethiopian chidren. Lancet 1997;349(9068):1801-4. [ Links ]
20. Lowen AC, Mubareka S, Steel J, Palese P. Influenza virus transmission is dependant on the relative humidity and temperature.2007; http://www.ncbi.nlm.nih.gov/pubmed/17953482 [ Links ]
21. Kragt J, van Amerongen b, Killestein J, Dijkstra C, Uitdenhaag B, et al. Higher levels of 25-hydroxyvitamin D are associated with a lower incidence of multiple sclerosis only in women. Mult Scler 2009;15:9-15. [ Links ]
22. Munger KL, Levin LI, Hollis BW, Howard NS, Ascherio A. Serum 25-hydroxyvitamin D levels and risk of multiple sclerosis. JAMA 2006;296:2832-8. [ Links ]
23. Patel S, Farragher T, Berry J, Bunn D, Silman A, Symmons D. Association between serum vitamin D metabolite levels and disease activity in patients with early inflammatory polyarthritis. Arthritis Rheum 2007;56:2143-49. [ Links ]
24. http://www.lef.org/LEFCMS/aspx/PrintVersionMagic.aspx?CmsID=117825 [ Links ]
25. Hypponen E, Läärä E, Reunanen A, Järvelin MR, Vitanen SM. Intake of vitamin D and risk of type 1 diabetes: a birthcohort study. Lancet 2001;358:1500-3. [ Links ]
26. Zipits CS, Akobeng AK. Vitamin D supplementation in early childhood and risk of type 1 diabetes; a systematic review and meta-analysis. Arch Dis Child 2008;93:512-7. [ Links ]
27. Forouhi NG, Luan J, Cooper A, Boucher BJ, Wareham NJ. Baseline serum 250hydroxy vitamin D is predictive of future glycemic status and insulin resistance: the Medical Research Council Ely Prospective Study 1990-2000. Diabetes 2008;57:2619-25. [ Links ]
28. Freedman BI, Wagenknecht LE, Hairston KG, Bowden DW, Carr JJ, et al. Vitamin D, adiposity, and calcified atherosclerotic plaque in African-Americans. J Clin Endocrin Metab 2010;95:1076-83. [ Links ]
29. Melamed ML, Munter P, Michos ED, Uribarri J et al. Serum 25-hydroxyvitamin D levels and the prevalence of peripheral arterial disease: results from NHANES 2001 to 2004. Arterioscler Thrombosis Vasc Biol 2008;28:1179-85. [ Links ]
30. Giovannucci E, Liu Y, Hollis BW, Rimm EB. 25-Hydroxyvitamin D and risk of myocardial infarction in men. Arch Intern Med 2008;168:1174-80. [ Links ]
31. Dobnig H, Pilz S, Schnarnagl H Renner W, Seelhorst U et al. Independent association of low serum 25-hydroxyvitamin D and 1,25 dihydroxyvitamin D levels with all-cause and cardiovascular mortality. Arch Intern Med 2008;168:1340-49. [ Links ]
32. Garland CF. Vitamin D and prevention of breast cancer: pooled analysis. J Steroid Biochem Mol Biol 2007;103:708-11. [ Links ]
33. Abbas S. Serum 25-hydroxyvitamin D and risk of post menopausal breast cancer - results of a large case-control study. Carcinogenesis 2008;29:93-99. [ Links ]
34. Lappe JM. Vitamin D and calcium supplementation reduces cancer risk: results of a randomized trial. Am J Clin Nutr 2007;85:1586-91. [ Links ]
35. Wheatherby C. Vitamin D may lower risk for ovarian, breast, kidney and colon cancers. http://chetday.com/cancervitamin.htm [ Links ]
36. http://www.cancersupportivecare.com/Survivorship/sun.html [ Links ]
37. http://www.webmd.com/osteoporosis/features/the-truth-about-vitamin-d? pages 1-3 [ Links ]
 Reprint requests:
Reprint requests:
Prof EJ Raubenheimer
P O Box D24
Medunsa Campus University of Limpopo
0204
Email: ejraub@ul.ac.za
The content of the article is the sole work of the author.
No benefits of any form have been received from a commercial party related directly or indirectly to the subject of this article.


{kind=link}