










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSA Orthopaedic Journal
versión On-line ISSN 2309-8309
versión impresa ISSN 1681-150X
SA orthop. j. vol.10 no.1 Centurion ene. 2011
EXPERT OPINION ON PUBLISHED ARTICLES
Similar effects of disease-modifying anti-rheumatic drugs, glucocorticoids and biologic agents on radiographic progression of rheumatoid arthritis
Meta-analysis of 70 randomised placebo-controlled clinical studies, including 112 comparisons.
Niels Graudel and Gesche Jurgens
Arthritis and Rheumatism, 2010, 62(10), 2852-63
The treatment of rheumatoid arthritis has been revolutionised by the advent of biological (targeted) therapies. Developed countries are engaged in debate about introducing these newer agents as first-line therapies while developing countries are denied access to these drugs due to expense. In addition, the risk of opportunistic infections such as deep fungi and TB has raised concern about their use. Many rheumatologists in developing countries have wondered whether their patients are being denied optimum care, as a result.
These authors have performed a meta-analysis of 70 studies comparing biologicals and conventional DMARDs (disease-modifying anti-rheumatic drugs) in the treatment of rheumatoid arthritis (RA). Data from 70 trials (112 comparisons, 16 interventions) were summarised in 21 meta-analyses. Compared with placebo, the percentage of the annual radiographic progression rate (PARPR) was 0.65% smaller in the single DMARD group (p<0.002) and 0.54% smaller in the glucocorticoid (GC) group (p<0.00001). Compared with single DMARD treatment, the PARPR was 0.62% smaller in the combination DMARDgroup (p<0.001) and 0.61% smaller in the biologic plus methotrexate (MTX) group (p<0.00001). The effect of a combination of two DMARDs plus step-down GC did not differ from the effect of a biological agent plus MTX.
The authors conclude that biologic agents should still be reserved for patients whose RA is resistant to DMARD therapy. Future trials of the use of biologic agents should compare such agents with combination treatments including DMARDs and GC.
These recommendations are in keeping with current practice in treating RA in South Africa and are consistent with the recommendations of the South African Rheumatism and Arthritis Association (SARAA).
Reviewer: Prof Asgar Ali Kalla
Professor of Rheumatology
University of Cape Town
South Africa
Inflammatory blood laboratory levels as markers of prosthetic joint infection: a systematic review and meta-analysis
Berbari E, Mabry T, Tsaras G, Spangehl M, Erwin PJ, Murad MH, Steckelberg J, Osmon D.
Bone Joint Surg Am. 2010 Sep 1; 92(11):2102-109
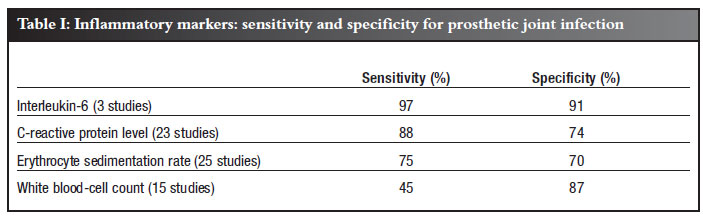
Deciding whether a painful prosthetic joint is due to infection or not can be problematic. Frequently we rely on a combination of inflammatory markers, such as the white blood-cell count, the erythrocyte sedimentation rate, serum C-reactive protein levels and, less commonly and more recently, serum interleukin-6 levels.
Interleukin-6 is a product of monocytes and macrophages, which induces the production of acute phase proteins including C-reactive protein. The levels of both these substances increase after uncomplicated surgery. Interleukin-6 levels return to normal values after two to three days and CRP levels after two to three weeks.
This meta-analysis was performed by authors from the Mayo Clinic and indexed the standard electronic databases from 1950 to 2009. This review summarises the evidence they obtained on the accuracy of these markers.
Thirty studies were included, with a total of 3 909 revision total hip or knee arthroplasties. The prevalence of prosthetic joint infection was 32.5% (1 270 of 3 909).
The pooled sensitivity and specificity were evaluated using a statistical model (Table I).
The authors concluded that interleukin-6 has the highest accuracy for the diagnosis of prosthetic joint infection.
This study has all the usual shortcomings of a meta-analysis and can never follow the rules of hard science. It is only a statistical examination of scientific studies, not an actual scientific study itself.
It is clear, however, that the use of measuring interleukin-6 levels may be useful and is likely to be the subject of further studies. The facilities to measure interleukin-6 should become more readily available in South Africa in the future.
Reviewer: Johan van der Merwe
First Specialist
Dept Orthopaedic Surgery
University of the Free State
Tel: (051) 4052242
Red blood cell transfusion strategies
MA Blajchman, PC Hébert
Transfus Clin Biol. 2001 Jun; 8(3):207-10
The administration of allogenic blood, most notably for volume resuscitation and augmentation of oxygen delivery, is an integral part of the daily activities of all orthopaedic surgeons. However it is interesting that there are inconsistent criteria regarding administration policies among practitioners. In addition there appears to be a lack of awareness of all the potential hazards, in particular the more recently published ones, associated with the administration of homologous red blood cells.
This article reviews recent trends in RBC transfusion practice, evaluating the use and role of clinical guidelines, as well as the scientific basis for the use of RBC transfusion thresholds to guide evidence-based clinical transfusion practice.
In this study the authors review the clinical practice guidelines for the administration of allogeneic RBCs that had been developed by a variety of national agencies. A review of published guidelines at that time found that the recommendations contained in most of the guidelines relied heavily on expert opinion based on clinical judgement or perceived specific risk factors and not through the use of evidence-based input as obtained from the published literature. Although the intended patient populations varied considerably, one guideline recommended a specific transfusion trigger, most recommended a range of thresholds and one guideline advocated only the use of clinical judgement without indicating a specific transfusion trigger. A number of reviewed studies reported variations in transfusion practice including interinstitutional discrepancy, and variation within cohorts of patients with specific disease categories, clinical settings, and/or surgical procedures
A literature review by Calder etal of allogeneic RBC transfusion practice indicated that the rates of unnecessary or inappropriate RBC transfusions ranged from 4 to 66%. This apparent lack of adherence to clinical practice guidelines led to a variety of strategies to gain compliance with coherent administration practices including advocacy of education (can include one-to-one meetings with physicians; teaching sessions and scheduled conferences with medical and ancillary staff; and the participation of transfusion medicine personnel in daily clinical rounds) while other authors have suggested the use of intra-operative transfusion algorithms; and the implementation of quality assurance programmes, or auditing systems.
The haemoglobin concentration has been the most commonly used trigger for allogeneic RBC transfusions, even though many guidelines advise against using such. Historically, the most frequent trigger to transfuse is a haemoglobin concentration of 100 g/l (10 g%) despite the lack of evidence supporting the use of this arbitrary value. The use of the haematocrit was alluded to but no further information was presented.
In a study by Hébert et al of 5 298 consecutive patients variation in transfusion practice was more pronounced in sicker patients, indicating that critical-care physicians tend to individualise decisions based on patients' disease severity. It was suggested that conflicting evidence and practical implementation of published guidelines may have impacted on the observed variation. Inter-institutional practice variations were identified as a significant independent predictor of the transfusion threshold.
In a second randomised control trial, Hébert et al compared a liberal allogeneic RBC transfusion strategy (trigger = 10 g%) with a restrictive strategy (trigger = 7 g%) in 830 critically ill patients. The authors found that the more restrictive transfusion strategy was at least equivalent, if not superior, to the liberal transfusion strategy for critically ill patients; with the possible exception of patients with unstable angina or myocardial infarction. The authors report on four smaller randomised control trials which also sought to identify the optimal transfusion indication by comparing liberal and restrictive allogeneic RBC transfusion strategies in different patient populations. All four failed to identify a statistically significant difference in clinical outcome between the restrictive and liberal RBC transfusion strategies.
A number of messages can be taken from this paper, even though it was published in 2001. From this review it would appear that we as practitioners lack a consistent blood administration policy. Has much changed to accommodate this observation over the past decade? Perhaps more importantly what emerges here is the apparent advantage that a restrictive blood administration policy has over a more liberal one. It is still common that the trigger for transfusion in our postoperative patients is a haemoglobin value of 9 g% or even 10 g% (haematocrit = 30). The evidence presented in this paper suggests that much lower haemoglobin levels (down to 7 g%) are tolerated, even by cardiac patients.
Consultation with junior and senior colleagues suggests limited application of the recommendations implicit in this paper and the inconsistencies reported, persist.
Reviewer: Prof J Walters
Department of Orthopaedics
University of Cape Town


{kind=link}