










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSA Orthopaedic Journal
On-line version ISSN 2309-8309
Print version ISSN 1681-150X
SA orthop. j. vol.10 n.1 Centurion Jan. 2011
CLINICAL ARTICLE
Do some of the newer COX-2 inhibitors cross-react with sulfonamide antibiotics? An overview
GL Muntingh
B Pharm, MSc(Med), PhD. Department of Pharmacology, School of Medicine, Faculty of Health Sciences, University of Pretoria
ABSTRACT
The professional information leaflets of three locally available specific cyclooxygenase-2 inhibitors indicate that these drugs are contraindicated in persons with a known allergy to sulfonamides. There are many concerns about cross-allergenicity between sulfonamide antibiotics and non-antibiotic sulfonamide-containing drugs including the sulfones, and these concerns continue to complicate drug therapy. Several elegant investigations have demonstrated lack of interaction between the sulfonamide group and either cellular or humoral immunity. The immunologic determinant of type I immunologic responses to sulfonamide antibiotics are the N1 heterocyclic ring, and non-antibiotic sulfonamides including the sulfones lack this structural feature. Reactive sulfonamide metabolites contribute many non-type I hypersensitivity responses to sulfonamide antibiotics. Metabolite formation demonstrates stereospecificity to the N4 amino nitrogen of the sulfonamide antibiotics, a structure not found on any non-antibiotic sulfonamide drugs and is also lacking in the sulfones. Apparent cross-reactivity responses to sulfonamide-containing drugs likely represent multiple concurrent, rather than linked, drug hypersensitivities.
Introduction
A drug product label contains intion, adverse drug reactions (ADRs) and contraindications. Although the information contained in the efficacy and administraformation on efficacy, administration sections is often based on clinical trial data, contraindications or warnings may be based on individual case reports or extrapolated from previous experience with similar agents. Because the available scientific data may be disparate from the information contained within the product label, confusion arises concerning the potential of certain clinical implications. As an example, at the time of writing, a perusal of the South African MIMS (September 2010) indicated that there are three locally available specific cyclooxygenase-2 inhibitors (COXIBs) namely, celecoxib, etoricoxib (indicated for the treatment of rheumatoid arthritis and osteoarthritis) and parecoxib (indicated for the treatment postoperative pain) that all contain a sulfonamide substituent. It is thought that because of this structural component, the professional package inserts (PIs) of all three mentioned COXIBs indicate that these drugs are contraindicated in persons with a known allergy to sulfonamides. Although many references suggest that there is cross-reactivity between various sulfonamide medications, this has not been substantiated in the literature either from a structural framework (e.g. metabolism, chemical structure) or from a clinical standpoint. This article will discuss the similarity and differences in structure between the various sulfonamide medications. Differences in metabolism will also be highlighted between sulfonamide antimicrobials and other sulfonamide-containing compounds such as celecoxib and etoricoxib.
Sulfonamides
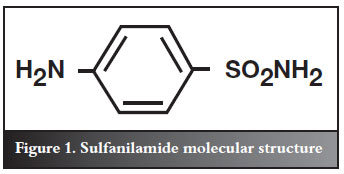
There is often confusion surrounding the term 'sulfa allergy'. Sulfa allergy strictly refers to those patients who have a history of hypersensitivity to sulfonamide antibiotics.1 The prevalence of true hypersensitivity or allergic reactions to sulfonamide antibiotics is about 3-5%.1 Sulfa drugs, also called sulfonamides, are any members of a group of synthetic antibiotics containing the sulfanilamide molecular structure (Figure 1).2
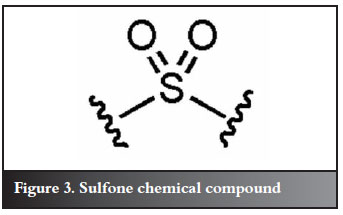
Sulfonamide agents all contain structurally similar paminobenzoic acid rings and include: antimicrobials (trimethoprim or sulfamethoxazole), sulfonylureas, furosemide, thiazide diuretics, chlorthalidone, sulfasalazine, diazoxide, and some of the newer COX-2 selective inhibitors, e.g. celecoxib.3 No interaction between the human immune system and the sulfonamide functional group has been demonstrated. The immunologic determinant of type I, immediate hypersensitivity responses to sulfonamide antibiotics is the N1 heterocyclic ring (Figure 2).4,5 Non-antibiotic sulfonamides do not contain this structural feature. The other major difference between sulfonamide antimicrobials and other sulfonamide-containing medications is that sulfonamide antimicrobials also contain an aromatic amine group at the N4 position; this group is not found with non-aromatic amine-containing sulfonamides.
This allows for division of the sulfonamides into two groups: aromatic amines (i.e. sulfonamide antimicrobials) and non-aromatic amines.6 Non-type I, hypersensitivity responses to sulfonamide antibiotics are largely attributable to reactive metabolites that may cause either direct cytotoxicity or an immunologic response. Formation of these metabolites is a stereospecific process that occurs at the N4 amino nitrogen of the sulfonamide antibiotics, a structure that is absent on any non-antibiotic sulfonamide drugs.5 The stereospecificity of these reactions implies that crossreactivity with non-antibiotic sulfonamide-containing drugs is highly unlikely; this assertion is supported by recent literature. In fact, a recent study investigating the differences in risks to allergic reaction to sulfonamide antibiotic drugs based on the chemical structure, confirmed that the N1 heterocyclic ring needs to be present to elicit an allergic reaction.5 In this study, sulfonamides were classified according to the presence/absence of a stereospecific, N1 substituent (N1(+)/(-)) and/or an arylamine (N4(+)/(-)) and it was found that specifically, current use of N1(+) N4(+) sulfonamide drugs was associated with the outcome. Current use of N1(+) N4(-) and N1(-) N4(-) sulfonamide drugs was also associated with the occurrence of allergic reactions.7
Based on these studies then, cross-reactivity between these sulfonamide antibiotics and non-antibiotic sulfonamides is therefore highly unlikely.
Furthermore, sulfonamide-containing drugs should not be confused with sulfur, sulfate or sulfite moieties. These entities lack the aromatic amine, p-aminobenzoic ring and N1-substituent. Therefore, the presence of sulfur, sulfates (salts or esters of sulfuric acid) or sulfites (salts or esters of sulfurous acid (H2SO3)) within a formulation does not constitute a risk to patients hypersensitive to sulfonamides. Sulfites are primarily used as preservatives in many injectable drugs such as gentamycin, metoclopramide, doxycycline, vitamin-B complex, local anaesthetics, and the recently manufactured generic propofol, and have not been shown to cross react with sulfonamides or sulfones in any published reports.8,9
Sulfones
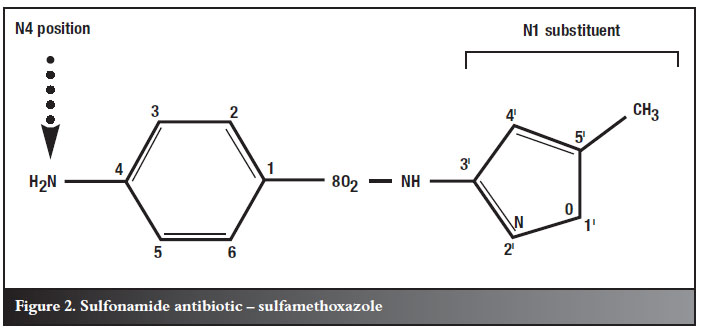
A sulfone is a chemical compound containing a sulfonyl functional group attached to two carbons (Figure 3).10
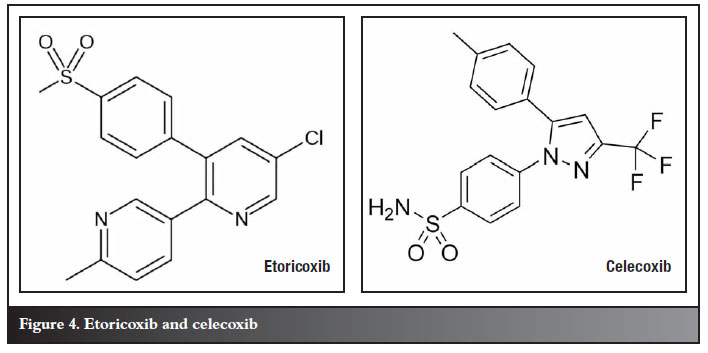
It is important to note that sulfone-containing products are non-antibiotic sulfonamides and therefore also lack the N1 heterocyclic ring. Recent investigations into the COX-2 inhibitor, celecoxib, which also lacks the aromatic amine and N1-substituent, did not show any cross-reaction in patients with a sulfonamide antibiotic allergy.11,12 Another example of a sulfone-containing agent is the newer COX-2 inhibitor, etoricoxib (Figure 4),13,14 which is a sulfone and also lacks the aromatic amine and N1-substituent.
It seems most authors agree that non-antibiotics are less likely to cause severe reactions, and that the chemical differences between sulfa-antibiotics and non-antibiotics make true cross-reactivity extremely unlikely. An extensive literature survey found only one case report of anaphylaxis caused by furosemide;15 the authors were not able to prove that the allergen was in fact conclusively chemically related to the sulfa moiety.
Perhaps the most reassuring evidence comes from Strom et al,1 who elegantly turned the United Kingdom General Practice Research Database into a retrospective cohort study (level II evidence) to show that giving sulfa non-antibiotics to patients with a history of sulfa (antibiotic) allergy carries little risk of cross-reactivity. The authors reviewed the data of 969 patients who had had allergic reactions to sulfonamide antibiotics and of 19 257 patients who had not. All these patients subsequently received sulfonamide non-antibiotics. For this study, 'allergy' was defined very broadly and included development of eczema and various unspecified adverse effects within a full month of receiving the medication in question, making under-reporting bias unlikely. Although Strom and colleagues found that patients allergic to sulfonamide antibiotics were more likely than non-allergic patients to react to sulfonamide non-antibiotics (9.9% vs 1.1%), they also found that the rate of reaction was even greater among patients allergic to penicillin who received sulfonamide non-antibiotics (14.2%). Penicillins do not have a sulfonamide moiety, so the researchers argued that any sulfonamide cross-reactivity appears predominantly related to a greater predisposition to allergic reactions in general among patients allergic to sulfonamide antibiotics, rather than to a specific sulfa hypersensitivity.
After a thorough critique of the literature by Johnson et al, it appears that the dogma of sulfonylarylamine cross-reactivity with non-sulfonylarylamines is not supported by the data. While many of the case reports on the surface support the concept of cross-reactivity, on closer examination the level of evidence in many of the cases does not conclusively support either a connection or an association between the observed cause and effect.
Conclusion
The stereospecificity of sulfone and nonantibiotic sulfonamide drugs implies that crossreactivity with sulfonamide antibiotics is highly unlikely; this assertion is supported by recent literature. Thus, one is able to conclude that it is highly unlikely that COX2 inhibitors, e.g. etoricoxib and celecoxib, which do not contain a sulfonamide moiety, will show any crossreactivity in patients with true sensitivity to sulfonamide antibiotics.
References
1. Strom BL et al. Absence of crossreactivity between sulfonamide antibiotics and sulfonamide nonantibiotics. NEJM. 2003; 349(17): 1628-35. [ Links ]
2. http://www.britannica.com/EBchecked/topic/572427/sulfadrug. [ Links ]
3. Ponka D. Approach to managing patients with sulfa allergy: Use of antibiotic and nonantibiotic sulfonamides. Can Fam Physician. 2006; 52: 1434-38. [ Links ]
4. Bracket CC. Sulfonamide allergy and crossreactivity. Current Allergy and Asthma Reports. 2007; 7(1): 41-48. [ Links ]
5. Carolyn C. Brackett, Pharm.D., Harleen Singh, Pharm.D., and John H. Block, Ph.D. Likelihood and Mechanisms of CrossAllergenicity Between Sulfonamide Antibiotics and Other Drugs Containing a Sulfonamide Functional Group. Pharmacotherapy 2004; 24(7):856-70. [ Links ]
6. Hemstreet BA., Page RL. Sulfonamide Allergies and Outcome Related to Use of Potentially CrossReactive Drugs in Hospitalized patients. Pharmacotherapy. 2006; 26(4): 551-57. [ Links ]
7. Verdel BM, Souverein PC, Egberts AC, Leufkens HG. Difference in risks of allergic reaction to sulfonamide drugs based on chemical structure. Ann Pharmacother. 2006 Jun;40(6):1040-46. [ Links ]
8. Murhammer J., Ross M., Bebout K. Sulfonamide CrossSensitivity Reactions. Virtual Hospital. www.healthcare.uiowa.edu/pharmacy/rxupdate/2003/07rxu.html. [ Links ]
9. Gonyeau M. Identifying cross reactivity among commonly prescribed drug classes MSHP Newsbrief 1 2000; 1: 12, 9. [ Links ]
10. http://commons.wikimedia.org/wiki/File:Sulfonyl_group.png. [ Links ]
11. Shapiro L.E, Knowles S.R, Weber E, Neuman M.G., Shear N.H. Safety of Celecoxib in Individuals Allergic to Sulfonamide: A Pilot Study. Drug Safety, 26, Number 3, 2003, 187-95(9). [ Links ]
12. Knowles S., Shapiro L., Shear NH. Should celecoxib be contraindicated in patients who are allergic to sulfonamides? Revisiting the meaning of 'sulfa' allergy. Drug Saf. 2001; 24(4): 239-47. [ Links ]
13. http://en.wikipedia.org/wiki/Image:Etoricoxib.svg. [ Links ]
14. http://commons.wikimedia.org/wiki/File:Celecoxib_structure.png. [ Links ]
15. Hansbrough JR, Wedner HJ, Chaplin DD. Anaphylaxis to intravenous furosemide. J Allergy Clin Immunol 1987;80:538-41. [ Links ]
16. Johnson et al. Sulfonamide crossreactivity: Fact or fiction? Ann Pharmacother Vol. 39, No. 2, pp. 290-93. [ Links ]
 Reprint requests:
Reprint requests:
Dr GL Muntingh
Dept of Pharmacology
PO Box 2034
University of Pretoria
Pretoria, 0001
Email: george.muntingh@up.ac.za
The content of this article is the sole work of the author. No benefits of any form have been received from a commercial party relating directly or indirectly to the subjectof this article.
Note from the Editor-in-Chief: A world-renowned authority in this field prefers to avoid prescribing the remedies referred to for patients who have suffered anaphylaxis or shown acute skin reactions to anyof the remedies, irrespective of whether it is a sulfonamide or a sulfone.


{kind=link}
{kind=link}