










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSA Orthopaedic Journal
On-line version ISSN 2309-8309
Print version ISSN 1681-150X
SA orthop. j. vol.9 n.4 Centurion Jan. 2010
CLINICAL ARTICLE
Risser sign – trends in a South African population
Z MayetI; M LukheleII; N MohammedIII
IMBChB, Registrar in Orthopaedics, University of the Witwatersrand
IIMBChB, MMed FCS(Orth)SA, Professor and Head of Division of Orthopaedics, University of Witwatersrand
IIIMBChB, Registrar in Radiology, University of the Witwatersrand
ABSTRACT
INTRODUCTION: In scoliosis management the five stages of the Risser sign on the iliac crest have been widely used as a tool to assess skeletal age and remaining spinal growth. However, as with other markers of skeletal age, it is under the influence of genetic and environmental factors. Proof of this was given by Risser, who observed that children in warmer climates developed earlier. Numerous other authors have also shown differences for other measures of maturity between different race groups.
OBJECTIVE: This study was aimed at determining the trends of Iliac crest apophyseal ossification as represented by the Risser sign in the South African population and how it compares with that published by Scoles et al in their population group.
METHOD: Radiographs of patients between the ages of 8 to 20 years undergoing abdominal X-rays for abdominal pains at our teaching hospitals were collected and assessed by two independent observers for the Risser sign. X-rays of patients with Risser stage 0, skeletal abnormalities and conditions which can affect skeletal growth and maturity were excluded from the study. The Risser stage, the ages and the race of the patients were observed and documented.
RESULTS: A total of 743 abdominal X-rays were collected; of those 280 X-rays were excluded as per exclusion criteria leaving 463 X-rays to analyse. Of the 463 X-rays available, 292 were for black patients, 117 whites, 42 coloureds, 11 Indians and 1 Chinese. The average age of Risser stage 1, 2, 3, 4 and 5 were 12.75, 15.38, 15.83, 16.38, and 17.06 years respectively. The girls tended to be of a younger age group in all Risser stages. There were no statistically significant differences in average age of the Risser stages among the black and white population groups except for the white male in Risser stage 1 who had a younger age than the black population in the same Risser stage. The South African boys at Risser stage 1 were of a younger age when compared those published by Scoles et al in their population group.
CONCLUSION: The Risser sign can be applied equally among the South African population as no significant statistical differences between the major population groups were found in this study.
Introduction
Management of scoliosis is largely dependent on the magnitude of the curve as determined by the Cobb's angle. The decision, however, is complicated by the fact that scoliosis is a disorder of growth and is governed by the Hueter-Volkman principle, which states that the rate of growth of the physis is determined by the amount of pressure placed across it.1,2 This means that as the spine undergoes longitudinal growth, the magnitude of the curve progresses. The decision-making regarding modality of treatment is therefore determined by what the Cobb's angle is now, and what it will be in the future. Predicting the growth potential remaining for a child is very important in the management of scoliosis. There are a number of methods for the estimation of skeletal age, each having its own advantages and disadvantages. The commonly used methods are the Greulich and Pyle Atlas, the Tanner-Whitehouse and the Risser sign.3-7
The Greulich and Pyle method assesses hand and wrist films which correspond to a gender-specific standard in the atlas, and a certain bone age.4 There is however some amount of difficulty in matching patients' X-rays to standards in the atlas and substantial user variability was found. Secondly in the Atlas of Greulich and Pyle it is highlighted that published trends of maturation and skeletal age may not be applicable to every population.5
The Tanner-Whitehouse method attempts to address this by assigning separate scores to the radius, ulna and bones of the hand.5,6 This was found to be a cumbersome method and was simplified into the DSA method by Sanders et al in 2008.6 The DSA method was found to correlate excellently with the curve-acceleration phase in scoliosis patients.
The Risser sign was first described by JC Risser following a ten-year follow-up of scoliosis patients beginning in 1936.7 He described the ossification of the iliac apophysis, and separated them into five stages, as ossification progressed across the four quadrants of the iliac blade (Figure 1). Risser found that completion of stage 5 occurred at an average of 14 years in girls (range 10–18 years) and 16 years in boys (range 10–20 years). He also found that iliac apophysis ossification took an average of one year to complete (range 7 months to 3 years). Risser also found differences in maturation between a scoliotic population in New York, as compared to his original population in Los Angeles, with the New York population having delayed maturation. He attributed this to the colder New York climate.7 Kotwicki has shown that to fully assess the Risser stage a lateral pelvis X-ray is necessary to exclude extension of the apophysis to the posterior superior iliac spine in that way excluding a Risser stage 4 where an assessment of a Risser stage 3 has been made.8 The Risser sign is arguably the most widely used method in the treatment of scoliosis.

A meta-analysis by Grivas et al showed that geographical latitudes had an influence in Europe, with age at menarche occurring later in more northern latitudes.9 This was also attributed to climatic differences. Ontell et al studied skeletal age in a heterogeneous population in California.10 They found differences between different ethnic groups, with the black population having a tendency to mature faster than other ethnic groups. The sexual maturity data based on Tanner staging and secondary sexual characteristics collected and assessed by the Third National Health and Nutrition survey in the United States found that black girls and boys started to mature early and that all children completed maturation at approximately the same age.11
Scoles et al conducted a review of radiographs from the Cleveland-based Brush–Bolton collection.12 In their study they did not calculate the average age of patients in Risser stage 0 because of the wide range of ages found in this stage. They showed that maturation of the iliac crest together with clinical observations of secondary sexual maturation permit an accurate assessment of skeletal maturation. More importantly the study provided us with standards for chronological ages for the Risser sign in a normal population.
Before we embarked on this study there were no published data on the trends of Risser stages from the African continent. This stimulated the authors to undertake the study on the trends of the Risser stages in the South African population. The hypothesis was that there are no differences on the Risser staging among the various population groups in South Africa.
Materials and methods
Permission to undertake the study was granted by the university ethics committee to undertake this study following the submission of a protocol. Abdominal X-rays that showed the pelvis performed on children between the ages of 8 years and 20 years were retrieved from the radiology department for the study. The abdominal X-rays were part of the investigations requested on patients who presented with acute and chronic abdominal pains in the hospital. X-rays of patients with conditions which may affect skeletal growth and maturity such as skeletal dysplasia, tumours, metabolic and endocrinology conditions were then excluded from the study. X-rays with Risser stage 0 were also excluded in line with the study of Scoles et al.12The pelvis was independently assessed by two third-year registrars-in-training. The one was an orthopaedics registrar (ZM) and the other was a registrar from the radiology department (NM). Where there was disagreement, the senior author (ML) acted as an umpire and provided the final Risser staging for that radiograph. The chronological age, sex and race were obtained from the hospital records and X-ray request form. The mean age of patients at each Risser stage was calculated looking at any differences between male and female in each stage. Comparison of the ages at each Risser stage were only made between the black and white population groups because of the small numbers in the other ethnic groups. The results were then compared to those of Scoles et al using the student T-test. A p-value of <0.05 was defined as significant.
Results
A total of 743 radiographs were assessed for the Risser staging. Nine were found to have skeletal abnormality and were excluded from the study leaving a total of 734. Twohundred-and-seventy-one (271) were found to be Risser stage 0. These were then excluded from further analysis as in the Scoles study.
The two primary observers were in disagreement in allocating the Risser stage in only 12 of the 463 radiographs analysed. This gave variability between the observers of 2.6%. Those radiographs were then assessed by the senior author, who determined the final Risser stage assignment.
On analysis according to race it was found that 292 were blacks, 117 whites, 42 coloureds, 11 Indians and 1 Chinese. The radiographs belonging to the Indian and Chinese populations were excluded from further analysis due to the small numbers.
Of the 451 radiographs 83 were classified Risser stage 1; 26 Risser stage 2; 57 Risser stage 3; 115 Risser stage 4; and 170 Risser stage 5. The mean ages for Risser 1, 2, 3, 4, and 5 were 12.75, 15.38, 15.83, 16.38 and 17.06 years respectively (Table I). In all the stages the females were of younger age than the males (Table I).

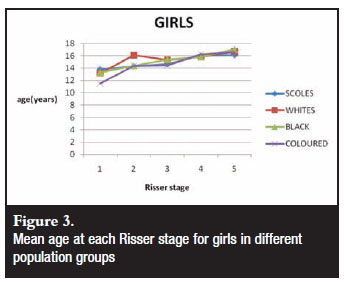
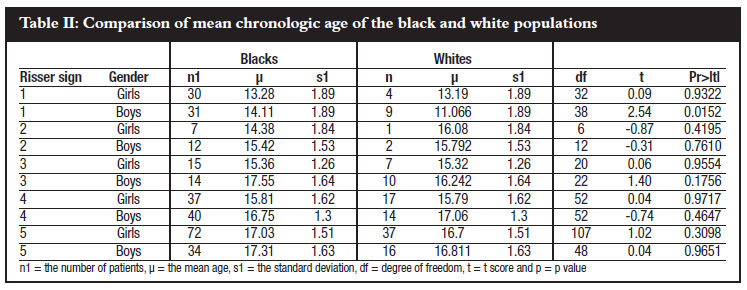
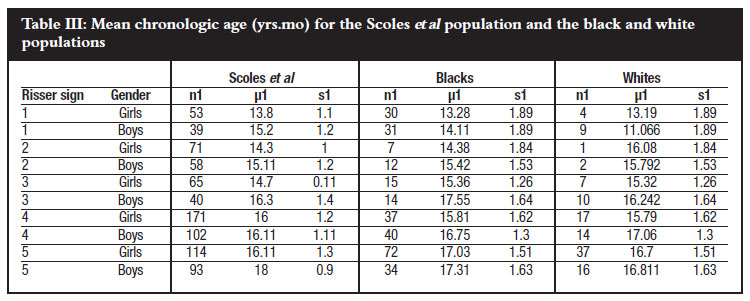
There was no significant statistical difference between the black and the white population in all the Risser stages except in Risser stage 1 where the average age was younger in white boys (Table II). Comparing the black and white population of this study with the population group of Scoles, no significant statistical difference in the average ages of each Risser stage was found except in Risser stage 1 (Table III). Our study population at Risser stage 1 was of a younger age than that of the North American Scoles population (Figure 2). Our female populations compared the same as those of the Scoles population (Figure 3).

Discussion
The Risser sign was first described by JC Risser in a paper in 1957, which was entitled, 'The iliac apophysis: An invaluable sign in the management of scoliosis'.7 The drawback in its use is that the Risser sign typically occurs after the peak height velocity (PHV) in 85% of patients and is thought not to correlate well with skeletal age.5 It also correlates differently in boys and girls. Saunders found that girls at Risser stage 4 have little remaining growth, while boys have substantial growth and may continue to have substantial curve progression.5 Saunders et al showed that girls tend to have a substantial curve progression between Risser stages 4 and 5.6Kotwicki showed that the posterior part of the apophysis can be hidden behind the sacrum, which leads to errors in interpretation.8This tends to be worse on PA rather than AP radiographs. He showed improved accuracy in interpretation by using lateral radiographs, which could be analysed using lateral Risser modifiers. Despite these drawbacks, the Risser sign remains an invaluable sign, and is still widely used by spinal surgeons. The advantage for using the Risser sign is the fact that it is readily visible on the standard set of scoliosis radiographs. No additional Xrays films are required. The second advantage is that it can be allocated with ease with little inter-observer disagreement as was evident in our finding of only a 2.74% disagreement between the two observers. One of the reasons for the inter-observer differences in this study was the presence of bowel gas which sometimes obstructed the iliac apophysis in patients who had abdominal distension (Figure 4). This is unlikely to be found in scoliosis patients. The other reason for the disagreement was the presence of a skipped unossified area (Figure 5).


This phenomenon was also noted by Risser, as he found that, after the usual capping or the appearance of ossification anteriorly and laterally on the iliac crest, further development may occur posteriorly, leaving a space, or gap, to be filled in later.7
The black and white populations in South Africa had similar trends (Figures 2 and 3). The only group that differed was Risser stage 1 for white boys who were of a younger age than the black population in the same Risser stage (Table III). The similarity between the groups suggests that genetic factors do not play a major role in the Risser staging. Climatic conditions might be a more important influence on Risser staging. Scoles found environmental factors to have some significant role on the ages of Risser stages.12 Grivas et al showed that geographical latitudes had an influence with age at menarche.9
The onset iliac crest ossification in boys was statistically significantly earlier in this study compared to the population studied by Scoles et al (Figure 2). The average age of Risser 3 in black boys was higher than that of Risser 4 and 5 in the same population (Table II). The average age in Risser stage 4 in white boys was also found to be higher than Risser stage 5 (Table III).
This anomalous finding may be explained by the marked difference in the number of radiographs assessed in each of those Risser stages.
In this study there were fewer radiographs with Risser stages 2 and 3 in line with the Scoles et al population (Table II). This may indicate that ossification passes quickly through these stages. The average age for Risser stage 5 in boys was statistically significantly lower in this study compared to the population of Scoles indicating that they stop growing earlier. The average age for girls Risser 5 was however higher than that of Scoles, indicating a more prolonged course.
Limitation of the study
The power of this study was limited by:
• the number of radiographs available in the radiology department for analysis. This resulted in smaller number of radiographs in certain groups.
• the fact that lateral pelvis radiographs were not available to confirm that the Risser 3 groups were not Risser 4.
• the fact that the individuals did not have serial radiographs, to allow charting of the exact time for each stage.
Conclusions
The Risser sign can be applied equally among the South African population as no significant statistical differences between the major population groups were found in this study.
Acknowledgements
The authors would like to acknowledge Dr N Aboo for assisting with the collection of the radiographs for this study.
References
1. Srokes IAF. Mechanical effect on skeletal growth. J Musculoskel Neuron Interact 2002; 2(3): 277-80. [ Links ]
2. Modi HN, Suh SW, Sang H-R, et al. Differential wedging of vertebral body and intervertebral disc in thoracic and lumbar spine in adolescent idiopathic scoliosis: A cross-sectional study in 150 patients. Scoliosis 2008; 3: 11 (www.scoliosisjournal.com/content/3/1/11). [ Links ]
3. Greulich WW, Pyle SI. Radiographic atlas of skeletal development of the hand and wrist, 2nd edition. Stanford CA, Stanford University Press 1959. [ Links ]
4. Tanner J, Oshman D, Bahhage F, Healy M. Tanner-Whitehouse bone age reference values for North American Children. J Paeditr 1997; 131: 34-40. [ Links ]
5. Sanders JO. Maturity indicators in spinal deformity. JBJS-A 2007; 89: 14-20. [ Links ]
6. Sanders JO, Khoury JG, Kishan S, Browne RH, Mooney JF III, Arnold KD, McConell SJ, Bauman JA, Finegold DN. Predicting scoliosis progression from skeletal maturity: A simplified classification during adolescence. JBJS-A 2008; 90: 540-53. [ Links ]
7. Risser JC. The iliac apophysis: an invaluable sign in the management of scoliosis. Clin. Orthop 1958; 11:111-19. [ Links ]
8. Kotwicki T. improved accuracy of Risser sign grading with lateral spinal radiography. Eur Spine J 2008; 17: 1676-85. [ Links ]
9. Grivas TB, Vasiliadis E, Mouzakis V, Mihas C, Koufopoulos G. Association between adolescent idiopathic scoliosis prevalence & age at menarche in different geographic latitudes. Scoliosis 2006; 1(9). [ Links ]
10. Ontell FK, Ivanovic M, Ablin DS, Barlow TW. Bone age in children of diverse ethnicity. AJR 1996; 167:1395-98. [ Links ]
11. Sun SS, Schubert CM, Chumlea WC, Roche AF, Kulin HE, Lee PA, Himes JH, Ryan AS. National estimates of the timing of sexual maturation & racial differences among US children, Pediatrics 2002; 110(5): 911-19. [ Links ]
12. Scoles PV, Salvagno R, Villalba K, Riew D. Relationship of iliac crest maturation to skeletal & chronologic age. J Paed Orth 1988; 8(6): 639-44. [ Links ]
 Reprint requests:
Reprint requests:
Dr Z Mayet
email: DR.Z@telkomsa.n
No benefits or sponsorship have been received by any of the authors for this study. This study was part of the University of Witwatersrand MMed Orthopaedic dissertation for one of the authors (ZM).


{kind=link}
{kind=link}