










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSA Orthopaedic Journal
versão On-line ISSN 2309-8309
versão impressa ISSN 1681-150X
SA orthop. j. vol.9 no.3 Centurion Jan. 2010
CASE REPORT
Contiguous bifacet cervical fracture dislocations
JWM KigeraI; M NyatiII
IMBChB. Registrar, Department of Orthopaedics, Makerere University, Kampala, Uganda
IIMMed. Consultant Orthopaedic Surgeon, Spine Unit, Department of Orthopaedics, Mulago Hospital, Kampala, Uganda
ABSTRACT
Bifacet dislocations of the cervical spine are severe debilitating injuries often associated with complete cord injury. Contiguous bilateral facet dislocations are extremely rare and, to the best of our knowledge, have only been described once before. We present a patient who was involved in a road traffic accident. Pre-operative radiographs suggested contiguous bifacet injury and this was confirmed intra-operatively. This should alert physicians to the possibility of contiguous injuries to the cervical spine.
Introduction
Bifacet dislocation of the cervical spine is associated with a complete cord injury in up to 85% of injuries with the majority of the other patients suffering some form of neurological compromise.1 During dislocation, the inferior articular facets of the upper vertebra separate and displace anteriorly while rotating primarily in flexion, relative to the superior facets of the lower vertebra and become locked in the intervertebral foramina. At the time of the dislocation, dynamic spinal-canal narrowing occurs, producing cord compression and complete or incomplete cord lesions.2 At the dislocated spinal level, the spinal cord is dynamically compressed between the anterior edge of the neural arch of the upper vertebra and the posterosuperior corner of the lower vertebral body.3 These injuries are hence quite debilitating. We describe a contiguous bifacet dislocation of the C4/5 and C5/6 regions. This is rare and, to our knowledge, has only been described once before.
Case report
A 23-year-old man was admitted to the emergency ward after being involved in a road traffic crash. He was a motorcycle (bodaboda) rider who fell off his motorcycle after being knocked from behind by a speeding motor vehicle. He immediately had neck pain and an inability to move all four limbs. Initial assessment on admission to the Accident and Emergency Ward revealed a Glasgow Coma Scale of 15, and quadriplegia with a sensory level of T4. The patient was transferred to the spine unit after resuscitation and initial imaging of the spine.
Radiology
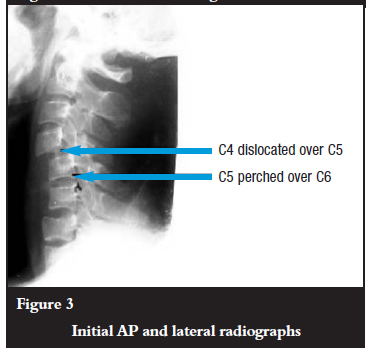
Antero-posterior and lateral views of the cervical spine revealed bifacet dislocation at the C4/5 level and at the C5/6 level. The injury at the C5/C6 level is less obvious and is evidenced by the disruption of the spinal laminar line and the rotation of the spinous process as seen on the AP film. There is an apparent retrolisthesis at C6/7 level. The posterior bodylines are, however, intact and the superior endplate of C7 is co-linear with the inferior end plate of C6. It is likely that there is a fracture of the superior endplate of C6. CT scans would have helped to evaluate the pathology better. No CT scans were done due to financial constraints.
Initial AP and lateral radiographs of the patient are shown in Figures 1, 2 and 3.


Intervention and outcome
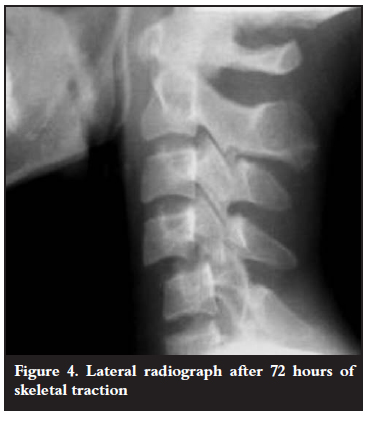
Closed reduction using Gardner Well tongs was considered but this was not done using the standard protocol due to lack of fluoroscopic control. Check radiographs taken after 72 hours of traction revealed no reduction.
Figure 4 shows the lateral radiograph after 72 hours of traction.
Subsequently the surgeons decided on operative reduction. Intra-operative findings included bifacet dislocations at the C4/5 and C5/6 levels and lamina fractures of C4 and C5. There was a lateral mass fracture of C4 (Figure 5).
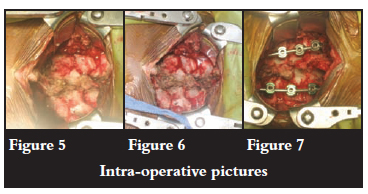
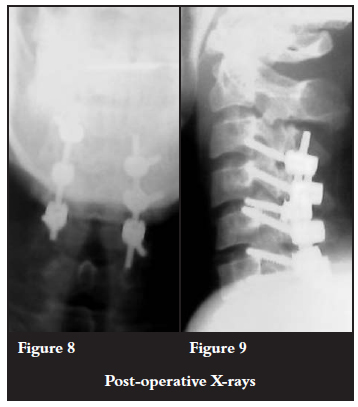
Posterior reduction was done plus instrumentation using lateral mass screws and rods from C3 to C6. The extension of the instrumentation and fusion to the C3 level was necessitated by the fracture of the lateral mass of C4 (Figures 6 and 7). Postoperative control radiographs were taken and showed adequate reduction (Figures 8 and 9).
No neurological improvement was noted at the last review eight weeks postoperatively. The patient is being rehabilitated into a wheelchair.
Discussion
Bifacet dislocations constitute about 37% of all subaxial injuries of the spine.3 They have been noted to have devastating consequences. The mechanism of injury is described as flexion-distraction. The injury is commonest at the C5/6 segment.2 The posterior ligamentous structures are usually disrupted as well as the anterior structures of the annulus fibrosus and the anterior longitudinal ligament.4 It has been noted that the radiologically determined extent of canal compromise is only a fraction of the initial dynamic canal narrowing.2
A review of the literature has revealed only one case of contiguous bifacet dislocation of the cervical spine.5 It is plausible that contiguous injuries in the lower cervical spine can occur and clinicians should be aware of this. Vigilance and careful review of radiographs is one way to make sure injuries of such magnitude are not missed in the clinical setting. CT scans would be of added value in defining the exact nature of these injuries.
Conclusion
Contiguous bifacet dislocations of the cervical spine are rare clinical entities. This case highlights the need for thorough radiological evaluation of all patients suffering from cervical spine injuries. A prospective study is needed to further evaluate the magnitude of these injuries.
References
1. O'Brien PJ, Schweigel JF, Thompson WJ. Dislocations of the lower cervical spine. J Trauma 1982;22:710-4. [ Links ]
2. Ivancic PC, Pearson AM, Tominaga Y. Mechanism of cervical spinal cord injury during bilateral facet dislocation. Spine 2007;32(22):2467-73. [ Links ]
3. Allen BL, Ferguson RL, Lehmann TR, O'Brien RP. A mechanistic classification of closed, indirect fractures and dislocations of the lower cervical spine. Spine 1982;7:1-27. [ Links ]
4. Vaccaro AR, Madigan L, Schweitzer ME, Flanders AF, Hilibrand AS, Albert TJ. Magnetic resonance imaging analysis of soft tissue disruption after flexion-distraction injuries of the subaxial cervical spine. Spine 2001;26(17):1866-72. [ Links ]
5. Uzel AP, Do L. Multilevel contiguous injuries of the lower cervical spine during flexion trauma with delayed diagnosis: a case report. Neurochirurgie 2009;55(6): 585-8. Epub 2009 May 28. [ Links ]
 Reprint requests:
Reprint requests:
Dr JWM Kigera
E-mail: jameskigera@yahoo.co.uk
No benefits of any form have been received from a commercial party related directly or indirectly to the subject of this article.

