










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSA Orthopaedic Journal
On-line version ISSN 2309-8309
Print version ISSN 1681-150X
SA orthop. j. vol.9 n.1 Centurion Jan. 2010
CLINICAL ARTICLE
Cervical corpectomy and anterior standalone plate stabilisation in sub-axial cervical spine trauma: a retrospective review of the radiological outcomes
DT McGuireI; N KrugerII
IMBChB, Registrar, Department of Orthopaedics, Groote Schuur Hospital, University of Cape Town
IIMBChB, FRCS(Ed), FCS(SA)Orth, Consultant Spine and Orthopaedic Surgeon, Department of Orthopaedics, Groote Schuur Hospital, University of Cape Town
ABSTRACT
INTRODUCTION: Compression-flexion injuries of the cervical spine often result in instability of both the anterior and posterior columns. Debate exists in the literature regarding the surgical approach to stabilisation of these fractures, the options being anterior, posterior or combined surgical approaches. The combined approach offers superior stability, but results in increased cost, patient morbidity and theatre time. This study reviews the results of the anterior approach with standalone cervical corpectomy and plate stabilisation combined with postoperative Philadelphia collar immobilisation.
METHODS: We retrospectively reviewed 30 patients with compression-flexion injuries of the cervical spine. Surgical management consisted of anterior corpectomy, iliac tricortical strut autograft, and anterior cervical static locked plating. Postoperatively patients were immobilised in a Philadelphia collar for six weeks. This radiological review assessed the postoperative constructs, and the final follow-up radiographs.
RESULTS: Overall radiological union was achieved in 90% of cases at an average of 3.8 months. Patients with good constructs had a union rate of 100%. Those with poor constructs had a 25% union rate. Poor results included delayed union, cervical kyphosis, graft migration and loss of screw fixation.
CONCLUSION: Poor results in this study were related to operative technique. With good operative technique, excellent results can be expected. Therefore, anterior cervical corpectomy and locked plating alone, with Philadelphia collar immobilisation, appears to be a safe and cost-effective alternative in the management of these fractures.
Introduction
Fractures of the sub-axial cervical spine can be devastating injuries associated with a high rate of injury to the spinal cord.1 These fractures are caused by various mechanisms of action. In 1982 a mechanistic classification was introduced by Allen and Ferguson, which divided subaxial fractures into six types, which were further divided into stages.2
Compression-flexion injuries are most commonly caused by motor vehicle accidents and diving injuries.3 They are divided into five stages with increasing severity for each stage. The injury is speculated to occur first by flexion of the spine through the facet joints. The anterior column (vertebral body) becomes increasingly compressed and shortened. Eventually, the posterior ligamentous complex fails, noted by interspinous gapping and local kyphosis. With further energy, the facet joints will fail, leading to translational deformity.4 Therefore with mild injuries only the anterior column is injured, but with more severe injuries the posterior column is disrupted as well.
There is debate in the literature regarding the approach to stabilisation of these fractures, particularly with regard to injuries with disruption of both the anterior and posterior columns.5 The different approaches that can be used are anterior, posterior, or combined approaches. Halo vests have also been advocated for treatment of these fractures.6
Brodke et al believe that a fracture involving both columns is an indication to do a combined approach using both anterior and posterior instrumentation.7 This addresses the biomechanical deficiencies in both columns as well as allowing for anterior decompression. If an anterior or posterior alone fixation is performed, the biomechanical deficiencies are not addressed as only one column is stabilised.8
A combined surgical approach does have its shortcomings however, such as:
• increased surgical time
• increased cost
• the need for the patient to be turned on the operating table
• increased patient morbidity
• increased anaesthetic time and complications
• increased blood loss9,10
The advent of locked plate technology has increased the strength and stability of plate osteosynthesis.11 This now lends itself to the possibility of anterior alone plate fixation with postoperative immobilisation in a cervical orthosis.12 The rationale behind this is that locked plate fixation of the anterior column is sufficient enough to avoid having to augment the posterior column surgically, and simple immobilisation in a Philadelphia collar is adequate.
This study was performed to assess the results of this technique as it is an attractive option, especially in units with limited theatre time and budget constraints.
Materials and methods
This was a retrospective radiological review. We reviewed 30 patients with compression-flexion injuries of the subaxial cervical spine who presented to Groote Schuur hospital over a five-year period. There were 24 males and six females in the study group with an average age of 26 years.
All patients presented initially to Groote Schuur hospital's trauma unit, either from referral hospitals or from Groote Schuur's drainage area. There they were stabilised and initially immobilised with cones callipers and traction. All patients had cervical spine X-rays and an MRI scan.
Patients were operated on at the next available theatre list. The surgical procedure was an anterior corpectomy, decompression and fusion via a Smith-Robinson anterior approach. The plate used was a CSLP (cervical spine locking plate) - all cases done used a plate from the same company. The graft was an iliac crest tricortical strut autograft, harvested with osteotomes or an oscillating saw. A screw was inserted in the graft depending on the surgeon's preference. Patients were immobilised in a Philadelphia collar for 6 weeks postoperatively. A variety of surgeons were involved including consultant orthopaedic and neurosurgeons, as well as spinal fellows.
The following parameters were assessed:
Pre-op:
• age
• sex
• injury severity using the Allen-Ferguson classification
• neurological injury and level
• posterior structure integrity on MRI scan
Postop:
• hardware characteristics
• graft characteristics
• sagittal alignment
• surgical technique
Final radiological review (minimum 3 months)
• hardware characteristics
• graft characteristics
• sagittal alignment
• union
We defined the surgical technique as either adequate or sub-optimal fixation.
Adequate fixation:
• unicortical screws recessed into the plate and sited in bone
• no plate encroachment over adjacent disc spaces
• plate well applied to the vertebral body
• fixed in lordosis
Sub-optimal fixation:
• poor plate and/or screw position>
• screws too short or misplaced
• fixed in kyphosis
• poor graft position
The graft was assessed for:
• gap
• poor position
• height
Results
A total of 30 patients were enrolled in the study. When the pre-op parameters were correlated we found the following:
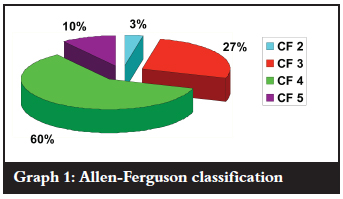
| 1. | Severity of injury by Allen-Ferguson classification (Graph 1): |
| • CF 1: 0 patients (0%) | |
| • CF 2: 1 patients (3%) | |
| • CF 3: 8 patients (27%) | |
| • CF 4: 18 patients (60%) | |
| • CF 5: 3 patients (10%) |
| 2. | Spinal cord injury: |
| • Neurologically normal: 1 patient (3%) | |
| • Incomplete neurological deficit: 14 patients (47%) | |
| • Complete neurological deficit: 15 patients (50%) |
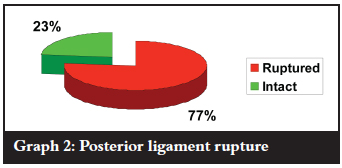
| 3. | Posterior ligamentous disruption assessed by MRI scan (Graph 2): |
| • Intact: 7 patients (23%) | |
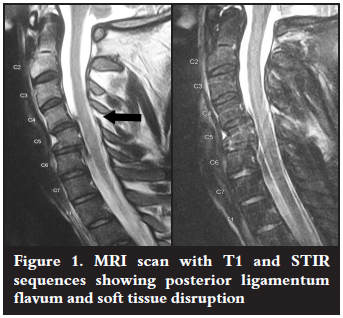
| • Ruptured: 23 patients (77%) (Figure 1) |
On the initial post-op radiographs the quality of the construct was assessed by the abovementioned means, and was classified as either adequate or sub-optimal.
• Adequate: 26 patients (87%)
• Sub-optimal: 4 patients (13%)
The postop and final follow-up radiographs were then assessed and compared.
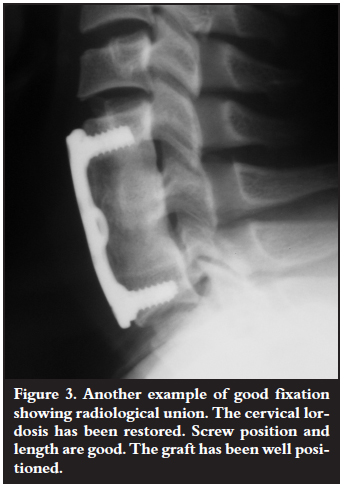
| 4. | Union rate: |
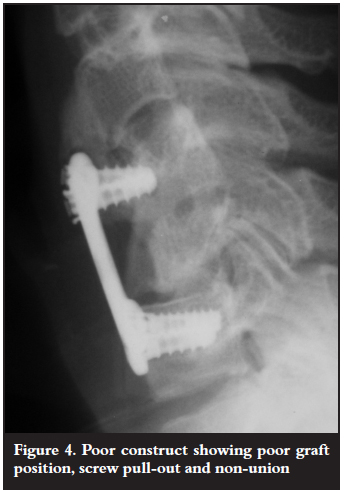
| • Overall union rate was 90% (27 out of 30 patients) (Figures 2 and 3) | |
| • Only 10% (3 patients) did not unite (Figure 4) |

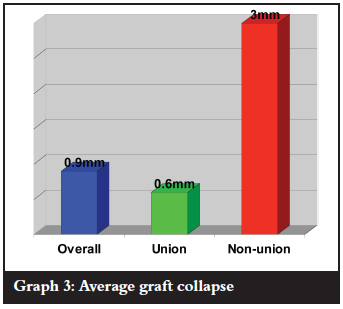
| 5. | Average graft collapse (Graph 3): |
| • Overall: 0.9 mm | |
| • Non-union: 3 mm | |
| • Union: 0.6 mm |
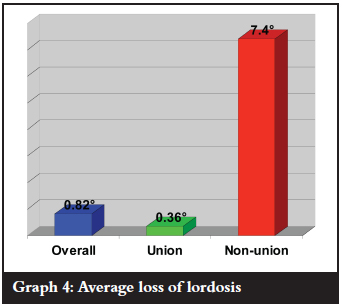
| 6. | Average loss of lordosis (Graph 4): |
| • Overall: 0.82º | |
| • Non-union: 7.4º | |
| • Union: 0.36º |
We then assessed the union rates compared with the various measured parameters:
| 1. | Severity of injury (Allen-Ferguson classification): | |
| • CF 2: | Union - 2 patients | |
| Non-union - 0 patients | ||
| • CF 3: | Union - 7 patients | |
| Non-union - 1 patient | ||
| • CF 4: | Union - 15 patients | |
| Non-union - 2 patients | ||
| • CF 5: | Union - 3 patients | |
| Non-union - 0 patients | ||
This suggests that injury severity by Allen-Ferguson classification does not affect union rates.
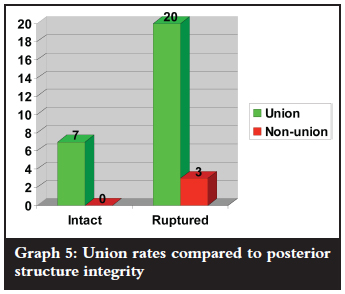
| 2. | Posterior ligament disruption - 24 patients (Graph 5): |
| • Union: 20 patients (87%) | |
| • Non-union: 3 patients (13%) | |
| These union rates are similar to the overall union rate. |
| 3. | Sub-optimal fixation (4 patients): |
| Union: 1 patient (25%) | |
| Non-union: 3 patients (75%) |
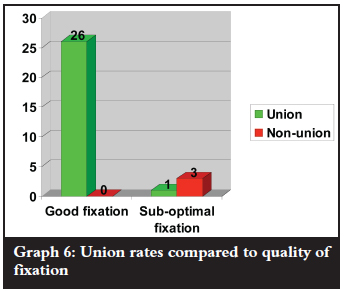
| 4. | Adequate fixation - 26 patients (Graph 6): |
| Union: 26 patients - 100% union rate | |
| Non-union: 0 patients |
Discussion
The principal goals in the surgical treatment of cervical spine injuries are: stabilisation of the spine, decompression of the spinal cord and facilitation of rehabilitation.15 With compression-flexion injuries of the sub-axial cervical spine, decompression should be performed anteriorly via a corpectomy to increase the chance of neurological recovery.16 Stabilisation is obtained by fusion to adjacent vertebrae, and can be done via either an anterior or posterior approach.
Since the introduction of anterior plate fixation by Orozco and Llovet-Tapies,17 Bohler and Tscherne et al. excellent clinical results have been reported in the literature.18,19 Since then this technique has gained in popularity.20
Originally non-locked plates were used, with either static or dynamic screw fixation. Since then the locked plate system has been introduced. In recent years, anterior plating with locked fixation screws has been shown to provide better stability than conventional anterior plating without locked screw fixation.21 Fogel et al, also showed that locking plate constructs had higher pull-out strengths than nonlocked systems.22
Compression-flexion injuries of the cervical spine causing spinal cord injury are usually associated with disruption of the posterior bony and/or ligamentous structures. This is supported by the findings of this study. This therefore raises the question of whether anterior plate stabilisation alone is biomechanically stable enough to treat these fractures.
Several investigators have conducted biomechanical studies of the surgical construct stability provided by various anterior and posterior instrumentations of the cervical spine.21,23-25 Broadly speaking the options are anterior alone, posterior alone, or a combined stabilisation approach. It has been concluded by many of these studies that combined anterior and posterior fixation, and a posterior alone fixation, are both biomechanically more stable than an anterior alone fixation.23,26,27 Although posterior stabilisation alone provides adequate stability, there is inadequate decompression anteriorly via a corpectomy, especially when there is canal compromise, so this technique is not favoured by surgeons.16 Therefore this leaves two options: anterior alone stabilisation or a combined approach.
Some studies have suggested that anterior plate fixation alone was insufficient when posterior structures were injured.24,25 There have been no studies though, to assess the success of the technique of anterior alone locked plate stabilisation after single level corpectomy, with postoperative immobilisation in a rigid cervical collar. The theory behind this is that the increased stability afforded by locked plates, combined with immobilisation in a rigid cervical collar, obviates the need for posterior stabilisation.
As mentioned in the introduction, a combined anterior and posterior approach is associated with increased complications and prolonged operative time. If an anterior alone approach shows acceptable results then it would be an attractive option due to the shorter theatre time required, reduced cost and patient morbidity.
There is a paucity of literature showing results using this technique. Adams et al performed in vitro testing simulating burst fractures with posterior distraction of the subaxial cervical spine. They then stabilised this with an anterior locked plate with graft, and showed that this technique is capable of returning the stability of this cadaveric spine to well within its pre-injury level.28 Grubb et al also investigated this using an injury model with anterior and posterior disruption. They demonstrated that the stability of the normal spine was comparable to that of an injured spine stabilised by an anterior locking plate with unicortical screws, or by a non-locking plate with bicortical screws.21
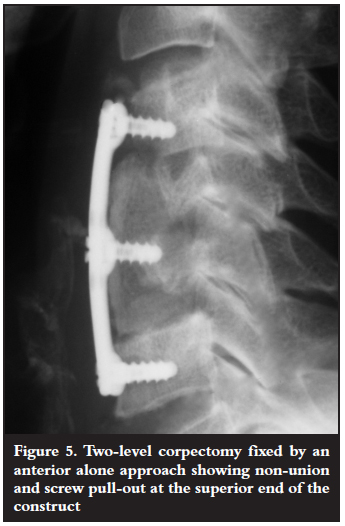
If there is more than one vertebral body involved and the procedure requires a two-level corpectomy, results are not as encouraging. There are reports in the literature that show a high rate of failure with anterior instrumentation alone in these cases.29 In our study, out of the three patients who did not unite, one of them was a two-level corpectomy (Figure 5). In these cases then it is probably advisable to supplement the anterior fixation with posterior instrumentation as well.
Patients in this study were only followed up until radiological union. Therefore the follow-up is too short to comment on any adjacent level degeneration.
Conclusion
All poor results in this study were due to sub-optimal fixation. Those constructs showed a 25% union rate (1 out of 4).
All patients who had adequate fixation united (26 out of 26). Therefore with good surgical technique 100% union can be expected.
There was no correlation between posterior ligament rupture and union rates. Therefore, it appears that supplementing the anterior fixation with posterior instrumentation is unnecessary. In cases where multi-level corpectomy is required, posterior supplementary fixation is recommended.
We can therefore conclude that anterior cervical corpectomy and locked plating alone with Philadelphia collar immobilisation appears to be a safe, cost-effective and time-saving alternative in the management of compression-flexion fractures in the sub-axial cervical spine.
References
1. Kraus JF, Franti CE, Riggins RS, et al. Incidence of traumaticspinal cord lesions. and dislocations of the lower cervical spine. Spine 1982;7:1-22. [ Links ]
2. Reference 2 missing?
3. Goldberg W, Mueller C, Panacek E, et al. Distribution and patterns of blunt traumatic cervical spine injury. Ann Emerg Med 2001;38:17-21 [ Links ]
4. Bono CM. Fractures and dislocations of the lower cervical spine. In: Bucholz R, Heckman JD, Court-Brown CM (eds). Rockwood & Green's Fractures In Adults, 6th Edition. Lippincott,Williams and Wilkins 2006:1498-541. [ Links ]
5. Garvey TA, Eismont FJ, Roberti LJ. Anterior decompression, structural bone grafting, and Caspar plate stabilization for unstable cervical spine fractures and/or dislocations. Spine 1992;17:431-35. [ Links ]
6. Fisher CG, Dvorak MF, Leith J, et al. Comparison of outcomes for unstable lower cervical flexion teardrop fractures managed with halo thoracic vest versus anterior corpectomy and plating. Spine 2002;27:160-66. [ Links ]
7. Brodke DS, Anderson PA, Newell DW, et al. Comparison of anterior and posterior approaches in cervical spinal cord injuries. J Spinal Disord Tech 2003;16:229-35. [ Links ]
8. Mihara H, Cheng BC, David SM, et al. Biomechanical comparison of posterior cervical fixation. Spine 2001;26:1662-67. [ Links ]
9. Roy-Camille R, Saillant G, Laville C, et al. Treatment of lower cervical spinal injuries: C3 to C7. Spine 1992;17:442-46. [ Links ]
10. Bohler J, Gaudernak T. Anterior plate stabilization for fracturedislocations of the lower cervical spine. J Trauma 1980;20:203-5. [ Links ]
11. Smith W, Ziran B, Anglen J. Locking plates: Tips and tricks. J Bone Joint Surg Am. 2007;10:2297-307. [ Links ]
12. Fogel G, Liu W, Reitman C. Cervical plates: Comparison of physical characteristics and in vitro pull out strength. The Spine Journal 2003;3:118-24. [ Links ]
13. Orozco DR, Llovet-Tapies. J Osteosintesis en las fractures de raquis cervical. Rev Orthop Traumatol 1970;14:285-88. [ Links ]
14. Aebi M, Zuber K, Marchesi D. Treatment of cervical spine injuries with anterior plating. Indications, techniques, and results. Spine 1991;16:38-45. [ Links ]
15. Kocis J,Wendsche P,Vesely R, et al. Complications during and after surgery of the lower cervical spine by isolated anterior approach with CSLP implant. Acta Neurochir (wien) 2008;150:1067-71. [ Links ]
16. Toh E, Nomura T,Watanabe M, Mochida J. Surgical treatment for injuries of the middle and lower cervical spine.International Orthopaedics 2006;30:54-58. [ Links ]
17. Orozco DR, Llovet-Tapies J. Osteosintesis en las fractures de raquis cervical. Rev Orthop Traumatol 1970;14:285-88. [ Links ]
18. Aebi M, Zuber K, Marchesi D. Treatment of cervical spine injuries with anterior plating. Indications, techniques, and results. Spine 1991;16:38-45. [ Links ]
19. Blauth M, Schmidt U, Dienst M, Knop C, Lobenhoffer P, Tscherne H. Long-term outcome of 57 patients after ventral interbody spondylodesis of the lower cervical spine. Unfallchirurg 1997;99:925-39. [ Links ]
20. de Oliveira JC. Anterior plate fixation of traumatic lesions of the lower cervical spine. Spine 1987;12:324-29. [ Links ]
21. Grubb MR, Currier BL, Shih JS, Bonin V, Grabowski JJ, Chao EY. Biomechanical evaluation of anterior cervical spine stabilization. Spine 1998;23:886-92. [ Links ]
22. Fogel G, Liu W, Reitman C, S Essess. Cervical plates: comparison of physical characteristics and in vitro pushout strength. The Spine Journal 2003;3:118-24. [ Links ]
23. Young Do K, Tae-Hong L, Jae Won Y. A Biomechanical Comparison of Modern Anterior and Posterior Plate Fixation of the Cervical Spine. Spine 2001;26:15-21. [ Links ]
24. Coe JD, Warden KE, Sutterlin CE III, McAfee PC. Biomechanical evaluation of cervical spinal stabilization methods in a human cadaveric model. Spine 1989;14:1122-31. [ Links ]
25. Sutterlin CE III, McAfee PC, Warden KE, Rey RM Jr, Farey ID. A biomechanical evaluation of cervical spinal stabilization methods in a bovine model. Static and cyclical loading. Spine 1989;13:795-802. [ Links ]
26. Grubb MR, Currier BL, Stone J, Warden KE, An KN. Biomechanical evaluation of posterior cervical stabilization after a wide laminectomy. Spine 1997;22:1948-54. [ Links ]
27. Richman JD, Daniel TE, Anderson DD, Miller PL, Douglas RA. Biomechanical evaluation of cervical spine stabilization methods using a porcine model. Spine 1997;20:2192-97. [ Links ]
28. Adams M, Crawford N, Chamberlain R, et al. Biomechanical comparison of anterior cervical plating and combined anterior/lateral mass plating. The Spine Journal 2001;1:166-70. [ Links ]
29. Swank ML, Sutterlin CE 3rd, Bossons CR, et al. Rigid internal fixation with lateral mass plates in multilevel anterior and posterior reconstruction of the cervical spine. Spine 1997;22(3):274-82. [ Links ]
 Reprint requests:
Reprint requests:
Dr DT McGuire
Department of Orthopaedics Groote Schuur Hospital
H49 OMB Observatory
Tel: (021) 404-5108 Fax: (021) 404-3260
Email: duncan.mcguire@gmail.com
No benefits of any form have been received from a commercial party related directly or indirectly to the subject of this article. The work in this article has been approved by an ethics committee.

