










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouthern African Journal of Critical Care (Online)
versión On-line ISSN 2078-676X
versión impresa ISSN 1562-8264
South. Afr. j. crit. care (Online) vol.39 no.3 Pretoria nov. 2023
http://dx.doi.org/10.7196/SAJCC.2023.v39i3.1261
RESEARCH
Core competencies in critical care for general medical practitioners in South Africa: A Delphi study
S D MaasdorpI; F ParukII; K de VasconcellosIII; C GrionIV; I JoubertV; G M JoyntVI; N KalafatisVII; S E LapinskyVIII; J LipmanIX; M L N G MalbrainX; B MraraXI; G A RichardsXII; M G L SpruytXIII; E van der MerweXIV; J L VincentXV; L J van der MerweXVI
IMB ChB, MMed (Int Med), FCP (SA), Cert Pulmonology (SA) Phys; Division of Pulmonology and Critical Care, Department of Internal Medicine, Faculty of Health Sciences, University of the Free State, Bloemfontein, South Africa
IIMB ChB, FCOG (SA), Cert Crit Care (SA), MD; Department of Critical Care, Faculty of Health Sciences, University of Pretoria, South Africa
IIIFCA (SA), Cert Crit Care (SA); Discipline of Anaesthesiology and Critical Care, School of Clinical Medicine, College of Health Sciences, University of KwaZulu-Natal, Durban, South Africa
IVMD, PhD; Department of Clinical Medical, Hospital Universitári, Universidade Estadual de Londrina, Brazil
VMB BCh, DA (SA), FCA (SA), Critical Care; Division of Critical Care, Department of Anaesthesia and Perioperative Medicine, Faculty of Health Sciences, University of Cape Town, South Africa
VIMB BCh, FFA (SA), FCICM, FRCP (Edin); Department of Anaesthesia and Intensive Care, The Chinese University of Hong Kong, China
VIIMB BCh, FCA (SA), Cert Crit Care (SA), PhD; Discipline of Anaesthesiology and Critical Care, School of Clinical Medicine, College of Health Sciences, University of KwaZulu-Natal, Durban, South Africa
VIIIMB BCh, MSc, FRCPC; Department of Critical Care, Faculty of Medicine, University of Toronto, Canada
IXMB BCh, DA (SA), FFA (SA), FFA (Crit Care) (SA), FCICM, MD (Res), FISAC, DMed (Res); Jamieson Trauma Institute, Royal Brisbane and Women's Hospital, University of Queensland, Brisbane, Australia; and Nimes University Hospital, University of Montpellier, Nimes, France
XMD, PhD; First Department of Anaesthesiology and Intensive Therapy, Faculty of Medicine, Medical University of Lublin, Poland
XIMB BCh, DA (SA), FCA (SA), Cert Crit Care (SA); Department of Anaesthesia, Faculty of Health Sciences, Walter Sisulu University, Mthatha, South Africa
XIIFCP (SA), PhD, FRCP; Department of Critical Care, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
XIIIMB ChB, MMed (Surg), Critical Care; Division of Critical Care, Department of Surgery, University of the Free State, Bloemfontein, South Africa
XIVFRCP (London), MMed (Int Med), Cert Crit Care (SA) Phys; Department of Critical Care, Livingstone Hospital, Gqeberha, South Africa
XVMD, PhD; Department of Intensive Care, Erasme University Hospital, Université Libre de Bruxelles, Belgium
XVIMB ChB, MMedSc (Surg), DA (SA), PhD (HPE); Division of Health Sciences Education, Faculty of Health Sciences, University of the Free State, Bloemfontein, South Africa
ABSTRACT
BACKGROUND. Despite a high burden of disease that requires critical care services, there are a limited number of intensivists in South Africa (SA). Medical practitioners at district and regional public sector hospitals frequently manage critically ill patients in the absence of intensivists, despite these medical practitioners having had minimal exposure to critical care during their undergraduate training.
OBJECTIVES. To identify core competencies in critical care for medical practitioners who provide critical care services at public sector hospitals in SA where intensivists are not available to direct patient management.
METHODS. A preliminary list of core competencies in critical care was compiled. Thereafter, 13 national and international experts were requested to achieve consensus on a final list of core competencies that are required for critical care by medical practitioners, using a modified Delphi process.
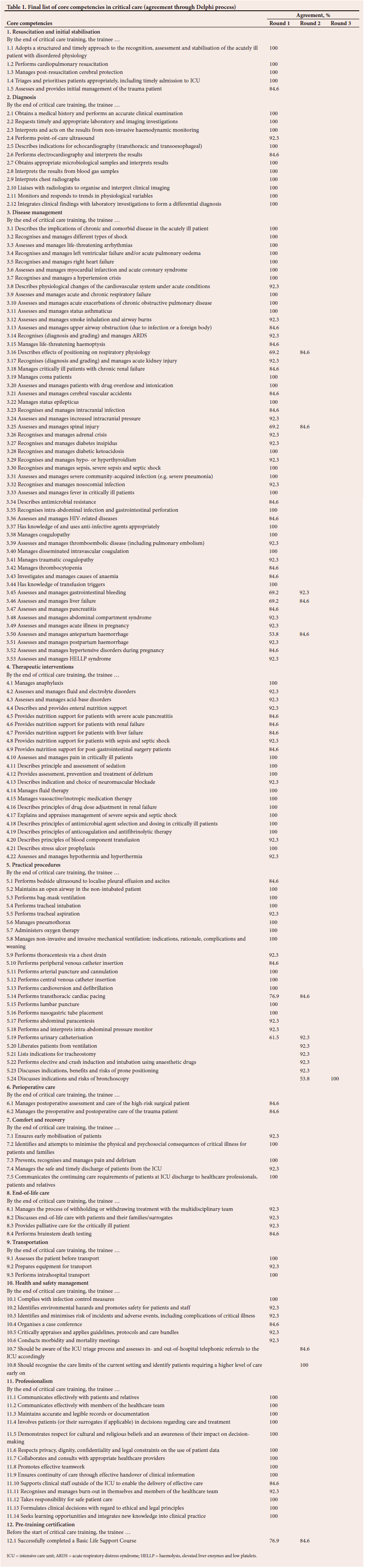
RESULTS. A final list of 153 core competencies in critical care was identified.
CONCLUSION. The core competencies identified by this study could assist in developing training programmes for medical practitioners to improve the quality of critical care services provided at district and regional hospitals in SA.
Keywords Core competencies, medical practitioners, Delphi.
South Africa (SA) is plagued by a high burden of HIV/AIDS, tuberculosis, non-communicable diseases, maternal conditions and trauma that often requires immediate critical care.[1] Specialists other than intensivists, as well as medical practitioners with varying levels of expertise and experience, are predominantly involved in the care of these critically ill patients, especially in non-university-affiliated hospitals.[2] This situation is largely attributed to a paucity of registered intensivists in SA.
The SA population comprises ~60 million people[3] and it is estimated that between 50 and 75 registered intensive care specialists (intensivists) work in intensive care units (ICUs) in the country.[4] Most healthcare workers practise in urban areas, with very few practising in rural areas, where the majority of the population resides.[5] Every year, only a small number of intensivists complete their training and qualify, and the lack of dedicated subspecialist training posts in SA contributes substantially to the limited number of registered intensivists. Therefore, it is unlikely that there will be sufficient intensivists to provide critical care services in SA within the foreseeable future.[2]
Despite this shortage, there is little exposure to critical care at undergraduate medical education level. Critical care specialisation requires specialty training, and there are, furthermore, no postgraduate diploma courses to bridge the gap in competency between undergraduate and ICU specialist levels. Several short courses in critical care for non-specialist healthcare professionals have been designed. Joynt et al.[6]conducted a systematic review of eight short courses for teaching critical care skills to non-specialist doctors working in ICUs. They found that the courses varied regarding content and that only the Basic Assessment and Support in Intensive Care (BASIC) and Fundamental Critical Care Support (FCCS) courses (both available in SA) included curriculum content that was similar to the guidelines prescribed by the Society of Critical Care Medicine and the Australia and New Zealand College of Anaesthetists for residents in training.[6] BASIC is a 2-day course that focuses on essential aspects of intensive care[7] and is designed for doctors who are new to the ICU environment. The 2-day FCCS course aims to train non-intensivists to manage critically ill patients for the first 24 hours, or until a critical care consultation can be undertaken.[8] None of the courses, however, includes experiential learning or assesses whether specific competencies have been achieved.[6]
Graduates of undergraduate medical programmes in SA work either as general practitioners (private practice) or medical officers (public health service). These general practitioners and medical officers are frequently expected to provide first-line healthcare services to critically ill patients, despite critical care not being specified as an essential requirement for national undergraduate medical training in SA.[9] Exposure and training in critical care can, however, increase the knowledge, skills and confidence of doctors.[10] An additional benefit is reported by Haniffa et al.,[11] who found that, if doctors and nurses working in resource-limited settings received dedicated training, ICU mortality rates declined from 41% to 18%. Training of primary care physicians will have an impact on the burden and outcomes of patients who are admitted to ICUs in SA. Many of these admissions are unplanned.[12] Adequate 'high care dependency units' for postoperative care of elective surgical patients have the potential to decrease the burden on critical care resources in SA by 23%. Singh et al.[13] found that, in KwaZulu-Natal Province, patients who were referred to the ICU were young and had a high burden of medical and trauma conditions. Similar findings were reported from the Eastern Cape Province.[14] Decisions to accept patients to ICU were limited by available resources, and there was a need to apply ICU triage.[13]
We sought to address the problem of a lack of critical care training for general practitioners and medical officers in SA. Specifically, the findings reported in this article identify the core competencies in critical care that could be reasonably expected of medical practitioners working in critical care settings or providing critical care services at public sector hospitals in SA in the absence of intensivist supervision.
Methods
The study used a modified Delphi process. Researchers of the Rand Corporation first developed the Delphi process as 'a method of eliciting and refining group judgements'.[15] Members of the study group answered several rounds of questionnaires anonymously, until final consensus was reached. In the modified Delphi process used for this study, curricula of international critical care training programmes, including CoBaTrICE[16] and the Chinese Critical Care Society,[17] were reviewed to identify competencies deemed essential to critical care training programmes. The core competencies compiled by the Chinese Critical Care Society were deemed suitable for low- and middle-income countries,[17] and were, therefore, used to compile the questionnaire. The questionnaire made use of a 5-point Likert scale and options for answers were 'strongly disagree', 'disagree', 'neutral', 'agree' and 'strongly agree'. A pilot study was conducted first, by submitting the questionnaire to two physicians working in the Department of Critical Care at the University of the Free State, Bloemfontein, SA, to determine aspects such as clarity of the questions, time required to complete the questionnaire, and to ensure that the questions were not biased. No changes were made to the questionnaire after the pilot study. As the participants in the pilot study did not meet inclusion criteria (as discussed below) for the study, the results of the pilot study were not included in this analysis.
National and international experts in critical care were identified and invited to participate in the modified Delphi process. The academic heads of critical care units at nine medical schools in SA were deemed to be national experts in their field and were approached to participate, or to suggest an alternative participant with at least 5 years' experience in critical care medicine for inclusion on the Delphi panel. International experts in critical care medicine were also identified by perusing the council membership of international societies of intensive care medicine or critical care medicine.
The invitation to participate was sent via email to all identified experts. Consent to participate in the study was inferred by participation. A link to an electronic questionnaire using REDCap (Research Electronic Data Capture),[18,19] was sent via email to all experts who accepted the invitation and who, thus, became Delphi panel members. Consensus was defined as agreement of >80% for individual questions on the questionnaire. Several rounds of the Delphi process were performed until agreement of >80% was achieved. Answers of agree or strongly agree were deemed to be agreement, and questions on which >80% agreement was achieved during the first round were removed from subsequent rounds. This process was repeated until consensus was reached for all questions. Additional competencies suggested by Delphi panel members were included in the subsequent rounds. Descriptive statistics, i.e. frequencies and percentages, were calculated for the categorical data, and the analysis was performed by the Department of Biostatistics, University of the Free State. Data analysis was performed with SAS Software, version 9.4 (SAS Institute Inc., USA).
Ethical clearance to conduct the study was obtained from the Health Sciences Research Ethics Committee of the University of the Free State (ref. no. UFS-HSD2020/1524/2411).
Results
A total of 25 experts were invited (11 national and 14 international). Of these, 13 (52%) (7 national and 6 international) accepted the invitation and completed the first round of the Delphi process (171 questions). Consensus was reached for 126 of the core competencies. These were removed for the second round of the Delphi process, which comprised 45 questions, on which agreement was reached for 14. There were 27 core competencies for which the responses were strongly disagree, disagree or neutral during these two rounds of the Delphi process. These competencies were excluded from further rounds, as there was consistency in responses by the panel. An additional seven core competencies were suggested by members of the panel during the first round. These included that trainees should be able to liberate patients from ventilation; list indications for tracheostomy; perform elective and crash induction and intubation using anaesthetic drugs; discuss indications, benefits and risks of prone positioning; discuss indications and risks of bronchoscopy; be aware of the ICU triage process and assess both in- and out-of-hospital telephonic referrals to the ICU; recognise the care limits of the current setting; and identify patients requiring a higher level of care early. These competencies were, therefore, only included in the questionnaire during the second round and only have results for round two of the Delphi process. In the third round, six remaining core competencies were circulated. Of these, consensus was reached for only one, with the other five not agreed on. The final list of core competencies is shown in Table 1.
Discussion
This study used a modified Delphi process to identify a list of core competencies that could be expected of non-intensivist medical practitioners working in healthcare settings where intensivists are often not available to direct medical treatment. The final list of core competencies included components of resuscitation and stabilisation of critically ill patients, disease management, practical procedures, health and safety management, transportation and end-of-life care.
Most core competencies were agreed upon after only one round. The following competencies were, however, only agreed upon after a second round: effects of positioning on respiratory physiology; assessment and management of spinal injury, gastrointestinal bleeding, liver failure and antepartum haemorrhage; performing transthoracic cardiac pacing and urinary catheterisation; discussion of indications and risks of bronchoscopy; and, finally, the need to have successfully completed a basic life-support course. It is possible that some of the Delphi panel members deemed many of these conditions, such as spinal injury, liver failure, gastrointestinal bleeding, antepartum haemorrhage and cardiac pacing, as areas specific to specialist care and not necessarily core competencies for non-specialists. SA, however, has a high rate of death due to pregnancy- and trauma-related complications,[20] which requires competency for managing these conditions at all levels of the healthcare system. Although urinary catheterisation is often performed by nursing personnel, doctors are invariably required to perform this procedure and should be sufficiently skilled to do so. Bronchoscopies are usually performed by pulmonologists, but it is important for clinicians working with intubated patients to know the indications for bronchoscopy and the risks involved. The requirement of Basic Life Support Course certification was only agreed upon during the second round of the Delphi process. It may, therefore, be that some Delphi panel members deemed pre-training courses irrelevant, as the accepted core competencies included cardiopulmonary resuscitation, which is the key component of the Basic Life Support Course.
The core competencies for general medical practitioners identified in our study are similar to those previously identified by Perkins et al.[21] as important for undergraduate student training as part of the Acute Care Undergraduate TEaching (ACUTE) initiative, but are not as extensive as the competencies suggested for specialist intensivists.[16,17] In SA, intensivist certification is provided by the Colleges of Medicine of South Africa (CMSA).[22] The syllabus for critical care training is designed as subspecialty training for already qualified specialists in a non-ICU discipline. This syllabus is also linked to the requirement of a dedicated 2 years, full-time ICU placement to acquire practical and procedural expertise. This is clearly an impractical approach to the training of already busy medical practitioners. A dedicated syllabus, including only the requirement for core competencies in critical care at a postgraduate diploma level, would be better suited to improve the performance of non-intensivists in dealing with critical care emergencies.
Compared with the curriculum contents of the CMSA subspecialty certificate in critical care,[22] the ACUTE initiative contains 53 of the 306 (17.3%) components, whereas our study contained 115 (37.6%). This is not unexpected, as the former is targeted at undergraduate medical students, while the core competencies identified in our study are more applicable to a training programme for qualified medical doctors who are faced with the need for a wider skill set. There is considerable overlap between the attitude and the mandatory practical skills components required for intensivists and the core components for non-intensivists identified in our study. The advisable or optional components of the subspecialty curriculum usually require specialised equipment that would not generally be available at regional or district hospitals in SA and were also not identified in our study as core competencies for general medical practitioners. There was less overlap with regard to knowledge of specific disease management, especially immunology and transplantation medicine. The curriculum of the subspecialty certificate in critical care included mandatory organisational and administrative components, which did not form part of the suggested competencies for undergraduate students or the core competencies for critical care for general medical practitioners. The competencies for the latter identified in our study can be considered as providing sufficient additional skills to address the large gap between undergraduate and specialist training.
Regarding the list of core components, the Delphi panel did not reach consensus on the intensive care management of paediatric patients. Neonatal and paediatric patients are typically managed by specialist neonatologists and paediatricians in dedicated ICUs and may therefore not be deemed a core competency for general medical practitioners at district or regional hospitals in SA. One may, however, argue that, in a resource-constrained environment with limited availability of paediatricians or paediatric intensivists, skills training in paediatrics could be beneficial.[23]
In a study among medical officers at an SA hospital, Van Deventer[24] found that the majority of the respondents lacked essential knowledge of intubation and mechanical ventilation. Similarly, junior SA doctors expressed a keen interest in managing critically ill patients, although only 13.3% were comfortable with mechanical ventilation.[25] The fixed duration of medical training limits the time available to add additional modules in critical care during undergraduate medical training, which reinforces the need for a short course or postgraduate diploma in critical care after graduation. The ideal postgraduate diploma would include supervised workplace-based training for a short period of 3 - 6 months to achieve improved competence for non-intensivists. An appropriate workplace assessment process can be incorporated into a competency-based training programme, supplemented by a summative knowledge-based component to drive learning and establish consistent standards.
Study strengths and limitations
A strength of our study was that core competencies for general medical practitioners were identified by national experts who were heads of academic critical care departments in SA. Furthermore, most of the international experts were either knowledgeable of the SA critical care environment or had experience of working in low- or middle-income countries. This is important for selecting core competencies relevant to the SA healthcare setting and could easily be fed into a training programme. All participants had an equal opportunity to voice their opinion in a blinded fashion, as separate links to the electronic questionnaires were sent to each member of the panel individually. Individual Delphi panel members were unaware of the answers provided by other members until all three rounds had been completed and results reported. This eliminated the potential for the opinion of a panel member to be influenced by dominant or prominent panel members in the field of critical care.
There were several limitations to our study. Firstly, all the experts who were invited did not respond to the invitations. The email invitations were sent out three times every 72 hours to encourage participation. The experts who did not respond may have had different opinions regarding core competencies of critical care. This deficiency might be addressed by viewing the current list of core competencies as a minimum list to which can be added, if needed. Secondly, critical care experts from the rest of the African continent were not invited to participate in the study. By including experts from the rest of Africa, alternative and valuable additional insights into expected critical care core competencies in Africa might have been gained; however, the study focused on SA, where ICU practice is currently more closely aligned with wider international practice than with our closer neighbours in Africa. Thirdly, the core competencies were not weighted in terms of importance, as occurred with the curriculum contents for subspecialists in critical care,[22] where some components are mandatory and others optional. Our study aimed to identify core competencies required and did not rank their importance.
As discussed above, consensus on competencies for paediatric intensive care could not be achieved. This deficit could be corrected in the future as an additional or optional competency.
Another limitation was the timing of the data collection. The study was conducted between January and August 2022, after the peak periods of the COVID-19 pandemic in SA. During the peak periods of COVID-19, practitioners at regional and district hospitals in SA were managing critically ill COVID-19 patients, who would otherwise have been referred to central hospitals. The expectations of the experts regarding what would be core competencies may have been influenced by the severity of illness that they would be likely to see at regional and district hospitals. It is, however, unlikely that this factor would have significantly influenced the opinions of the Delphi panel members, as they were highly experienced and knowledgeable of the SA critical care setting.
Finally, the core competencies in the final list were compiled for general medical practitioners working at SA hospitals and cannot be generalised to countries with different healthcare structures to SA.
Conclusion
By using a modified Delphi technique, a list of core competencies in critical care for medical practitioners was compiled. These competencies consist of the minimum knowledge, attitudes and skills required by medical practitioners providing critical care services outside of settings where intensivists direct the treatment of patients. We recommend that academic critical care departments at SA universities consider the list of core competencies to develop critical care training programmes for non-intensivist medical practitioners. By ensuring the competence of medical practitioners, the quality of critical care provided at district and regional hospitals in SA might be improved.
Declaration. None.
Acknowledgements. We wish to thank Mr Cornel van Rooyen, Department of Biostatistics, University of the Free State, who assisted with the statistical analysis.
Author contributions. SDM, FP and LJvdM conceptualised the study and drafted the protocol. The rest of the authors formed part of the Delphi panel. All authors contributed equally to analysing and interpreting the results, and edited and approved the final manuscript.
Funding. None.
Conflicts of interest. None.
References
1. Bradshaw D, Groenewald P, Laubscher R, et al. Initial burden of disease estimates for South Africa, 2000. S Afr Med J 2003;93(9):682-688. https://doi.org/10.7196/SAMJ.2327 [ Links ]
2. Mathivha LR. ICUs worldwide: An overview of critical care medicine in South Africa. Crit Care 2002;6(1):22-23. [ Links ]
3. Statistics South Africa. Mid-year population estimates, 2018. https://www.statssa.gov.za/publications/P0302/P03022018.pdf (accessed 2 February 2021). [ Links ]
4. Joynt GM, Gopalan DP, Argent AA, et al. The Critical Care Society of Southern Africa Consensus Statement on ICU Triage and Rationing (ConICTri). S Afr Med J 2019;109(8):613-629. https://doi.org/10.7196/SAMJ.2019.v109i8b.13947 [ Links ]
5. Department of Health. National Health Insurance for South Africa Policy, 2017. https://www.gov.za/sites/default/files/gcis_document/201707/40955gon627.pdf (accessed 9 August 2022). [ Links ]
6. Joynt GM, Zimmerman J, Li TST, Gomersall CD. A systematic review of short courses for nonspecialist education in intensive care. J Crit Care 2011;26(5):533.e1-533.e10. https://doi.org/10.1016/j.jcrc.2011.01.007 [ Links ]
7. BASIC. https://www.aic.cuhk.edu.hk/basic/faq.php (accessed 17 October 2022). [ Links ]
8. Society of Critical Care Medicine. Fundamental critical care support. https://www.sccm.org/Education-Center/Educational-Programming/Fundamentals/Fundamental-Critical-Care-Support (accessed 17 October 2022). [ Links ]
9. Health Professions Council of South Africa. Regulations relating to the registration of students, undergraduate curricula and professional examinations in medicine. Government Gazette No. 31886. 2009. [ Links ]
10. Hopkinson D, Akuamoah-Boateng K, Banguti P, et al. The impact of the fundamental critical course on knowledge acquisition in Rwanda. South Afr J Crit Care 2022;38(1):14-19. https://doi.org/10.7196/SAJCC.2022.v38i1.491 [ Links ]
11. Haniffa R, Lubell Y, Cooper BS, et al. Impact of a structured ICU training programme in resource-limited settings in Asia. PLoS ONE 2017;12(3):e0173483. https://doi.org/10.1371/journal.pone.0173483 [ Links ]
12. Skinner DL, de Vasconcellos K, Wise R, et al. Critical care admission of South African (SA) surgical patients: Results of the SA Surgical Outcomes Study. S Afr Med J 2017;107(5):411-419. https://doi.org/10.7196/SAMJ.2017.v107i5.11455 [ Links ]
13. Singh M, Maharaj R, Allorto N, Wise R. Profile of referrals to an intensive care unit from a regional hospital emergency centre in KwaZulu-Natal. Afr J Emerg Med 2021;11(4):471-476. https://doi.org/10.1016/j.afjem.2021.07.006 [ Links ]
14. Aylward RE, van der Merwe E, Pazi S, et al. Risk factors and outcomes of acute kidney injury in South African critically ill adults: A prospective cohort study. BMC Nephrol 2019;20(460). https://doi.org/10.1186/s12882-019-1620-7 [ Links ]
15. Dalkey NC. The Delphi method: An experimental study of group opinion. Futures 1969;1(5):408-426. https://doi.org/10.1016/S0016-3287(69)80025-X [ Links ]
16. CoBaTrICE Collaboration; Bion JF, Barrett H. Development of core competencies for an international training programme in intensive care medicine. Intens Care Med 2006;32(9):1371-1383. https://doi.org/10.1007/s00134-006-0215-5 [ Links ]
17. Hu X, Xi X, Ma P, et al. Consensus development of core competencies in intensive and critical care medicine training in China. Crit Care 2016;20(1):330. https://doi.org/10.1186/s13054-016-1514-z [ Links ]
18. Harris PA, Taylor R, Minor BL, et al. The REDCap consortium: Building an international community of software platform partners. J Biomed Inform 2019;95:103208. https://doi.org/10.1016/j.jbi.2019.103208 [ Links ]
19. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap) - a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform 2009;42(2):377-381. https://doi.org/10.1016/j.jbi.2008.08.010 [ Links ]
20. Pillay-van Wyk V, Msemburi W, Laubscher R, et al. Mortality trends and differentials in South Africa from 1997 to 2012: Second National Burden of Disease Study. Lancet Glob Health 2016;4(9):e642-e653. https://doi.org/10.1016/S2214-109X(16)30113-9 [ Links ]
21. Perkins GD, Barrett H, Bullock I, et al. The Acute Care Undergraduate TEaching (ACUTE) initiative: Consensus development of core competencies in acute care for undergraduates in the United Kingdom. Intens Care Med 2005;31(12):1627-1633. https://doi.org/10.1007/s00134-005-2837-4 [ Links ]
22. Colleges of Medicine of South Africa. Sub-speciality Certificate in Critical Care of the College of Physicians of South Africa (SA) Phys. https://www.cmsa.co.za/view_exam.aspx?QualificationID=75 (accessed 9 November 2022). [ Links ]
23. Bronicki RA, Pollak U, Argent AC, et al. Global perspective on training and staffing for paediatric cardiac critical care. Cardiol Young 2017;27(S6):S9-S13. https://doi.org/10.1017/S1047951117002566 [ Links ]
24. Van Deventer L. Intubation and mechanical ventilation: Knowledge of medical officers at a South African secondary hospital. S Afr Fam Prac 2014;56(3):182-185. https://doi.org/10.1080/20786204.2014.936667 [ Links ]
25. Ahmed N, Davids R. COVID-19: Are South African junior doctors prepared for critical care management outside the intensive care unit? Pan Afr Med J 2021;40(41). https://doi.org/10.11604/pamj.2021.40.41.30134 [ Links ]
 Correspondence:
Correspondence:
S D Maasdorp
maasdorpsd1@ufs.ac.za
Accepted 15 October 2023
Contribution of the study
The study provides consensus on a list of core competencies in critical care that non-intensivist medical practitioners managing critically ill patients in healthcare settings in South Africa, especially where intensivists are not readily available, should have. The list can form the core content of training programmes aimed at improving critical care competence of general medical practitioners, and in this way hopefully improve the overall outcomes of critically ill patients in South Africa.


{kind=link}