










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouthern African Journal of Critical Care (Online)
On-line version ISSN 2078-676X
Print version ISSN 1562-8264
South. Afr. j. crit. care (Online) vol.38 n.3 Pretoria Nov. 2022
http://dx.doi.org/10.7196/SAJCC.2022.v38i3.549
ARTICLE
A comparison of the warming capabilities of two Baragwanath rewarming appliances with the Hotline fluid warming device
K WilsonI; M FourtounasII; C AnamourlisIII
IMB ChB, DA (SA), Dip HIV, FCA, MMed (Anaesthesin) Department of Anesthesiology, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IIBSc (Physio), MB BCh, DA(SA) ; Department of Anesthesiology, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IIIMB BCh, MSc (Med), DA (SA), FCA, MMed (Anaesthesiol) Department of Anesthesiology, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
ABSTRACT
BACKGROUND. Accidental intraoperative hypothermia is a common and avoidable adverse event of the perioperative period and is associated with detrimental effects on multiple organ systems and postoperative patient outcomes. In a resource-limited environment, prevention of intraoperative hypothermia is often challenging. Resourceful clinicians overcome these challenges through creative devices and frugal innovations.
OBJECTIVE. To investigate the thermal performance of two Baragwanath Rewarming Appliances (BaRA) against that of the Hotline device to describe an optimal setup for these devices.
METHODS. This was a quasi-experimental laboratory study that measured the thermal performance of two BaRA devices and the Hotline device under a number of scenarios. Independent variables including fluid type, flow rate, warming temperature and warming transit distance were sequentially altered and temperatures measured along the fluid stream. Change in temperature (ΔT) was calculated as the difference between entry and exit temperature for each combination of variables for each warming device.
RESULTS. A total of 219 experiments were performed. At a temperature of 43.0°C and a transit distance of 200 cm, the BaRA A configuration either matched or exceeded the ΔT of the Hotline over all fluid type and flowrate combinations. The BaRA B configuration does not provide comparable thermal performance to the Hotline. Measured flowrates were noticeably slower than manufacturer-quoted values for all intravenous (IV) cannulae used.
CONCLUSION. A warm-water bath at 43.0°C with 200 cm of submerged IV tubing provides thermal performance comparable to the Hotline device, with all fluid type and flowrate combinations.
Keywords: perioperative hypothermia; frugal innovation; warming devices.
Accidental intraoperative hypothermia is defined as a core temperature below 36.0°C. It is a common and avoidable adverse event of the perioperative period and is associated with detrimental effects on multiple organ systems and postoperative patient outcomes.[1] The incidence of these adverse effects increases at core temperatures below 34.5°C.[2] Shivering is an unpleasant experience, and negatively contributes to a patient's perioperative experience.[3] Hypothermia increases the length of stay in the post-anaesthetic care unit, as well as in hospital, and prolongs the recovery from surgery,[4,5] which increases healthcare costs.[1] In addition, perioperative hypothermia is associated with increased surgical-site infections, altered coagulation, and altered drug metabolism.[4,6-8] The most serious adverse effects of perioperative hypothermia are related to cardiac complications. Dubick et al.[9] propose that hypothermia predisposes the heart to ischaemia and reduces the threshold of the myocardium for arrythmias. By maintaining normothermia, Frank et al.[10] found that there was a reduction in perioperative morbid cardiac events, e.g. unstable angina, cardiac arrest and myocardial ischaemia. In their recently published multicentre trial, Sessler et al.[2] have shown no difference in the rate of major adverse cardiac events between patients with intraoperative core temperatures maintained at 35.5°C and those aggressively warmed to 37.0°C.[2] This provides a reasonable target temperature for perioperative temperature management.
Considering the consequences and the incidence of perioperative hypothermia, which may occur in up to 40% of patients,[6] it is not surprising that the maintenance of normothermia is a specific perioperative goal. The importance of this is reflected in a number of local and international guidelines outlining the minimum level of care for perioperative hypothermia. The overarching aims of these guidelines are to guide best practice and ensure patient safety.
In their 2018 practice guidelines, The South African Society of Anaesthesiologists (SASA),[11] specifically mention the need to monitor patient temperature for procedures planned to take longer than 30 minutes, as well as active measures required to maintain the core temperature between 36.0 and 37.0°C. A thermometer and a blood or fluid warmer are listed as essential equipment that should be available at all hospital levels, failing which the provision of an anaesthetic becomes unsafe.[11] Similar recommendations regarding temperature monitoring and the warming of intravenous (IV) fluids are made by the Canadian Anesthesiologists' Society,[12] National Institute of Health and Care Excellence (NICE),[13] the World Health Organization (WHO) and the World Federation of Societies of Anaesthesiologists (WFSA).[14]
Anaesthesia increases the risk of hypothermia by inhibiting normal homeostatic responses that maintain the body's core temperature. The mechanisms involved in perioperative hypothermia include inhibition of the central and peripheral thermoregulatory responses by the anaesthetic agents used, an increased loss of heat to the environment through patient exposure, altered behavioural responses to the cold and administration of cold fluids internally.[1,3]
Yi et al.[15] have identified the administration of unwarmed IV fluids in excess of 1 000 mL as a risk factor for developing perioperative hypothermia. It is commonly quoted that infusing >1 L of room temperature (21°C) fluid into an adult will reduce the core body temperature by 0.25°C.[16,17] Sixteen kilocalories of energy are needed to warm a litre of fluid from room temperature to a core body temperature of 37.0°C.[18] Various methods have been described to prewarm IV fluids before administration. These include storing the fluid in a fluid-warming cabinet,[1-prewarming the fluids in a warm-water bath[19-or heating the fluid in a microwave.[20] These methods have been shown to be superior at maintaining core temperature (compared with administering room-temperature fluid) and are also comparable with the performance of commercially available in-line fluid-warming devices such as the Hotline apparatus (ICU Medical Inc., USA).[1]
Resource-limited settings challenge the delivery of acceptable levels of care and low-and middle-income countries are most affected. In response to these constraints, a number of creative solutions have been constructed to warm fluids. There are many anecdotal stories of blood products being warmed in warm blankets, buckets of warm water or even in groins and axillae before being administered to patients. Recommendations have been published on the optimal use of these creative solutions. Lindhoff and Palmer[20] described the optimal use of a microwave for prewarming IV fluids.[20] Shah et al.[21] described a novel fluid-warming device using a non-sterile latex glove filled with warmed water to heat a coil of IV fluid being administered to the patient. Craig et al.[22] described a method of prewarming IV fluids using a warm air blower and a modified cooler box. It is common practice at Chris Hani Baragwanath Academic Hospital (CHBAH) to warm IV fluid by passing the IV tubing through a warm-water bath as it flows to the patient. This sort of Baragwanath Rewarming Appliance (BaRA) is an example of a novel technology that addresses the need to provide acceptable anaesthetic care in a resource-limited setting; however, an assessment of the performance of these devices is lacking.
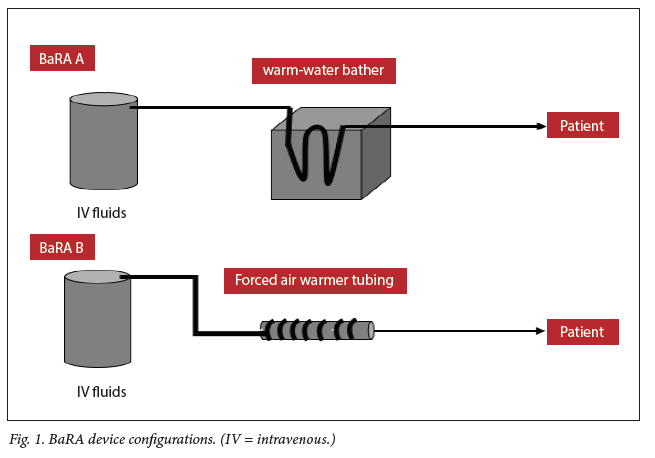
The two BaRA configurations used in the present study are shown in Fig. 1. BaRA A consists of a warm-water bath with a variable amount of IV extension tubing submerged in it. BaRA B consists of a variable amount of IV extension tubing wrapped around the tubing of a forced-air warmer, Bair Hugger (3M, USA).
The aim of the present study was to describe and compare the warming capabilities of two BaRA devices and the Hotline device to describe an optimal assembly of these devices that approximates the warming capabilities of the commercially available Hotline device.
Ethics
Ethical clearance was obtained from the Wits Human Research Ethics Committee (Medical) (ref. no. M2008107) and permission to use human blood products was obtained from the South African National Blood Services (ref. no. 2019/0520).
Methods
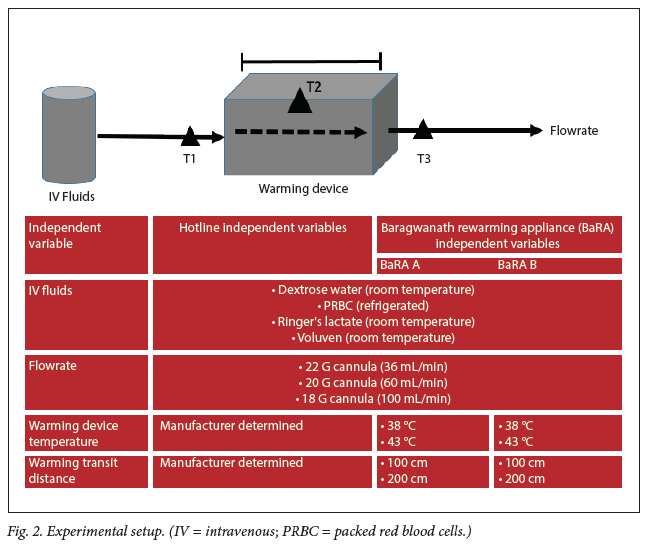
A quasi-experimental, quantitative research design was employed in the present study. The study was conducted in an unused, fu ly operational surgical theatre at CHBAH using standardised 20 drops/min IV and 10 drops/min blood administration sets and IV cannulae. Dextrose water was included in the study as an electrolyte-free control fluid. IV fluids were kept at a standard 1 m height above the warming device to control driving pressure. Ambient air temperature and fluid temperatures were continuously monitored for fluctuations during the experiments. Under experimental conditions, independent variables relating to the Hotline, BaRA A and BaRA B devices were sequentially altered to assess the effect on temperature at points T1 and T3, the dependent variables. Fig. 2 illustrates the experiment setup, the independent variables related to each warming device and the location of the temperature measurement points. Actual flowrates for each cannula were measured.
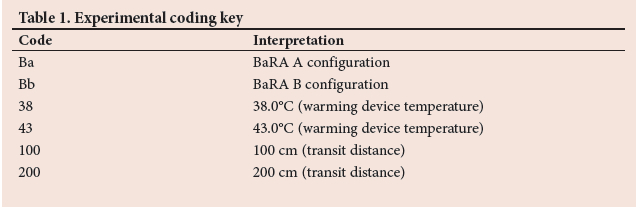
The independent variables for each BaRA configuration were assigned a code which described the warming device configuration, e.g. Ba.43.200. Table 1 outlines the coding system. Twelve combinations of independent variables were tested for the Hotline and 48 combinations were tested for each BaRA configuration, totalling 108 experimental combinations.
Temperature was recorded at six points and stored by a multichannel thermistor and data capture software (BaRAGRABA 2.0), both specifically designed for the experiment. Full details on device and software construction and calibration are available as a supplement (https://www.samedical.org/file/1952). In-stream temperatures were recorded at T1 and T3. T2 was monitored to maintain warming device temperature for the BaRA A experiments. Hotline and BaRA B temperatures were determined by the individual devices. Ambient temperature and in-line fluid temperature were also recorded and monitored at two distal points to control experimental conditions.
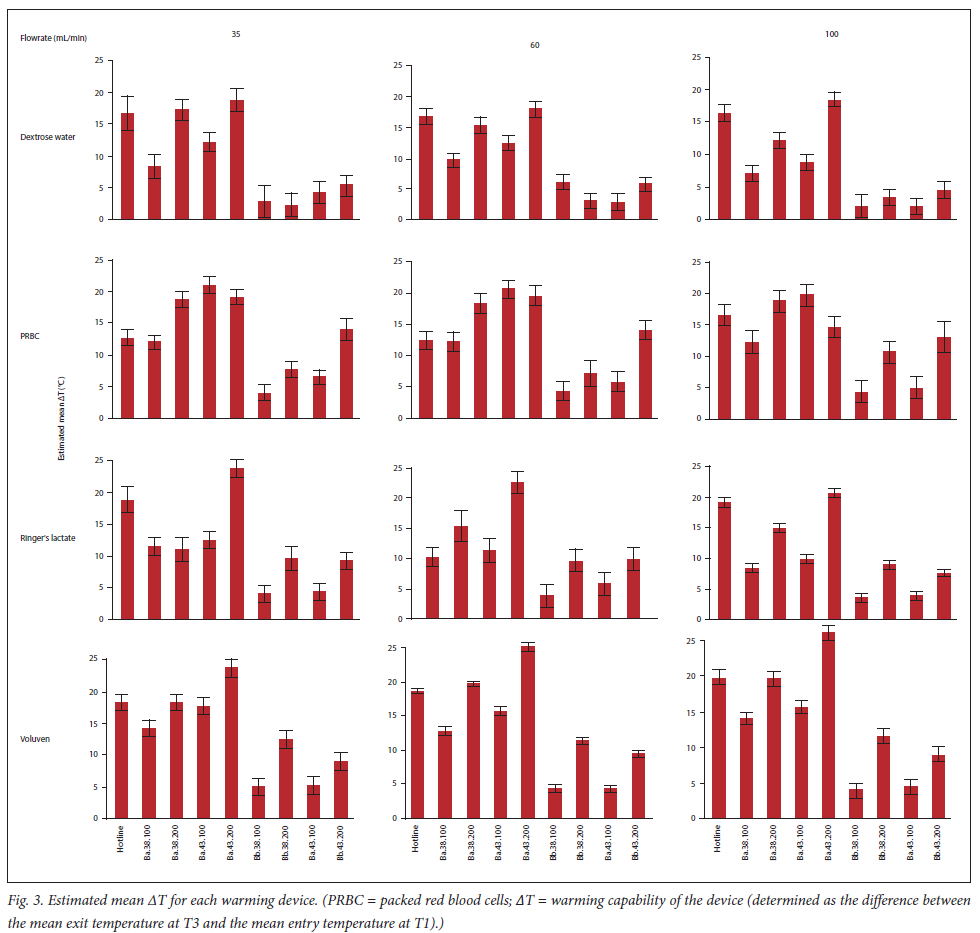
Temperature measurements were recorded automatically at 500 ms intervals for a period equal to the transit period plus 5 seconds. The transit period was calculated as the time taken for an indicatorbubble to trave from T1 to T3. These temperature measurements were automatically measured and saved digitally. The warming capability of the device was determined as the difference between the mean exit temperature at T3 and the mean entry temperature at T1 (ΔT).
Data analysis was carried out using SAS v9.4 for Windows (SAS, USA). A 5% significance level was used. Each dependent variable, for each warming device, was modelled in terms of the relevant independent variables and their two-way interactions using a general linear model (GLM). Outliers were removed as indicated by model diagnostics. Nonsignificant interaction terms were removed for model parsimony. A one-way ANOVA was used for comparison of each dependent variable for the Hotline to that of the eight corresponding BaRA A and BaRA B device conditions at a given combination of fluid type and flowrate. Post hoc tests were conducted using the Tukey-Kramer adjustment for unequal group sizes to determine which BaRA A and BaRA B combinations did not differ significantly from the Hotline device readings.
Results
Experiments were conducted twice at each combination of independent variables, giving a total of 216 experiments. Data for nine experiments were missing owing to file errors. The estimated mean AT, with associated 95% confidence intervals of the warming devices at each combination of the independent variables are shown in the supplementary Table 1 (https://www. samedical.org/file/1952) and Fig. 3.
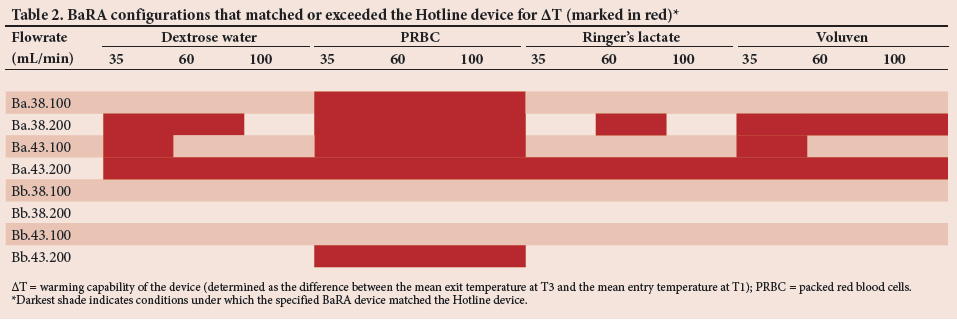
Table 2 shows the BaRA combinations, marked in black, where ΔT matched or exceeded the Hotline device. Ba.43.200 was the only configuration that provided a similar ΔT to the Hotline device under all fluid and flowrate combinations. Other BaRA A configurations provided comparable ΔT values but only under specific fluid and flowrate combinations. When packed red blood cells (PRBC) were utilised all configurations of BaRA A had ΔT values similar to the Hotline device.
The BaRA B devices only approximated the ΔT of the Hotline in the Bb.43.200 configuration and only when PRBC were used. No other combination of variables of this device approximated the Hotline ΔT readings.
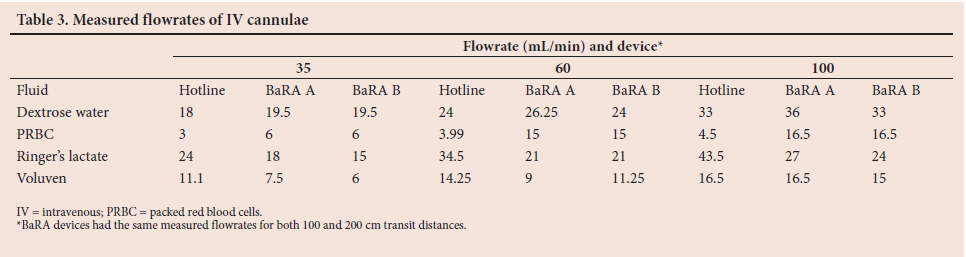
Table 3 shows the measured flowrates for each fluid through each warming device. There was a large difference between the manufacturer-stated flowrates and the measured flowrates for each cannula. Flowrates also varied substantially between fluids in the case of PRBC. PRBC and Voluven had the lowest flowrates of all fluids through all devices and at all flowrates. PRBC had notably lower flowrates through the Hotline device at all flowrates.
Discussion
The aim of the present study was to describe and compare the warming capabilities of two BaRA devices with the commercially available Hotline device to describe a configuration of the BaRA device that would best approximate the warming capabilities of the Hotline device. Table 2 illustrates that Ba.43.200a provides a one-combination-fits-all match for the thermal performance of the Hotline, i.e. the BaRA A configuration with a warming temperature of 43.0°C and a transit distance of 200 cm. There are a number of isolated conditions for the BaRA A configuration which approximate the Hotline but only under specific fluid and flowrate combinations. The BaRA B configuration did not provide a comparable amount of heating compared with the Hotline device under most fluid type and flowrate combinations; however, the warming performance was similar to that of the Hotline under condition Bb.43.200.
The transfer of heat energy from the warming device to the fluid is proportional to the surface area available for heat transfer. The entire surface area of the extension tubing is included in heat transfer in both the Hotline and BaRA A devices as it is either enveloped by or submerged in the warming device. This superior warming effect by a co-axial system has been described in a previous study by Shultz et al.[19] The BaRA B device has only a fraction of the tubing surface area in contact with the warming device as it is coiled on the outer surface of the Bair Hugger warmer conduit.
Fluid transit time is a function of the fluid flowrate and transit distance. Longer transit times allow for greater heating of the fluid. Thongsukh et al.[16] have previously shown the inverse relationship between flowrate and warming device performance. Interestingly, the measured flows were only ~5 - 55% of manufacturer-quoted flows. Measured fluid flowrates were much higher with less viscous fluids such as dextrose water and Ringer's lactate, and decreased as viscosity increased, i.e. when using PRBC and Voluven. The significance of this is that more viscous fluids had longer transit times and resultant increased heating. This may explain why PRBC were better heated compared with other fluids under both BaRA A and B configurations. It is noteworthy that the PRBC flowed slower through the Hotline than the other two devices. Thermistors were mounted within the flow of fluids (https://www.samedical.org/file/1952) and may have also affected flowrates. These factors are important considerations when interpreting the results of the present study. It is worth noting that the conclusions of the study may no longer be valid at higher flowrates.
Study limitations
There were a few technical challenges with the conduct of the study. Firstly, the study was quasi-experimental as no randomisation was performed. This potentially allows repeat error to bias a particular experimental condition. The reason for this design was to ensure efficient use of resources and time and, most importantly, PRBC. Secondly, it was not anticipated that the electrolyte solutions would alter the readings of the thermistors. This was indeed the case - the thermistor leads required insulation and recalibration. Dextrose water was included in the study as a control for the effects of the electrolytes on the thermistors. After insulation there were comparable readings at all temperature points with all fluids.
The use of an analogue electronic system, such as the multichannel thermistor, poses a number of challenges. As the system increases in complexity, and more thermistors are added, electrical interference within the system increases and calibration becomes more difficult and less reliable. This may affect the measurement of absolute temperatures, as they are calculated indirectly through the Steinhart-Hart equation. The relative changes between temperatures such as ΔT should not be affected as the relationship between temperature and resistance remains fixed within the system, however, a digital temperature monitoring device would be an ideal upgrade over the analogue system employed in the present study. Finally, the BaRAGRABA 2.0 corrupted 9 (of 216) data sets. Despite this loss, many data points were available for statistical comparison.
Conclusion
Despite a number of technical challenges, the findings of the study provide valuable insights into the use of the BaRA devices as alternatives to the Hotline device. To the best knowledge of the authors, this is the first study that compares the warming capabilities of the Hotline with the BaRA devices. Resource-limited settings challenge the provision of adequate levels of perioperative care. Sessler et al.[2-have shown that a reasonable target core temperature is between 35.5 and 37.0°C. Providing adequately warmed IV fluids forms a major part of maintaining this target range in the perioperative period. The BaRA A can be constructed easily from basic consumables found in most clinical settings and at a fraction of the cost of the Hotline device and its consumables. This device is not limited to the warming of fluids during the perioperative period but can be constructed in any setting requiring the provision of warmed IV fluids. The requirements for constructing the BaRA A are a container of water warmed to 43.0°C and 200 cm of IV extension tubing. With this length of IV extension tubing submerged in the container of warm water, the configuration should provide warming of dextrose water, Ringer's lactate, PRBC and Voluven through IV cannulae at flowrates of 36, 60 and 100 mL/min, respectively, that is comparable with the Hotline device. The challenges outlined in the study may assist in the future design of a similar study.
Declaration. This study was performed in partial fulfilment of the requirements of KW's MMed degree.
Acknowledgements. We acknowledge the statistical consultation services of Data Management and Statistical Analysis (DMSA) in the preparation of the results. We would like to thank the CHBAH Department of Anaesthesiology for access to valuable resources to complete this study.
Author contributions. KW: conceptualisation, methodology, software, investigation, writing (original draft); MF: supervision, methodology, writing, review and editing; CA: supervision, methodology, writing, review and editing.
Funding. The CHBA H Department of Anaesthesiology bore the cost of printing and paper for the postgraduate approval as well as the consumables, excluding the blood products for the experiments. The blood products were supplied by SANBS at no additional cost. KW provided the funds for the multichannel thermistor, statistician and data capture software.
Conflicts of interest. None.
References
1. John M, Ford J, Harper M. Peri-operative warming devices: Performance and clinical application. Anaesthesia 2014;69(6):623-638. https://doi.org/10.1111/anae.12626 [ Links ]
2. Sessler DI, Pei L, Li K, et al. Aggressive intraoperative warming versus routine thermal management during non-cardiac surgery (PROTECT): A multicentre, parallel group, superiority trial. Lancet 2022;399(10337):1799-1808. https://doi.org/10.1016/S0140-6736(22)00560-8 [ Links ]
3. Campbell G, Alderson P, Smith AF, Warttig S. Warming of intravenous and irrigation fluids for preventing inadvertent perioperative hypothermia. Cochrane Database Syst Rev 2015;2015(4):1-62. https://doi.org/10.1002/14651858.CD009891.pub2 [ Links ]
4. Kurz A, Sessler DI, Lenhardt R. Perioperative normothermia to reduce the incidence of surgical-wound infection and shorten hospitalisation. Study of Wound Infection and Temperature Group. N Engl J Med 1996;334(19):1209-1215. https://doi.org/10.1056/NEJM199605093341901 [ Links ]
5. Lenhardt R, Marker E, Goll V, Mild intraoperative hypothermia prolongs postanesthetic recovery. Anesthesiology 1997;87(6):1318-1323. https://doi.org/10.1097/00000542-199712000-00009 [ Links ]
6. Melling AC, Ali B, Scott EM, Leaper DJ. Effects of preoperative warming on the incidence of wound infection after clean surgery: A randomised controlled trial. Lancet 2001;358(9285):876-880. https://doi.org/10.1016/S0140-6736(01)06071-8 [ Links ]
7. Heier T, Caldwell JE. Impact of hypothermia on the response to neuromuscular blocking drugs. Anesthesiology 2006;104(5):1070-1080. https://doi.org/10.1097/00000542-200605000-00025 [ Links ]
8. Rajagopalan S, Mascha E, Na J, Sessler DI. The effects of mild perioperative hypothermia on blood loss and transfusion requirement. Anesthesiology 2008;108(1):71-77. https://doi.org/10.1097/01.anes.0000296719.73450.52 [ Links ]
9. Dubick MA, Brooks DE, Macaitis JM, Bice TG, Moreau AR, Holcomb JB. Evaluation of commercially available fluid-warming devices for use in forward surgical and combat areas. Mil Med 2005;170(1):76-82. https://doi.org/10.7205/milmed.170.L76 [ Links ]
10. Frank SM, Fleisher LA, Breslow MJ, et al. Perioperative maintenance of normothermia reduces the incidence of morbid cardiac events. A randomised clinical trial. JAMA 1997;277(14):1127-1134. https://doi.org/10.1001/jama.1997.03540380041029 [ Links ]
11. South African Society of Anaesthesiologists. Practice Guidelines 2018 Revision. SAJAA 2018;24(2):1-58. https://sasaapi.sasaweb.com/Document/SAJAA(V24N1)2061SASAPracticeGuidel ines_V12_636803016948256880.pdf (accessed June 2020). [ Links ]
12. Dobson G, Chow L, Flexman A, et al. Guidelines to the Practice of Anesthesia - Revised Edition 2019. Can J Anesthesia 2019,66(1):75-108. https://doi.org/10.1007/s12630-018-1248-2 [ Links ]
13. National Institute for Health and Care Excellence. Hypothermia: Prevention and Management in Adults Having Surgery (NICE Guideline 65). London: NICE, 2008. http://nice.org.uk/guidance/cg65 (accessed 5 March 2020). [ Links ]
14. Gelb AW, Morriss WW, Johnson W, et al. World Health Organization-World Federation of Societies of Anaesthesiologists (WHO-WFSA) International Standards for a Safe Practice of Anesthesia. Can J Anaesth 2018;65(6):698-708. https://doi.org/10.1007/s12630-018-1111-5 [ Links ]
15. Yi J, Lei Y, Xu S,et al. Intraoperative hypothermia and its clinical outcomes in patients undergoing general anesthesia: National study in China. PLoS ONE 2017;12(6):1-13. https://doi.org/10.1371/journal.pone.0177221 [ Links ]
16. Thongsukh V, Kositratana C, Jandonpai A. Effect of fluid flow rate on efficacy of fluid warmer: An in vitro experimental study. Anesthesiol Res Pract 2018;2018:1-4. https://doi.org/10.1155/2018/8792125 [ Links ]
17. Sessler DI. Mild perioperative hypothermia. N Engl J Med 1997;336(24):1730-1737. https://doi.org/10.1056/nejm199706123362407 [ Links ]
18. Horosz B, Malec-Milewska M. Methods to prevent intraoperative hypothermia. Anaesthesiol Intensive Ther 2014;46(2):96-100. https://doi.org/10.5603/AIT.2014.0019 [ Links ]
19. Schultz J, Sims C, Bissonnette B. Methods for warming intravenous fluid in small volumes. Can J Anaesth 1998;45(11):1110-1115. https://doi.org/10.1007/BF03012402 [ Links ]
20. Lindhoff G, Mac G Palmer J. An assessment of the thermal safety of microwave warming of crystalloid fluids. Anaesthesia 2000;55(3):251-254. https://doi.org/10.1046j.1365-2044.2000.01319.x [ Links ]
21. Shah S, Hariharan U, Bhargava A. A novel fluid-and blood-warming technique for the developing world. Int J Health Allied Sci 2015;4(1):58-59. https://doi.org/10.4103/2278-344x.149278 [ Links ]
22. Craig R, Peoples GE. A novel device developed, tested, and used for warming and maintaining intravenous fluids in a forward surgical team during Operation Enduring Freedom. Mil Med 2006;171(6):500-503. https://doi.org/10.7205/milmed.171.6.500 [ Links ]
 Correspondence:
Correspondence:
K Wilson
mostoman@gmail.com
Accepted 11 August 2022
Contribution of the study. The present study provides an evidence-based method for warming intravenous fluid in resource-limited scenarios.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}