










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouthern African Journal of Critical Care (Online)
versão On-line ISSN 2078-676X
versão impressa ISSN 1562-8264
South. Afr. j. crit. care (Online) vol.38 no.2 Pretoria Jul. 2022
http://dx.doi.org/10.7196/SAJCC.2022.v38i2.539
RESEARCH
Iatrogenic blood loss in critical care: A prospective observational study conducted at Universitas Academic Hospital in the Free State Province, South Africa
J C AdamsI; C BarrettII; M SpruytIII
IBSc, BSc Hons, MB ChB; MMed (Surg), FCS (SA) ; Department of Surgery, Faculty of Health Sciences, University of the Free State, Bloemfontein, South Africa
IIMB ChB, PG Dip Transf Med, MMed (Int Med), FCP (SA) ; School of Clinical Medicine, Faculty of Health Sciences, University of the Free State, Bloemfontein, South Africa
IIIMB ChB, MMed (Surg); Department of Critical Care, Faculty of Health Sciences, University of the Free State, Bloemfontein, South Africa
ABSTRACT
BACKGROUND. Prevention of iatrogenic blood loss is an essential component of patient blood management (PBM) in intensive care units (ICUs). The amount of iatrogenic blood loss from diagnostic phlebotomy in the ICUs at Universitas Academic Hospital, Free State Province, South Africa, is unknown.
OBJECTIVE. To quantify diagnostic phlebotomy volumes, and volumes submitted in excess for diagnostic testing in the ICU.
METHODS. We conducted a prospective descriptive observational study on adults who were admitted to ICUs at a single centre over a period of 14 days. The weight of each filled phlebotomy tube was calculated using the specific gravity of blood and averages of empty phlebotomy tubes, establishing the total volume.
RESULTS. Data from 59 participants with a median length of stay at the ICU of 3 days were analysed. The median phlebotomy volume was 7.0 mL day and 13.6 mL/ICU admission. The volume of blood required for analysis daily and ICU admission was 0.7 mL and 2.2 mL, respectively. The median phlebotomy volume in excess of the amount required for analysis daily and ICU admission was 5.05 mL and 12.11 mL, respectively.
CONCLUSION. While the median excess daily phlebotomy volume in this present study may seem insignificant and underestimating the true excess of phlebotomy volume, interventions to reduce phlebotomy volumes and development of a PBM guideline for appropriate phlebotomy volumes and preventing wastage of patients' blood in the ICU is required.
Keywords:Critical care, diagnostic blood loss, ICU, patient blood management, phlebotomy volume.
Phlebotomy for diagnostic laboratory investigations is an integral part of the management of a patient in the intensive care unit (ICU). While important in the care of these patients, phlebotomy is an independent risk factor for the development of anaemia and transfusion in the ICU.[1] Anaemia and progression of underlying anaemia is one of the most common clinical events in patients admitted to the ICU, and is associated with increased morbidity and length of hospital stay, independent of blood transfusion.[1-3] Several observational studies have demonstrated that transfusion is independently associated with adverse outcomes.[4-8]
Iatrogenic blood loss is one of the few modifiable risk factors for anaemia and transfusion in critically ill patients, and even minor reductions may significantly reduce the number of transfusions.[9-Phlebotomy volume has been proposed as a quality metric for inter-institutional benchmarking.[10] While devices to reduce the phlebotomy volume in the ICU have been proposed and tested, findings are inconsistent, and despite showing as much as an 80% reduction in phlebotomy volume, there has been poor uptake of these devices. Small volume tubes have also been shown to reduce phlebotomy volume without affecting the reliability of laboratory tests, but these may require adaptations to procurement and laboratory processes.[11] These and other interventions, form part of a phlebotomy-reduction strategy that should be implemented as part of a phlebotomy stewardship programme in the ICU.
Patient blood management (PBM) is defined as 'a patient-centred, systematic, evidence-based approach to improve patient outcomes by managing and preserving a patient's own blood, while promoting patient safety and empowerment'.[5] PBM comprises three pillars namely, optimising red blood cells mass production, diminishing blood loss and enhancing the physiological reserve of anaemia.[12] All these strategies are based on the principle of patient-centred decision making.[13] Observational studies have shown improvement in patient outcomes and a reduction in costs when PBM principles are applied.[12] These findings demand the transformation of transfusion practices and warrant a paradigm shift from reflexively treating anaemia with transfusion, to applying the principles of PBM.[14
Local data on the various aspects of PBM are critical to establish a baseline against which phlebotomy stewardship interventions can be measured. Iatrogenic blood loss due to diagnostic testing in the ICU at Universitas Academic Hospital (UAH), Free State Province, South Africa (SA), has not previously been determined.
The aim of the study was to describe the diagnostic phlebotomy practices pertaining to ICU patients for the 14-day period between 7 and 20 October 2019. The objectives of this study were to (i) determine the number and type of collection tubes submitted to the laboratory; (ii) describe the laboratory investigations requested for each patient; (iii) determine the volume of blood submitted for diagnostic testing; and (iv) determine the volume of blood submitted in excess of what is required to perform routine testing.
Methods
Study design
A prospective descriptive observational study was performed. The sample size was determined based on the number of ICU beds (32) at UAH. We anticipated a minimum sample size of 48 participants over the study period based on a 75% bed occupancy.
Setting
UAH is a tertiary academic hospital that has a 6-bed cardiology ICU (CICU), 10-bed multidisciplinary unit (MDICU), 8-bed cardiothoracic ICU (CTU), 4-bed neurosurgical ICU (NSICU) and a 4-bed surgical ICU (SICU). Patients admitted to any of these ICUs were eligible for participation in the study.
Participants
All adult patients admitted to any of the ICUs during the period of 7 -20 October 2019 were screened for eligibility. Eligibility criteria were age >18 years and ICU admission for >24 hours. All eligible patients were approached to participate in the study. Potential participants or their legal representatives were given an information document and informed consent documents. Consenting participants were followed up daily for the duration of the study period. Phlebotomy samples submitted to the National Health Laboratory Service (NHLS) were included in the study. We excluded samples that were submitted to an off-site pharmacology laboratory for blood transfusion compatibility testing and samples for arterial blood gas analysis and other point-of-care (POC) testing. All measurements of the samples were done at the NHLS where a calibrated scale was available.
Variables
Demographic information collected, included date of birth, gender, admission date, reason for admission, ICU type and outcome (whether deceased, discharged to ward or still in ICU). Other variables were tests requested, the type and number of blood tubes used for drawing blood and the blood volume per tube.
Data sources
All samples were drawn according to the primary attending clinician's instruction and submitted to the NHLS in Becton Dickinson Vacutainer tubes (BD Vacutainer, USA). As none of the units have standard phlebotomy guidelines, laboratory investigations may have been drawn from a central venous line, arterial line, other invasive device or from venesection if no invasive device was placed. No study-related instruction was given to nurses as the researcher aimed to determine the trends in usual practice. Nursing staff performed phlebotomy according to the unit specific routine practice for laboratory analysis between 4 am and 6 am daily. After phlebotomy, each specimen had a barcode affixed to it, as per standard practice.
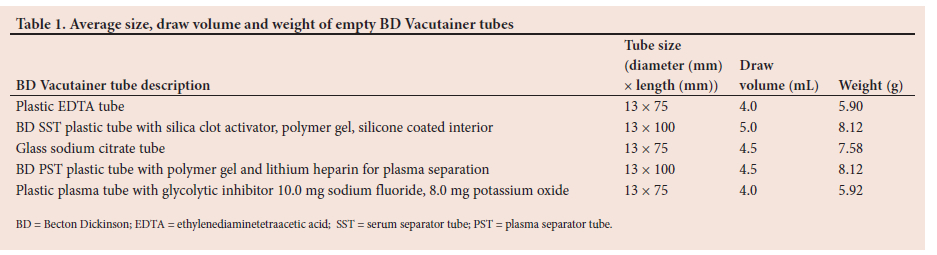
Each tube was individually weighed using the NHLS calibrated balanced scale (Sartorius, Germany). Specimen barcodes were used to trace the tests requested and participant information. The average weight of an empty BD vacutainer tube was determined using the Sartorius scale. The physical variables of the empty tubes are summarised in Table 1.
The weight of the empty vacutainer tube was subtracted from the weight of the tube filled with blood to obtain the weight of the blood at room temperature. The density of blood is 1.06 g/mL.'15] The weight of the blood was divided by 1.06 g/mL and the quotient used to estimate the volume of blood in the vacutainer tube.
Due to the study population, it was expected that additional specimens would be sent to the laboratory through the day. To capture this blood volume, each additional test was traced on LabTrak (Intersystems Corporation, USA), the electronic laboratory information system used by the NHLS. The researcher visited the laboratory daily and recorded the numbers, type of tubes and additional blood tests requested. These specimens were not weighed and were included in the analysis under additional tubes and tests only.
Clinical data were obtained by reviewing patient files. No identifying participant information was collected.
Statistical analysis
Study data were collected and managed using Research Electronic Data Capture (REDCap) software hosted by the University of the Free State. REDCap is a secure, web-based software platform designed to support data capture for research studies.[16,17]
Data were provided to the Department of Biostatistics in Microsoft Excel spreadsheet (Microsoft Corp., USA) for analysis. Numerical data were reported as medians and interquartile ranges (IQR), categorical data as proportions by means of frequency and percentiles. Calculations were performed to determine the volume of blood in excess of that was needed per test. The data was analysed using SAS statistical software, version 9.4 (SAS Institute Inc., USA).
Ethical considerations
Ethical approval to conduct the present study was obtained from the Free State Province Department of Health and the Health Sciences Research Ethics Committee of the University of the Free State (ref. no. HSD-2019/0920/2910-0002). Permission to perform the data analysis on phlebotomy samples submitted to the NHLS was obtained from the business manager.
Results
Participants
The study included 59 participants who were recruited during the 14-day study period. Complete data were not available for five participants, although demographic data and analysable data of these participants were included in the analyses. The median (IQR) age was 56 (45 - 66) years and 50.9% (n=30) of participants were female. More than a quarter of participants (27.1%; n=16) were admitted to the CICU, 16.9% (n=10) were admitted to CTU, 25.4% (n=15) were admitted to MDICU, 11.9% (n=7) were admitted to NSICU and 18.6% (n=11) were admitted to SICU. Half of the participants (50.9%; n=30) were admitted for post-operative care, 27.1% (n=16) for nonsurgical cardiac conditions, 13.6% (n=8) were medical patients and 8.5% (n=5) for other surgical conditions requiring intensive care. The other surgical conditions included a post-angiogram cerebral aneurysm, a polytrauma patient with thoracic aortic dissection, upper gastrointestinal haemorrhage with variceal bleed, critical limb ischaemia (n=2), one of whom required thrombolysis. The median (IQR) length of stay in the ICU was 3 (2 - 7) days.
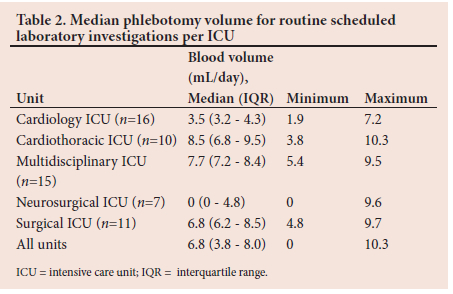
Routine phlebotomy volumes
A difference in the median volume of blood drawn for routine scheduled laboratory investigations was noted per unit (Table 2). The median phlebotomy volume for routine scheduled laboratory investigations was the lowest in the NSICU (0 mL/day), followed by the CICU (3.5 mL/day) and the highest was in the CTU (8.5 mL/day).
Number and type of Vacutainer tubes drawn
The median (IQR) number of tubes submitted per participant per day was 2 (1.7 - 2.3). The median (IQR) total number of tubes submitted per patient during their ICU admission was 4 (2 - 8) tubes. Of the total number of 342 tubes that were submitted to the NHLS, 37.4% (n=128) were EDTA tubes, 49.4% (n=169) were SST tubes and 13.2% (n=45) were citrate tubes.
Additional blood tests requested
The median (IQR) number of additional tubes per participant per day was 1 (1 - 1.36). The median (IQR) number of additional tests per participant per day was 5.5 (4 - 7). The median (IQR) number of additional tubes submitted per participant during their ICU admission was 3 (2 - 6). The median (IQR) number of additional laboratory tests requested per patient for their duration of ICU admission was 7 (5 - 15). The additional tubes and tests were mainly for five participants who had phlebotomy performed outside the scheduled collection times.
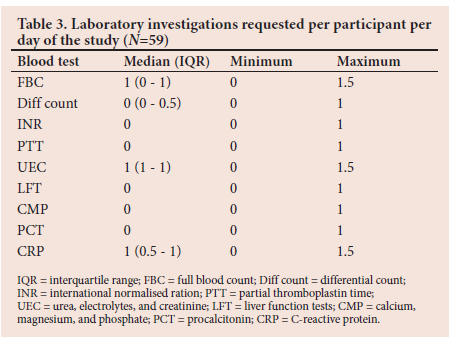
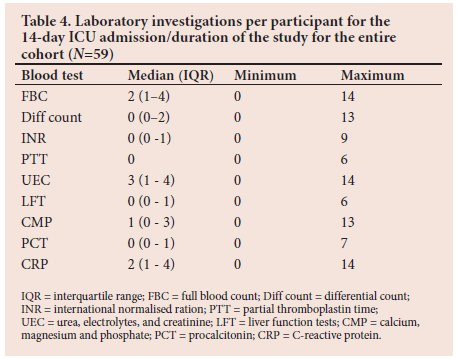
Laboratory investigations requested
The median (IQR) daily number of tests per participant during their ICU admission was 4 (2 - 5). The median (IQR) number of tests requested over the duration of their ICU admission was 7 (3 - 16). Table 3 represents the laboratory investigations per participant per day, and Table 4 summarises the laboratory investigations per participant for the duration of the 14-day ICU admission.
The volume of blood submitted for diagnostic testing
The median (IQR) total blood volume submitted was 13.6 (7.8 - 27 .8) mL per participant for the duration of their ICU stay. This comprised a median (IQR) of 7.3 (3.7 - 14.2) mL for EDTA tubes, 7.9 (4.3 - 14.4) mL for SST tubes and 8.9 (4.4 - 15.0) mL for citrate tubes.
The median (IQR) blood volume submitted per participant per day was 7.0 (4.7 - 8.6) mL for the duration of their ICU admission. The median daily blood volume for specific tubes submitted per participant per day was 3.3 (2.6 - 3.6) mL for EDTA tubes, 3.6 (3.2 - 4.1) mL for SST tubes and 4.3 (4.1 - 4.4) mL for citrate tubes.
The total iatrogenic blood volume submitted from all participants over the 14-day study period was 1 241.4 mL. The required blood volume for diagnostic laboratory testing was 323.2 mL.
Volume of blood required by the laboratory to perform diagnostic testing over the 14-day study period
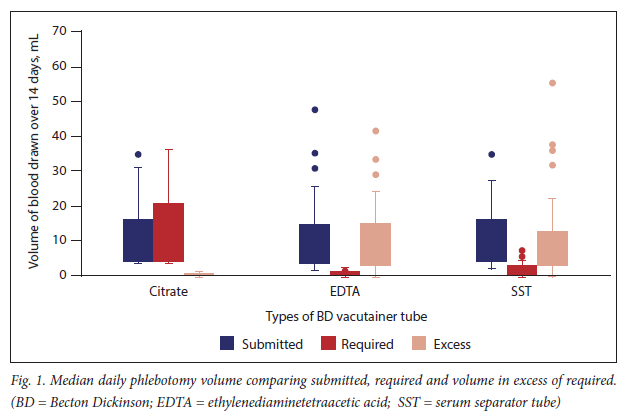
The median (IQR) blood volume required by the laboratory to perform the required tests was 0.7 (0.7 - 1.2) mL per patient per day. The required median (IQR) volume to perform requested tests per patient for their duration of ICU stay was 2.2 (0.7 - 6.7) mL. Fig. 1 shows the blood volume submitted compared with the blood volume required by the laboratory, as well as volumes in excess of the required volume. The median (IQR) blood volume submitted in excess per patient for the duration of the ICU admission was 12.1 (5.2 - 24.1) mL.
The average volume of blood required to perform laboratory tests in specific tubes was 0.2 mL for EDTA tubes, 0.6 mL for SST tubes and 4.5 mL for citrate tubes. The median (IQR) blood volume submitted per participant for specific tubes for their duration of ICU admission was 7.3 (3.7 - 15.0) mL for EDTA tubes, 7.9 (4.3 - 14.4) mL for SST tubes and 8.9 (4.6 - 15.0) mL for citrate tubes. The median (IQR) blood volume in excess submitted per participant for specific tubes was 6.9 (3.3 - 13.5) mL for EDTA tubes and 6.7 (3.6 - 12.2) mL for SST tubes for their duration of ICU admission.
Daily phlebotomy volume submitted in excess of the minimum required to perform analysis
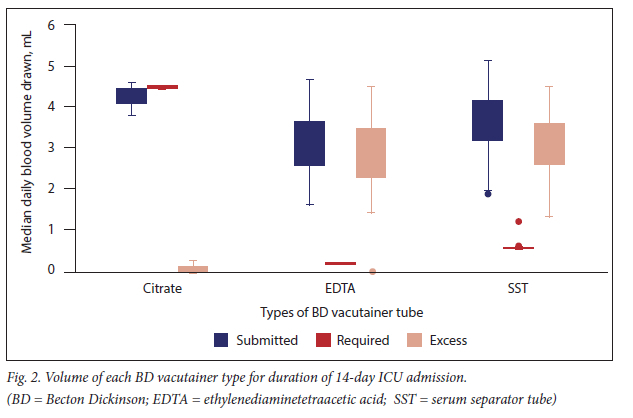
The median (IQR) daily volume per participant submitted in excess for all diagnostic testing was 5.1 (4.7 - 6.5) mL. The median (IQR) phlebotomy volume in excess per participant for each specific collection tube was 3.16 (2.3 - 3.4) mL for EDTA tubes and 3.1 (2.6 - 3.6) mL for SST tubes. Citrate tubes were frequently under-filled (56.3%; n=9/16) and never overfilled. Citrate tubes require 4.5 mL of blood and should not be under-filled. The breakdown of blood volumes submitted, required and in excess are shown in Fig. 2.
Discussion
We prospectively quantified diagnostic blood loss in a single-centre tertiary hospital. We aimed to quantify the volume of blood loss due to routine phlebotomy practice.
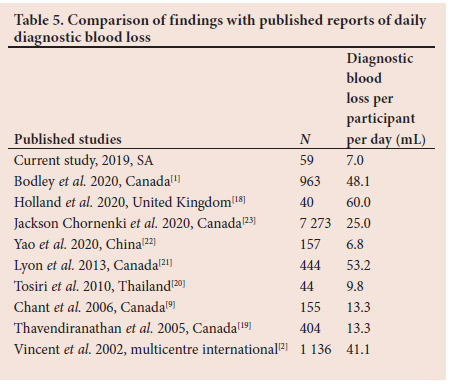
The diagnostic blood loss was substantially lower in this study compared with a majority of previously reported studies quantifying daily and overall ICU admission phlebotomy blood loss (Table 5).[1,9,18-23]
Phlebotomy volume compared with the volume required to perform analyses showed that phlebotomy was almost always in excess of what was needed, the only exception being citrate tubes. It was notable that citrate tubes were frequently under-filled, giving a false impression of restrictive blood draws. However, this could contribute to excess blood draws as tests needed to be repeated.
While these volumes may seem to be insignificant, it has been shown that median (IQR) blood volumes of as little as 3.5 (2.4 - 6.8) mL/day drawn in excess may double the odds of being transfused after 21 days in ICU.[9] The association between diagnostic phlebotomy and transfusion has been reported by an extensive multicentre study that included 7 273 patients.[23] Furthermore, other studies have shown that diagnostic testing contributes to ICU-acquired anaemia.[1,9,18-20]
Earlier studies reported similar daily phlebotomy losses ranging from 40 - 70 mL per day of ICU admission.[1,2,24] In comparison with international studies, our findings reflected non-significant volumes of blood loss, which could be attributed to the shorter study period and high patient turn-over.
Our study did not measure the volume of blood discarded during vascular access, which has been shown to contribute to blood loss of as much as 15 mL/day.[1] This is an area where more local data are required. Development of local phlebotomy stewardship programmes and guidelines may reduce iatrogenic blood loss due to vascular access.
Drawing a 'rainbow' of extra tubes for possible add-on blood testing has been described previously.[25] As few as 7.0% of the extra tubes are used for add-on testing.[25] This practice results not only in unnecessary blood loss, but also in additional patient discomfort, risk of biohazard exposure, use of laboratory resources and increased biohazardous waste production[26]
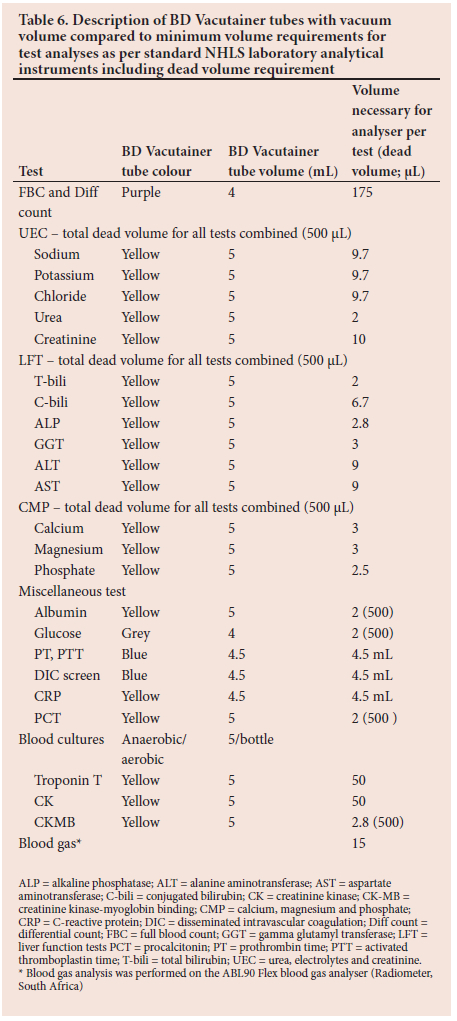
As summarised in Table 6, most laboratory tests require microlitres μL) rather than millilitres (mL) of blood to perform routine procedures. Vacuum-assisted blood volume tubes are standardised to allow 4 - 5 mL of blood. Consequently, using these standard tubes will result in 90% of the volume of blood being discarded.[27] Several options are available to reduce phlebotomy volumes. Two options are commonly available: small-volume paediatric tubes and partial draw tubes. Most automated laboratory systems are designed to use standard tubes. BD microtainer tubes are managed manually for analyses, which may add the demands of an increased workload on laboratory personnel and prolong the turnaround time.[1,11] A recent study analysed the use of small volume tubes to obtain blood for laboratory tests, and showed that they significantly reduced daily blood loss and decreased the necessity of transfusion requirement in critical care patients.[28]
Phlebotomy volume has been recommended as a quality metric in patient care.[1] Our data shows that phlebotomy volumes for routine scheduled laboratory investigations are not similar between units in a single institution. This may be due to different patient profiles or varying phlebotomy practices between units. Reducing phlebotomy volumes requires coordinated multidisciplinary collaboration within a phlebotomy stewardship programme.[1,5] In line with the principles of PBM, all decision making should be patient-centred, individualised according to the operational requirements of the unit and guided by local audit data.[29]
Study strengths and limitations
This study is novel in that it reported not only the volume of blood loss in the ICU, but also calculated the volume in excess of what is required by the laboratory to perform the necessary investigations.
One of the limitations of the study was that as standard practice, venesection samples are drawn by a professional nurse via central venous access, arterial line or a peripheral vein into a syringe. The blood is then transferred from the syringe into a sample tube. The management of blood that is drawn in excess of the sample tube requirement is determined by varying practices. In certain cases, the excess blood in the syringe is returned to the patient, whereas in other cases it is discarded. This might result in an underestimation of the blood volume drawn as only blood in the tube was analysed.
Other factors that contributed to under-reporting phlebotomy-related blood loss in this study were the exclusion of phlebotomy for blood gas analyses, specimens for blood bank cross-matching purposes for patients requiring blood or blood products, and phlebotomy for pharmacological analyses.
Conclusion and recommendations
Although the blood loss in this study was minimal compared with previously published data, it was still double the amount required to perform routine testing. The effect of the excess phlebotomy volume on participant haemoglobin and transfusion requirements were not measured . Further local studies to investigate PBM measures and outcomes of patients admitted to the ICU are required. The development of PBM guidelines for appropriate phlebotomy volumes in ICU is required. Initiatives such as 'Pause the Draws' from the Choosing Wisely campaign'291 should be incorporated into the approach of PBM in the ICU.
The following recommendations are proposed to reduce iatrogenic blood loss in the ICU: limit the volume and frequency of phlebotomy, especially in clinically stable patients,'291 reduce the performance of routine investigations and only order essential blood tests at appropriate intervals, do not order investigations that are unlikely to change the management of the patient,'291 avoid unnecessary repeat investigations, draw only the required volume of blood for tests and avoid drawing a 'rainbow' of unnecessary tubes, avoid underfilling of citrate tubes, use BD Microtainer (small-volume paediatric tubes) or partial-draw tubes where possible, improve coordination between laboratories for better use of phlebotomy samples, perform non-invasive testing where possible, increase the use of point-of-care testing, consider the use of blood conservation devices (closed blood sampling devices) and techniques, educate clinical staff, and develop and implement multidisciplinary institutional phlebotomy stewardship interventions.
Declaration. The study was performed by JCA in partial fulfilment of requirements of MMed degree (Surg).
Acknowledgements. We would like to thank personnel in all the ICUs at UAH, Prof. Gina Joubert and Mr Mpendulo Mamba at the Department of Biostatistics at the University of the Free State for statistical analyses, and Dr Daleen Struwig for technical and editorial preparation of the article.
Author contributions. JCA, CB and MS prepared the protocol and analysed data. JCA collected the data. JCA and CB wrote the first draft of the manuscript and MS critically reviewed the manuscript. All authors approved the final version of the manuscript for publication.
Funding. None
Conflicts of interest. None.
References
1. Bodley T, Chan M, Levi O, et al. Patient harm associated with serial phlebotomy and blood waste in the intensive care unit: A retrospective cohort study. PLoS One 2021;16(1):e0243782. https://doi.org/10.1371/journal.pone.0243782 [ Links ]
2. Vincent JL, Baron JF, Reinhart K, et al. Anaemia and blood transfusion in critically ill patients. JAMA 2002;288(12):1499-1507. https://doi.org/10.1001/jama.288.12.1499 [ Links ]
3. Corwin HL, Gettinger A, Pearl RG, et al. The CRIT Study: Anaemia and blood transfusion in the critically ill - current clinical practice in the United States. Crit Care Med 2004;32(1):39-52. https://doi.org/10.1097/01.ccm.0000104112.34142.79 [ Links ]
4. Athar MK, Puri N, Gerber DR. Anaemia and blood transfusions in critically ill patients. J Blood Transf 2012;2012:629204. https://doi.org/10.1155/2012/629204 [ Links ]
5. Shander A, Javidroozi M, Ozawa S, Hare GMT. What is really dangerous: Anaemia or transfusion? Br J Anaesth. 2011;107(Suppl 1):i41-i59. https://doi.org/10.1093/bja/aer350 [ Links ]
6. Vincent JL. Which carries the biggest risk: Anaemia or blood transfusion? Transfus Clin Biol 2015;22(3):148-150. https://dx.doi.org/10.1016/j.tracli.2015.05.001 [ Links ]
7. Isbister JP, Shander A, Spahn DR, Erhard J, Farmer SL, Hofmann A. Adverse blood transfusion outcomes: Establishing causation. Transfus Med Rev 2011;25(2):89-101. https://doi.org/10.1016/j.tmrv.2010.11.001 [ Links ]
8. Roubinian NH, Escobar GJ, Liu V, et al. Trends in red blood cell transfusion and 30-day mortality among hospitalised patients. Transfusion 2014;54(10 Pt 2):2678-2686. https://doi.org/10.1111/trf.12825 [ Links ]
9. Chant C, Wilson G, Friedrich JO. Anaemia, transfusion, and phlebotomy practices in critically ill patients with prolonged ICU length of stay: A cohort study. Crit Care 2006;10(5).R140. https://doi.org/10.1186/cc5054 [ Links ]
10. Harber CR, Sosnowski KJ, Hegde RM. Highly conservative phlebotomy in adult intensive care - a prospective randomised controlled trial. Anaesth Intensive Care 2006;34(4):434-437. https://doi.org/10.1177/0310057X0603400414 [ Links ]
11. Briggs EN, Hawkins DJ, Hodges AM, Monk AM. Small volume vacuum phlebotomy tubes: A controlled before-and-after study of a patient blood management initiative in an Australian adult intensive care unit. Crit Care Resusc 2019;21(4):251-257. https://ccr.cicm.org.au/file/download-article?id=1f8de85c-8374-424d-801f-70ab2b68f792&settings=litn2gC1RAsiHS43rCo4xrLtlEqu0qUr8NMbjrCw2VY%3D (accessed 20 April 2022). [ Links ]
12. Leahy MF, Hofmann A, Towler S, et al. Improved outcomes and reduced costs associated with a health-system-wide patient blood management program: A retrospective observational study in four major adult tertiary-care hospitals. Transfusion 2017;57(6):1347-1358. https://doi.org/10.1111/trf.1400617 [ Links ]
13. Meybohm P, Richards T, Isbister J, et al. Patient blood management bundles to facilitate implementation. Transfus Med Rev 2017;31(1):62-71. https://doi.org/10.1016/j.tmrv.2016.05.012 [ Links ]
14. Thomson J, Hofmann A, Barrett CA, et al. Patient blood management: A solution for South Africa. S Afr Med J 2019;109(7):471-476. https://doi.org/10.7196/SAMJ.2019.v109i7.13859 [ Links ]
15. Trudnowski RJ, Rico RC. Specific gravity of blood and plasma at 4 and 37 degrees. Clin Chem 1974;20(5):615-616. https://doi.org/10.1093/clinchem/20.5.615 [ Links ]
16. Harris PA, Taylor R, Minor BL, et al. The REDCap Consortium: Building an international community of software platform partners. J Biomed Inform 2019;95:103208. https://doi.org/10.1016/j.jbi.2019.103208 [ Links ]
17. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap) - a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform 2009;42(2):377-381. https://doi.org/10.1016/j.jbi.2008.08.010 [ Links ]
18. Holland J, Peralta RM, Moss RL, Feane K, Uprichard J. A single-centre review of iatrogenic anaemia in adult intensive care. Transfus Med 2020;30(3):196-200. https://doi.org/10.1111/tme.126740 [ Links ]
19. Thavendiranathan P, Bagai A, Ebidia A, Detsky AS, Choudhry NK. Do blood tests cause anaemia in hospitalised patients? The effect of diagnostic phlebotomy on haemoglobin and haematocrit levels. J Gen Intern Med 2005;20(6):520-524. https://doi.org/10.1111/j.1525-1497.2005.0094.x [ Links ]
20. Tosiri P, Kanitsap N, Kanitsap A. Approximate iatrogenic blood loss in medical intensive care patients and the causes of anaemia. J Med Assoc Thai 2010;93(Suppl 7):S271-S276. https://www.semanticscholar.org/paper/Approximate-iatrogenic-blood-loss-in-medical-care-Tosiri-Kanitsap/31acaaf63b8eb4234377048f07de0ba1fa11c833 (accessed 24 January 2022). [ Links ]
21. Lyon AW, Chin AC, Slotsve GA, Lyon ME. Simulation of repetitive diagnostic blood loss and onset of iatrogenic anaemia in critical care patients with a mathematical model. Comput Biol Med 2013;43(2):84-90. https://doi.org/10.1016/j.compbiomed.2012.11.008 [ Links ]
22. Yao R, Wu G, Xu L, et al. Diagnostic blood loss from phlebotomy and hospital acquired anaemia in patients with severe burns. Burns 2020;46(3):579-588. https://doi.org/10.1016/j.burns.2019.08.020 [ Links ]
23. Jackson Chornenki NL, James TE, Barty R et al. Blood loss from laboratory testing, anaemia, and red blood cell transfusion in the intensive care unit: A retrospective study. Transfusion 2020;60(2):256-261. https://doi.org/10.1111/trf.1564930 [ Links ]
24. Corwin HL, Parsonnet KC, Gettinger AG. RBC transfusion in the ICU. Is there a reason? Chest 1995;108(3):767-771. https://doi.org/10.1378/chest.108.3.767 [ Links ]
25. Humble RM, Hounkponou HG, Krasowski MD. The 'rainbow' of extra blood tubes -useful or wasteful practice? JAMA Intern Med 2017;177(1):128-129. https://doi.org/10.1001/jamainternmed.2016.6834 [ Links ]
26. Sanchez-Giron F, Alvarez-Mora F. Reduction of blood loss from laboratory testing in hospitalised adult patients using small-volume (paediatric) tubes. Arch Pathol Lab Med 2008;132(12):1916-1919. https://doi.org/10.5858/132.12.1916 [ Links ]
27. Siegal DM, Belley-Cote E, Arnold DM, et al. Small-volume tubes to reduce anaemia and transfusion (STRATUS): A pragmatic stepped wedge cluster randomised trial. Blood 2019;134(Suppl 1):3685. https://doiorg/10.1182/blood-2019-130257 [ Links ]
28. Wu Y, Spaulding AC, Borkar S, et al. Reducing blood loss by changing to small volume tubes for laboratory testing. Mayo Clin Proc Innov Qual Outcomes 2021;5(1):72-83. https://doi.org/10.1016/j.mayocpiqo.2020.08.007 [ Links ]
29. Choosing Wisely, Critical Care Societies Collaborative - Critical Care. Five things physicians and patients should question (reviewed 2021). https://www.choosingwisely.org/societies/critical-care-societies-collaborative-critical-care/ (accessed 25 January 2022). [ Links ]
 Correspondence:
Correspondence:
J C Adams
adams.jc83@gmail.com
Accepted 30 May 2022
Contribution of the study
We determined blood volume requirements for laboratory instrumentation, which allows phlebotomists to be cognisant of the true requirements for diagnostic tests to be undertaken accurately. We established diagnostic blood loss volumes in critical care units at a tertiary hospital in South Africa and we advocate for the introduction of patient blood management practice guidelines at local institutions.


{kind=link}
{kind=link}
{kind=link}