










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouthern African Journal of Critical Care (Online)
On-line version ISSN 2078-676X
Print version ISSN 1562-8264
South. Afr. j. crit. care (Online) vol.38 n.2 Pretoria Jul. 2022
http://dx.doi.org/10.7196/SAJCC.2022.v38i2.525
RESEARCH
Traumatic brain injury: Association between the Glasgow Coma Scale score and intensive care unit mortality
J J MkubwaI; A G BedadaII; T M EsterhuizenIII
IMB ChB, MSc (Clin Epi); Department of Anaesthesia and Critical Care, Princess Marina Hospital, Ministry of Health and Wellness, Gaborone, Botswana
IIMD ; Department of Surgery, Faculty of Medicine, University of Botswana, and Princess Marina Hospital, Gaborone, Botswana
IIIBSc Hons, MSc (Clin Epi); Division of Epidemiology and Biostatistics, Department of Global Health, Stellenbosch University, Cape Town, South Africa
ABSTRACT
BACKGROUND. Traumatic brain injury (TBI) prevalence in Botswana is high and this, coupled with a small population, may reduce productivity. There is no previous study in Botswana on the association between mortality from TBI and the Glasgow Coma Scale (GCS) score although global literature supports its existence.
OBJECTIVES. Our primary aim was to determine the association between the initial GCS score and the time to mortality of adults admitted with TBI at the Princess Marina Hospital, Gaborone, Botswana, between 2014 and 2019. Secondary aims were to assess the risk factors associated with time to mortality and to estimate the mortality rate from TBI.
METHODS. This was a retrospective cohort design, medical record census conducted from 1 January 2014 to 31 December 2019.
RESULTS. In total, 137 participants fulfilled the inclusion criteria, and the majority, 114 (83.2%), were male with a mean age of 34.5 years. The initial GCS score and time to mortality were associated (adjusted hazard ratio (aHR) 0.69; 95% confidence interval (CI) 0.508 - 0.947). Other factors associated with time to mortality included constricted pupil (aHR 0.12; 95% CI 0.044 - 0.344), temperature (aHR 0.82; 95% CI 0.727 - 0.929), and subdural haematoma (aHR 3.41; 95% CI 1.819 - 6.517). Most cases of TBI (74 (54%)) were due to road traffic accidents. The number of deaths was 48 (35% (95% CI 27.1% - 43.6%)), entirely due to severe TBI.
CONCLUSION. The study confirmed significant association between GCS and mortality. Males were mainly involved in TBI. These findings lack external validity because of the small sample size, and therefore a larger multicentre study is required for validation.
Keywords: Traumatic brain injury, ICU, GCSS, mortality.
Traumatic brain injury (TBI) is defined as physical injury to the head due to mechanical energy, which results in damage to brain tissue.[1,2] Worldwide, 69 million people suffer TBI annually but low- and middle-income countries have the highest incidence of road-traffic-related TBI.[1] In 2016, there were 12 941 TBI cases in Botswana. The age-standardised rate was 675 per 100 000, an increase of 16% between 1990 and 2016.[1] Therefore, the burden of TBI in Botswana is high, given a population of 2.1 million.[3] Mortality from TBI in Africa remains high as well.[4,5] For survivors, the number of years lived with disability can be high and this cost amounted to 8.1 million in 2016. Global productivity diminishes because relatively young people are involved.[6]
The three classes of TBI based on the Glasgow Coma Scale (GCS) score are: mild (13 - 15), moderate (9 - 12) and severe (3 - 8). The GCS is a standardised tool for assessing the level of consciousness, widely used since 1974.[7] It is based on three responses, namely: eye opening (4), best verbal response (5) and best motor response (6) points with maximum and minimum points of 15 and 3, respectively.[8] Similarly, coma is categorised as absent eye opening, failure to obey commands and no word verbalisations (GCS score 3 - 8 points). Patients who score <8 on the GCS are usually admitted to the intensive care unit (ICU) for management, but admission policies vary considerably between centres.[9]
The association between mortality and the GCS score has been explored extensively, including its combination with pupillary reaction to predict mortality in severe TBI with increased sensitivity.[10,11] Precise combinations of GCS for predicting mortality have been identified[12] and they contribute to the 'sum score differentially across the spectrum of consciousness'.[13] Nevertheless, a GCS of <8 predicts mortality better in TBI than non-TBI participants,[14] but a simple GCS-Age Prognosis score can predict outcomes reliably in geriatrics.[15] The length of stay (LOS) has implications on mortality as severe TBI and a space-occupying lesion prolong LOS in the ICU.[16] Observer variability may affect the reliability of the GCS but this problem may be mitigated through training, education and standardisation of assessments.[17,18] Factors associated with poor outcomes in traumatic brain injury include a low GCS score and absence of pupillary light reaction.[19]
There is a pre-hospital service provided by certified paramedics (called 997) that works in tandem with our hospital to resuscitate and transfer patients to hospital from the accident scene. After stabilisation at the accident and emergency unit, patients are subsequently transferred to the ICU, either directly or via the operating theatre. In the ICU, patients are artificially ventilated, given analgesia, sedated and monitored invasively and non-invasively. For TBI patients with raised intracranial pressure (ICP) mandatory decompressive craniectomy is done before ICU admission. The exception is lack of capacity to monitor ICP. Use of the neck collar in TBI is a standard procedure in the continuum of care.
In Botswana, TBI in the ICU has not been previously reported upon. Mortality is an outcome measure of ICU performance where critically ill patients such as those with severe TBI are managed. Since critical illness is associated with high mortality, the timing, the delivery and the type of intervention are key to ICU outcomes. Therefore, there is need for quality improvement activities that are geared towards better ICU outcomes with regard to TBI but it will be costly to implement them. This study seeks to provide preliminary knowledge regarding ICU mortality with regard to TBI.
Our primary aim was to assess the association between the admission GCS score and the time to mortality of adult patients admitted to ICU with TBI from 1 January 2014 to 31 December 2019. The secondary aims were to assess the association between selected risk factors and time to mortality over the same period, as well as to estimate the ICU mortality rate.
Methods
A retrospective cohort study was conducted at Princess Marina Hospital (PMH), Gaborone. It is the main referral and teaching hospital in Botswana with a catchment area in both northern and southern regions, and has a bed capacity of 567, including 8 ICU beds. At PMH, neurosurgery is one of the surgical subspecialties and there were three neurosurgeons at the time of the study. Children over the age of 1 month as well as adults were admitted to the ICU.
We included adults, >16 years of age, with TBI, either sedated, non-sedated or paralysed, admitted from 1 January 2014 to 31 December 2019, and excluded participants who met inclusion criteria but were transferred to other hospitals. Three research assistants extracted data from de-identified medical records.
A predefined and validated data collection tool was used to capture data from each patient record. We conducted a pilot test of the instrument before it was adopted for this study. Data entry was done by the principal investigator (PI) into an Excel (Microsoft Corp., USA) spreadsheet on a secure laptop computer. Original source documents were used to corroborate data entry. Access to this computer and a separate server was limited to the PI and authorised personnel, including a data analyst. Stata 15.1 (StataCorp., USA) was used for data analysis.
The independent variables were demographic and social factors such as age, sex, past medical history of TBI, education level and employment status. Others were TBI severity, initial GCS score, ICU LOS, and the mechanism of injury. We categorised the GCS score on admission consistent with mild, moderate or severe TBI. We also categorised pupillary size and light reaction as reactive or non-reactive, dilated or fixed and unilateral or bilateral. The outcome variables were the occurrence of death in the ICU and time to death following ICU admission.
To address the primary aim, the independent variable was GCS score, as a quantitative variable, and the outcome was time to mortality. We computed the ICU LOS as days from the admission to the exit date. A same-day admission and exit were computed as a half-day (0.5) LOS.
We used the Cox proportional hazard (PH) model to model the relationship between independent variables and time to mortality.[20] All variables which were significantly associated with time to mortality at significance level p<0.05 in univariate Cox regression analysis were entered into a multivariable Cox regression model to estimate the adjusted hazard ratios (aHR). Data were checked for the presence of multicollinearity, normality of data, and proportionality of hazards over time.[20] We set the level of statistical significance at p<0.05.
Our study relied on hospital records to capture patient data without participant contact. For this reason, we obtained a waiver for informed consent. However, patient data were safeguarded as per the data management plan. Permission was obtained from the health research ethics committee of Stellenbosch University, the Ministry of Health and Wellness (MoHW) in Botswana and the PMH ethics committee.
Results
In total, 137 participants met the inclusion criteria over the selected 6-year period. Besides the ventilated patient care bundle (includes head-up tilt, deep venous thrombosis and gastric hyperacidity prophylaxis, sedation hold and damp dusting), all patients received seizure prophylaxis, analgesia and end-tidal carbon dioxide monitoring.[21] The mean (standard deviation (SD); range) age was 34.5 (12; 18 - 88) years. Participants were predominantly male (n=114, 83.2%,), with a male to female ratio of 5:1. By GCS category, 91.2% (n=125) of the patients suffered severe TBI while 7.3% (n=10) suffered moderate TBI and 1.5% (n=2) mild TBI. The mean (SD) for the mean arterial pressure (MAP) was 87.6 (21.6) mmHg and for the initial temperature was 35.5 (2.4)°C; (95% confidence interval (CI) 35.1 - 36.0). All patients were artificially ventilated. Among the listed modes, 32.1% (n=44) of patients received the volume assist control (VAC) and 27.7% (n=38) the pressure synchronised intermittent mandatory ventilation (PSIMV) mode. All patients had a brain scan on admission to ICU; 38.7% (n=53) of participants suffered a subdural haematoma (SDH) and 27.0% (n=37) a skull base fracture. By mechanism of injury, 54.0% (n=74) of the TBIs were caused by road traffic accidents (RTAs) and 33.6% (n=46) by assault. The overall ICU mortality was 35.0% (n=48) (95% CI 27.1% - 43.6%). All deaths were attributed to severe TBI. The characteristics of study participants are shown in Table 1.

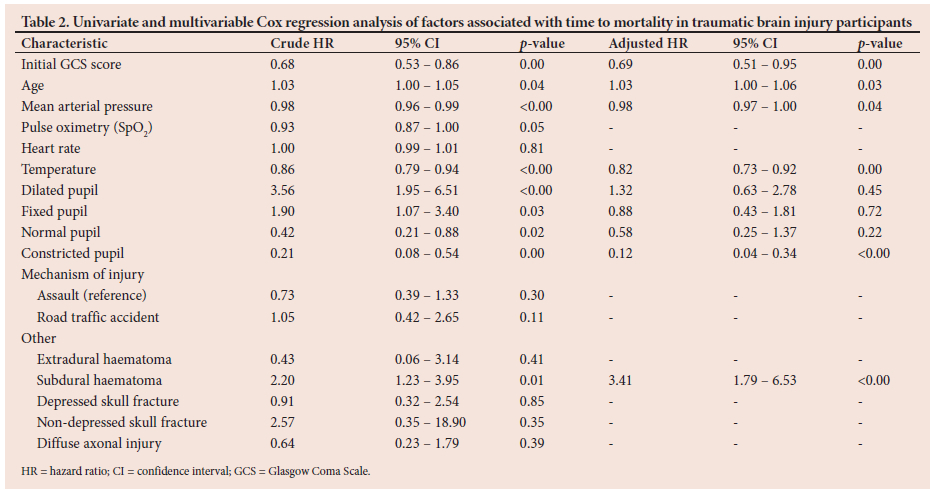
We found that the initial GCS was statistically significantly associated with time to mortality (HR 0.68; 95% CI 0.53 - 0.86; p=0.001). For every one unit increase in GCS, the hazard of mortality decreased by 32%. Other statistically significant factors in the univariate analysis included age (HR 1.03; 95% CI 1.00 - 1.05; p=0.04), MAP (HR 0.98; 95% CI 0.96 - 0.99; p<0.001), temperature (HR 0.86; 95% CI 0.791 - 0.935; p<0.00), dilated pupil (HR 3.56; 95% CI 1.945 - 6.51; p<0.00), fixed pupil (HR 1.90; 95% CI 1.07 - 3.40; p=0.03), normal pupil (HR 0.42, 95% CI 0.21 - 0.88, p=0.021), constricted pupil (HR 0.21; 95% CI 0.08 - 0.54; p=0.00) and SDH (HR 2.20; 95% CI 1.23 - 3.95; p=0.01).
Factors independently associated with time to mortality in the final multivariable model were initial GCS (aHR 0.69; 95% CI 0.51 - 0.95; p=0.00), age (aHR 1.03; 95% CI 1.001 - 1.056; p=0.04), MAP (aHR 0.98; 95% CI 0.971 - 0.998; p=0.03), constricted pupil (aHR 0.12; 95% CI 0.04 - 0.34; p<0.00), temperature (aHR 0.82; 95% CI 0.73 - 0.93; p=0.00), and SDH (HR 3.44; 95% CI 1.82 - 6.52; p<0.00). The hazard of death increased by 3% for every 1-year increase in age and increased by 3.44 times for those who had SDH. Conversely, the hazard of death decreased by 88% for those with constricted pupils and by 18% for every 1°C rise in temperature. It decreased by 2% for every mmHg rise in MAP. Table 2 shows both crude and adjusted estimates of the HRs, and their 95% CIs.
The ICU LOS varied from 0.5 to 103 days. In ascending order, the median LOS along with the corresponding 25th and 75th percentiles for the mild, moderate and severe TBI severity categories was (1.5: 0, 3), (3.5: 2, 7) and (6: 2, 19) days, respectively: however, the difference in LOS between the categories of GCS was not statistically significant (p=0.15). The overall median (interquartile range (IQR)) LOS was 6 (2 - 17) days. The mortality rate based on cumulative at-risk time of 3 999 days was 12 per 1 000 (95% CI 8.6 - 15.4) person days with a median survival time of 41 days.
Discussion
In our study, the GCS was an independent predictor of mortality in the best-fit Cox regression model. Others included SDH, constricted pupil, temperature, age and MAP. Interestingly, the HR for the GCS did not change when adjusted for the other factors associated with time to mortality. This suggests that it is a stable measurement of risk of mortality on its own, without taking the other factors into account. Although there are other scoring systems such as APACHE II as well as the increased use of machine learning approach, the GCS remains popular because of its simplicity and widespread application. The GCS, unlike the machine learning approach, does not require any equipment.[22] A review paper that reported on the early management of TBI revealed a quasi-exponential relationship with a decrease in mortality coupled with an increase in the GCS score from 3 to 8.[23] The prediction of mortality may contribute to the judicious use of intensive care resources through the application of ICU protocols, thus redirecting resources to where they are most beneficial. However, there have been arguments in support of initial aggressive management even in severe TBI because, firstly, it is difficult to predict outcome within 6 hours of presentation of TBI, and secondly, good functional outcome may be possible in some severe TBI cases.[16,24] The findings of our study are consistent with other studies in which a GCS score below 8 was associated with mortality.[25,26]-This underscores the role of GCS as a bedside clinical tool in predicting mortality that is applied in most settings.
The mean initial temperature was subnormal (35.5oC) and statistically significant (p<0.00), with an 18% reduction in the hazard of death for every 1°C increase in temperature. A recent systematic review reported positive outcomes in terms of reduced LOS and mortality in adults where fever is averted.[27] There was no use of induced hypothermia in our patients; axillary temperature was measured.
A constricted pupil demonstrated a protective effect which was statistically significant (p<0.00), with 88% reduction in the hazard of death. Other studies have reported statistically significant findings for pupillary reactivity (p=0.01) but not pupillary size.[21,M
The overall mortality in our study was 35% (n=48), with all deaths due to severe TBI. Our findings are consistent with the literature, demonstrating that the majority of deaths are due to severe TBI.[21,24,27] In our study, the mean age for TBI was 34.5 years, with 83.2% of the participants being male and the commonest mechanism of injury being RTAs at 74%. This is consistent with other studies regarding the age and mechanism of injury.[21,27] These studies also suggest that the male youth are mainly affected by TBI.
Another predictor of mortality we found to be consistent with other studies was the SDH.[20,27] In our study, the hazard of death in participants who had SDH was more than three times those who did not. The development of SDH is directly linked to a raised ICP, reduced cerebral perfusion pressure and hypoxia, leading to low GCS scores.[28-30] The HR for SDH increased by more than 50% with adjustment.
Limitations
Our study had limitations. The first is missing data, which is common in studies of this nature. We collected a data set for every participant who met inclusion criteria in the first hour of ICU admission. If the data for the first hour were missing then we extracted data for the second hour for the same participant. This was done in approximately 0.5% of the participants but it had no effect on our calculations. Our study was limited to one centre in Botswana, which implies that our findings may not be generalised to the rest of Botswana; additionally, we had a small sample size and thus the study power was diminished. This was evident in our computation of magnitudes of effect, some of which had wide CIs although they were statistically significant. We lacked data from invasive monitoring such as ICP measurements that are critical in TBI management.
Conclusion
In spite of its limitations, our study confirmed the association between GCS and mortality found in other larger studies. Some of the factors associated with mortality were found in other studies as well. Although our mortality rate does not differ markedly from other resource-limited settings in Africa, we have room for improvement. This study has demonstrated, to a limited extent, a gap in knowledge about TBI approaches in the PMH ICU. The male youth bears the burden of TBI, largely due to RTAs. A larger study is required to validate the findings in our study.
Declaration. None.
Acknowledgements. We are grateful to the PMH-ICU nurses and medical records personnel who retrieved the medical records of TBI patients.
Author contributions. JJM: study design, data collection, analysis, revision of content and accountability for entire work; AGB: revision of intellectual content; TME: study design, analysis and approval of final manuscript.
Funding. None
Conflicts of interest. None.
References
1. James SL, Theadom A, Ellenbogen RG, et al. Global, regional, and national burden of traumatic brain injury and spinal cord injury, 1990-2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol 2019;18(1):56-87. https://doi.org/10.1016/S1474-4422(88)30415-0 [ Links ]
2. Menon DK, Schwab K, Wright DW, et al. Position Statement: Definition of Traumatic Brain Injury Arch Phys Med Rehabil 2010;91(11):1637-1640. https://doi.org/10.1016/j.apmr.2010.05.17. [ Links ]
3. Statistics Botswana. Population and Housing Census 2011- Population of towns villages and associated localities, Gaborone. Statistics Botswana, 2011. https://www.statsbots.org.bw/sites/default/files/publications/ Population%20and%20Housing%20Census%202011%20%20Dissemination%20seminar%20report.pdf (accessed 9 August 2019). [ Links ]
4. Opondo EA, Mwangombe NJM. Outcome of severe traumatic brain injury at a critical care unit: A review of 87 patients. Ann Afr Surg 2007;1: 3-9. https://doi.org/10.4314/aas.v1i1.45788. [ Links ]
5. Dewan MC, Rattan A, Gupta S, et al. Estimating the global incidence of traumatic brain injury. J Neurosurg 2018;130(4):1080-1097. https://doi.org/10.3171/2017.10.JNS17352. [ Links ]
6. Teasdale G, Jennett B. Assessment of coma and impaired consciousness. Lancet 1974,-304(7872), 81-84. https://doi.org/10.1016/s0140-6736(74)91639-0. [ Links ]
7. Advances in Clinical Neuroscience and Rehabilitation. ACNR, 2013-Classification of Traumatic Brain Injury. Wiltshire BA12 6DQ. https://acnr.co.uk/articles/classification-of-traumatic-brain-injury/?hilite=headache (accessed 9 August 2019). [ Links ]
8. Volovici V, Ercole A, Citerio G, et al. Intensive care admission criteria for traumatic brain injury patients across Europe. J Crit Care 2019;49:158-161. https://doi.org/10.1016/j.jcrc.2018.11.002. [ Links ]
9. Brennan PM, Murray GD, Teasdale M. Simplifying the use of prognostic information in traumatic brain injury. Part 1: The GCS-Pupils score: An extended index of clinical severity. J Neurosurg 2018;128:1612-1620. https://doi.org/10.3171/2017.12.JNS172780. [ Links ]
10. Kung W-M, Tsai S-H, Chiu W-T, et al. Correlation between Glasgow coma score components and survival in patients with traumatic brain injury. Int J Care Injured 2011;42:940-944. https://doi.org/10.1016/j.injury.2010.09.019. [ Links ]
11. Reith FC, Lingsma HF, Gabbe BJ, et al. Diffrential effects of the Glasgow coma scale score and its components: Analysis of 54,069 patients with traumatic brain injury. Injury 2017;48:1932-1943. https://doi.org/10.1016/j.injury.2017.05.038 [ Links ]
12. Osler T, Cook A, Glance LG, et al. Differential mortality of Glagow coma score in patients with and without head injury. Injury 2016;47:1879-1885. https://doi.org/10.1016/j.injury.2016.04.016 [ Links ]
13. Khan M, O'Keeffe T, Jehan F, et al. The impact of Glasgow Coma Scale-Age Prognosis Score on geriatric traumatic brain injury outcomes. J Surg Res 2017;216:109-114. https://doi.org/10.1016/j.jss.2017.04.026 [ Links ]
14. Lazaridis C, Yang M, DeSantis SM, et al. Predictors of intensive care unit length of stay and intracranial pressure in traumatic brain injury. J Crit Care 2015,30(6):1258-1262. https://doi.org/10.1016/j.jcrc.2015.08.003 [ Links ]
15. Teasdale G, Knill-Jones R, van der Sande J. Observer variability in assessing impaired consciousness and coma. J Neurol Neurosurg Psychiatry 1978;41(7):603-610. https://doi.org/10.1136/jnnp.41.7.603 [ Links ]
16. Waxman K, Sundine MJ, Yang RF. Is early prediction of outcome in severe head injury possible? Arch Surg 1991;126(10):1237-1242. https://doi.org/10.1001/archsurg.1991.01410340079011. [ Links ]
17. Reith FCM, van den Brande R, Synnot A, et al. Reliability of the Glagow Coma Scale: A systematic review. Intensive Care Med 2016:42(1):3-15. https://doi.org/10.1007/s00134-015-4124-3 [ Links ]
18. Reith FCM, Synnot A, van den Brande R, et al. Factors affecting the reliability of the Glagow Coma Scale: A systematic review. Neurosurgery 2017;80(6):829-839. https://doi.org/10.1093/neuros/nyw178. [ Links ]
19. Kim Y-J. A systematic review of factors contributing to outcomes in patients with traumatic brain injury. J Clin Nurs 2011;20(11-12):1518-1539. https://doi.org/10.1111/j.1365-2702.2010.0368.x. [ Links ]
20. Abeysekera WWM, Sooriyarachchi MR. Use of Schoenfeld's global test to test the proportional assumption in the Cox proportional hazards model: An application to a clinical study J Nat Sci Foundation Sri Lanka 2009;37(1):41-51. https://doi.org/10.4038/jnsfsr.v37i1.456. [ Links ]
21. Brain Trauma Foundation. Brain Trauma Foundation Guidelines 2016. Guidelines for the Management of Severe TBI, 4th ed. New York: BTF, 2016. http://braintrauma.org/guidelines/guidelines-for-the-management-of-severe-tbi-4th-ed#-ventilation-therapies (accessed 13 April 2021). [ Links ]
22. Abujaber A, Fadlalla A, Gammoh D, et al. Prediction of in-hospital mortality in patients with post traumatic brain injury using National Trauma Registry and Machine Learning Approach. Scand J Trauma Resusc Emerg Med 2020;28:44. https://doi.org/10.1186/s13049-020-00738-5. [ Links ]
23. Moppett IK. Traumatic brain injury: assessment, resuscitation and early management. Br J Anaesth 2007;99(1):18-31. https://doi.org/10.1093/bja/aem128. [ Links ]
24. Chamoun RB, Robertson CS, Gopinath SP. Outcome in patients with blunt head trauma and a Glasgow Coma Scale score of 3 at presentation. J Neurosurg 2009;111(4):683-687. https://doi.org/10.3171/2009.2.JNS08817 [ Links ]
25. Okidi R, Ogwang DM, Okello TR, et al. Factors affecting mortality after traumatic brain injury in aresource-poor setting. BJS Open 2020;4(2):320-325. https://doi.org/10.1002/bjs5.50243. [ Links ]
26. Almutawa E, Al Balooshi AM, Ghanem S. Factors affecting mortality in severe traumatic brain injury. Bahrain Medical Bulletin 2017;39(2):96-99. [ Links ]
27. Madden LK, DeVon HA. Sytematic review of the effects of body temperature on outcome following adult traumatic brain injury. J Neurosci Nurs 2015;47(4):190-203. https://doi.org/10.1097/JNN.0000000000000142 [ Links ]
28. Ozyurt E, Goksu E, Cengiz M, et al. Retrospective analysis of prognostic factors of severe traumatic brain injury in a university hospital in Turkey. Turk Neurosurg 2015;25(6):877-882. https://doi.org/10.5137/1019-5149.JTN.9181-13.0 [ Links ]
29. Han M-H, Ryu JI, Kim CH, et al. Radiolological findings and patient factors associated with 30-day mortality after surgical evacuation of subdural haematoma in patients less than 65 years old. J Korean Neurosurg Soc 2017;60(2):239-249. https://doi.org/10.3340/jkns.2016.0404.009 [ Links ]
30. Shin D-S, Hwang S-C. Neurocritical management of acute subdural haematomas. Korean J Neurotrauma 2020;16(2):113-125. https://doi.org/10.13004/kjnt.2020.16.e43. [ Links ]
 Correspondence:
Correspondence:
J J Mkubwa
mkubwajack1@gmail.com
Accepted 2 May 2022
Contribution of the study
This study informs the relevant stakeholders in Botswana about sociodemographics, clinical characteristics, management and outcomes of patients admitted to the ICU with severe TBI on the backdrop of scarce ICU resources. It provides a basis for a larger study to inform its external validation.


{kind=link}