










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouthern African Journal of Critical Care (Online)
versión On-line ISSN 2078-676X
versión impresa ISSN 1562-8264
South. Afr. j. crit. care (Online) vol.36 no.1 Pretoria ene./jul. 2020
http://dx.doi.org/10.7196/sajcc.2020.v36i1.410
ARTICLE
Perceived barriers to the development of the antimicrobial stewardship role of the nurse in intensive care: Views of healthcare professionals
J RoutI; P BrysiewiczII
IMN; School of Nursing and Public Health, College of Health Sciences, University of KwaZulu-Natal, Durban, South Africa
IIPhD; OrcID 0000-0001-6258-1603; School of Nursing and Public Health, College of Health Sciences, University of KwaZulu-Natal, Durban, South Africa
ABSTRACT
BACKGROUND: Antimicrobial stewardship has become an important initiative within intensive care units in the global fight against antimicrobial resistance. Support for nurses to participate in and actively direct antimicrobial stewardship interventions is growing however, there may be barriers that impede the development of this nursing role
OBJECTIVES: To explore the views of healthcare professionals regarding barriers to the antimicrobial stewardship role of the nurse in intensive care in a private hospital in KwaZulu-Natal, South Africa
METHODS: Using a qualitative research approach, purposive sampling was used to identify fifteen participants from the disciplines of nursing, surgery, anaesthetics, internal medicine, microbiology, and pharmacy in a general intensive care unit. Content analysis was used to code data obtained from each individual interview
RESULTS: The following categories and subcategories were derived: regarding barriers to the role of the nurse in antimicrobial stewardship: (i) lack of collaboration (subcategories: not participating in the antimicrobial stewardship programme, no feedback about antimicrobial resistance in the unit, and not part of decision-making); (ii) inadequate knowledge (subcategories: not understanding infection prevention and control, missing the link between laboratory results and start of treatment, and poor knowledge of antibiotics and their administration); and (iii) inexperienced nurses (subcategories: shortage of intensive care nurses, lack of experienced nurses, and inadequate nursing staff to provide in-service training
CONCLUSION: The nursing role within antimicrobial stewardship was negatively affected by both staffing and collaborative difficulties, which impacted on the implementation of antimicrobial stewardship within the unit
Keywords: antimicrobial stewardship; barriers; nurse role.
Antimicrobial stewardship (AMS) is now accepted practice in hospitals, particularly within high-risk areas such as the intensive care unit (ICU) where infection rate and antimicrobial use are predictably higher than the rest of the hospital.[1] In order to effectively address the dual challenges of inappropriate antimicrobial prescription and antimicrobial resistance (AMR), it is necessary for all members of the multidisciplinary team to fully participate within AMS programmes.[2,3] Core AMS strategies appear to be directed towards the function of medical staff;[4] however this does not preclude the complementary role that nursing interventions can play in AMS such as prescriber 'prompting' during treatment choice, ensuring that appropriate cultures are taken prior to commencement of treatment, and using culture and antibiogram results to advocate for de-escalation.[5-8] Nurses possess a vast amount of clinical and microbiological information about the patients in their care and about trends of antimicrobial use in the ICU, and therefore have the potential to influence decision-making within AMS.[9] The nursing role within AMS has been largely relegated to the care of the infection prevention and control (IPC) nurse specialist,[2] but recent studies have extended this role to that of the non-specialist nurse.[3,5,7,10-12] The nonspecialist nursing role is recognised as essential in the co-ordination of patient care in AMR and AMS,[7] and is identified in the ICU as both clinical and advocatory.[11] It is therefore important that the hospital nurse at 'point of care' should be supported to take an active role in this initiative.
Objective
To explore the views of healthcare professionals regarding barriers to the AMS role of the nurse in intensive care.
Methods
This is part of a larger study exploring the role of the ICU nurse in AMS,[11] in which a qualitative descriptive research approach, using content analysis, was adopted.[13]
Setting
This study was conducted in a 20-bed adult ICU/high-care unit in a 200-bed private hospital in KwaZulu-Natal, South Africa (SA), which admits medical and surgical patients managed by non-intensivists.
Participants
Purposive sampling was used to identify participants from nurses and other healthcare professionals/other members of the multidisciplinary team (Table 1) who met the inclusion criteria and were interested to participate in the study.[14] Nursing participants included two nurses from hospital management who had set up the AMS programme two years previously, and six clinical ICU nurses whose responsibilities as shift leaders included daily AMS rounds. These were registered professional nurses; one held an additional qualification as an ICU nurse, the remaining five had experience of working in this area of nursing but held no specialist qualification. Non-nursing participants included a microbiologist, pharmacist, two anaesthetists, two physicians and two surgeons. The microbiologist was representative of one of the private laboratories that served the study hospital and the pharmacist was a representative from the hospital pharmacy. The clinicians were specialists who had admission rights in the ICU.
Ethical approval
Approval was granted by the ethics committee of the University of KwaZulu-Natal (ref. no. BE281/14), and hospital management. Participants were invited to take part in the study, were informed of the purpose of the study and the right to withdraw at any stage of the study. Written consent was obtained, and confidentiality maintained.
Data collection and analysis
Individual semi-structured individual interviews with all participants were held in a private room in the hospital during on-duty time, as agreed by hospital management. Interviews were conducted with nursing participants during routine break times, and with non-nursing participants at times that were determined convenient to them. All interviews were conducted by the principal investigator (JR) who worked in the unit as a clinical nurse. All interviews were digitally recorded with participant consent and knowledge. Interviews were transcribed verbatim and were read and reread in a process of submersion. Manifest content analysis [13] was used to identify categories arising from the data, guided by the purpose of the study and together with an experienced qualitative researcher. A process of interpretation was carried out by familiarisation with the text, examining each participant's contribution, and paraphrasing and condensing the content of the text to determine codes and categories. This was then checked by a co-coder to verify the accuracy of the coding (Table 2). Rigour was assured by adherence to the principles of trustworthiness (credibility, transferability, dependability, and confirmability) during the preparation, organisation and reporting phases of the study.[15]
Results
Nursing and non-nursing participants, comprised of clinical and management nurses, anaesthetists, physicians, surgeons, and a microbiologist and pharmacist, identified the following three categories regarding barriers to the role of the nurse in AMS. These were: (i) lack of collaboration (subcategories: not participating in the AMS programme, no feedback about AMR in the unit, and not part of decision-making); (ii) inadequate knowledge (subcategories: not understanding IPC, missing the link between laboratory results and start of treatment, and inadequate knowledge of antibiotics and their administration) and; (iii) inexperienced nurses (subcategories: shortage of ICU nurses, lack of experienced nurses, and inadequate nursing staff to provide in-service training). Contributions from both nursing (N) and non-nursing participants (NN) are provided to illustrate the categories and subcategories. Strategies were also suggested by the participants in order to develop the nurses' role in AMS and to address these barriers (Table 3).
Lack of collaboration
Nursing management started the AMS programme in this ICU soon after the hospital opened, following prompting by one of the private laboratories regarding global concerns of rising levels of bacterial resistance. The participants (both nursing and non-nursing) suggested a lack of collaboration, within the ICU multidisciplinary team, impacted negatively on the growth of this programme.
(i) Not participating in the AMS programme: Weekly telecommunication was arranged by nursing management with the microbiologists from the private laboratory that had helped to set up the programme; however nursing shift leaders and bedside nurses were not included in these meetings. Although they were invited, these scheduled meetings were not supported by doctors or the pharmacist. The participants explained: 'We tried initially to get the doctors on board to actually form part of our team and to join our meetings. They don't seem to be very interested..! (Nl); 'The pharmacist is not actively involved in the programme. I have been told that it is not happening... because the pharmacy is too busy... (N7). A non-nursing participant suggested: 'The problem is still the doctor and physician buy-in culture in South Africa (NN5).
(ii) No feedback about AMR in the unit: The clinical nurse participants reported that as shift leaders they had limited involvement within the AMS programme and did not receive feedback from the various aspects of the initiative. A participant explained: 'There's not much feedback... not that I'm aware of... that I've ever had back... and I have been involved in doing those rounds, but I haven't had any feedback! (N4). A non-nursing participant was also concerned that there was very little feedback from nursing management about AMR and the progress of the AMS initiative in the unit: You see, there is no feedback on that to us as clinicians... which is crazy. You know, it's all very well having these meetings but, I think, it is always good to get feedback to your clinicians, you know. Find out what bacteria are being cultured... I think it's important that we know about these things because otherwise we are all working in isolation' (NN6).
(iii) Not part of decision-making: Nursing participants said that doctors in the unit tended not to listen to them when offering opinions on treatment choices and thus they felt excluded from decisions made about treatment: 'There are the odd doctors who might say "what do you think?" or "how do you feel about this", or "what else can we do" ... but not very often. No, not often at all' (N4); 'Like a doctor, if asked... just asked... that "maybe you should considering putting the patient on this antifungal as... as opposed to that antifungal" and he would say "no, just leave it such" and the next day he will come and then change it to your suggestion (N7). Nurses complained that some doctors showed dismissive behaviour in interactions with the bedside nurses. Participants further explained: You know the attitude... I'm the doctor... and if I say it's got to be done, it's got to be done' (N2); 'You know the doctors think I am just a nurse... just sometimes (someone) to carry out orders..' (N5).
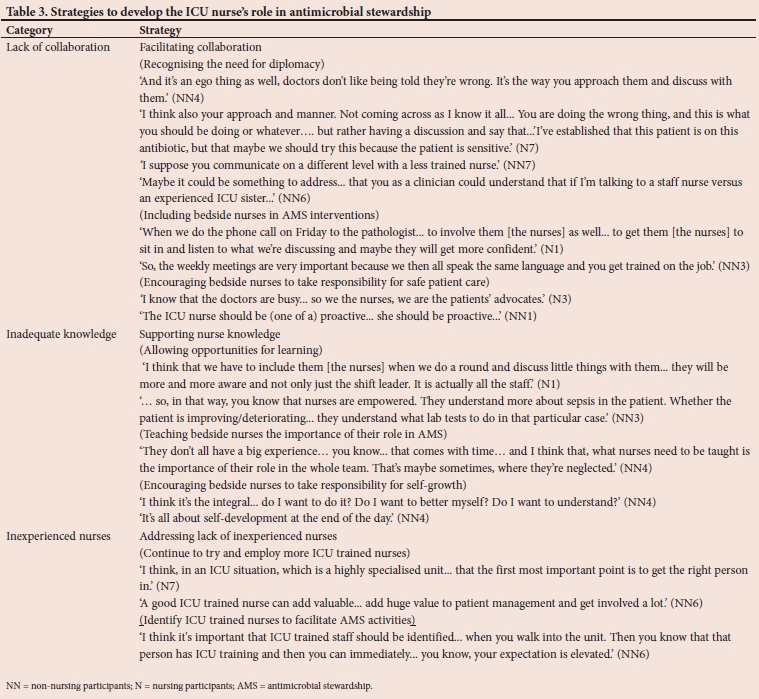
(iv) Strategies to facilitate collaboration: Participants suggested that development of the nurses' role in AMS in this ICU, regarding collaboration, could be developed by: recognising the need for diplomacy; including bedside nurses in AMS interventions; and by encouraging bedside nurses to take responsibility for safe patient care. No recommendations were made for ways to facilitate feedback about progress with the AMS programme to the multidisciplinary team, or to improve doctor and pharmacist support for AMS in the unit (Table 3).
Inadequate knowledge
The participants suggested that there are deficiencies in nurse training and education in SA, and this has impacted on the goals of AMS.
(i) Not understanding IPC: Inadequate basic nursing knowledge was felt to have contributed towards poor understanding of IPC and the role that this plays in AMR. A participant said, 'I think like when you first come to work (in the mornings), I don't see many people washing hands.' (N6). A non-nursing participant felt that patients admitted to ICU were at risk of severe infections due to exposure to the ICU environment, with the increased risk of cross infection: 'If I have someone in an ICU, that's there for longer than a week. The kind of infection that I expect is a very resistant bug which puts me immediately in the class of carbapenems, as a result.' (NN2).
(ii) Missing the link between laboratory results and start of treatment: Non-nursing participants suggested that nurses' reluctance to take the initiative, poor organisational ability in documentation and filing, and poor communication skills, led to delays in them receiving timely information regarding important antibiograms. This then impacted critical adjustment of antimicrobial therapy: 'Basically, to beg them (the nurse) to get the information. "Is anything back?" "Well I don't know" ... and this and that... and you have to go and dig through the whole file to see if there's anything new' (NN7). A participant said: 'You send off the specimen... you know it's pointless if you are not going to look at the results' (NN6). This was a source of frustration for both groups of participants who attributed delayed treatment changes to inadequate nurse training and disinterest. Participants said: 'If I (the nurse) file this thing, I (the doctor) am only going to see it tomorrow morning... think... think... (what) ICU is about... think!' (NN4); 'Just punch them (the results) and put them in the file. So, it doesn't always get looked at and then... some days down the line... you'll look, and doctor will ask "has anything been cultured on this?'"... and only when you go and look there and you find... oh... this, this and that has been cultured. but no one has said anything about it' (N3)
(iii) Poor knowledge of antibiotics and their administration: Both nursing and non-nursing participants stated that nurses need to understand not only how to mix antimicrobial treatment correctly but also how to administer it effectively: Obviously, each drug has its own mixing... you play an important role... if something has to be mixed with saline and it gets dex (dextrose) water. you know, it's stuffed. it's not going to work... ' (NN4); 'But their (the nurses) role is to understand... that, I'm giving Meronem... What, and how it is reconstituted, how it is given?' (NN4). Adherence to the correct timing was considered to be the most important part of administration of the antibiotic. A participant explained: 'Making sure that the frequency... the dose interval is done correctly... And it is strict 8 hourly, 12 hourly or whatever. The prescribed time, that is very important in stewardship also because you can create resistance by not carrying out your frequency correctly' (N2). Reference was also made by the participants to the administration of antibiotics by extended infusions. A participant said: 'Certain antibiotics you have to give regularly, and certain ones you have to give over a prolonged period... so, the nurses' function is to make sure that the correct antibiotic has been given, and it has been correctly given' (NN5). A nursing participant suggested that piggy backing the antibiotic onto the IV-fluid line allowed the nurse to flush the line, to ensure that the complete dose of antibiotic was delivered to the patient, but she said: 'I don't know why people give it as the whole individual line. But they do... a lot. I often find that with... especially the ICU patients that I'm looking after... then I'll come and there will be another IV medication line when actually there's a fluid, and you can just piggyback... like piggy back your little antibiotic on your add-a-line and it's done the job in the same amount of time and you can even actually fill... refill your line with some of the fluid from your maintenance and run it' (N4). The lack of a pharmacist presence in the AMS programme had been identified by the nursing participants as being a problem; however, it was not reported that it was common practice to phone pharmacy for clarity on prescribed orders, or advice on the correct administration of treatment: '.we're lacking in certain areas. Like, for example the pharmacy input... the pharmacists' input..' (N7).
(iv) Strategies to support nurse knowledge: Participants suggested that the development of the nurses' role in AMS, regarding supporting knowledge, could be facilitated by allowing opportunities for learning; teaching bedside nurses the importance their role in AMS and encouraging bedside nurses to take responsibility for self-growth (self-development) (Table 3).
Inexperienced nurses
Both nursing and non-nursing participants expressed concern about the shortage of ICU trained nurses in SA and the lack of ICU experienced nurses, resulting in the unit being mainly staffed with generalist nurses and non-registered nurses. The lack of skilled nurses was felt to impact on the general functioning of the ICU, and on senior-to-junior nurse guidance in the AMS programme.
( i) Shortage of ICU nurses: A nursing participant was concerned about employing nurses who are not competent to nurse critically ill patients: 'And I understand, and I know that there is a shortage of (ICU trained) nursing staff in the... countrywide, worldwide, it is a shortage. But, you know, you're left in such a tight spot or a difficult situation when you just employ a body' (N7). A non-nursing participant reported that the lack of trained ICU nurses impacted on doctor expectations of nursing staff: 'I don't even know how many of these nurses, that I work with in ICU, are actually properly ICU trained? So therefore, I suppose, my expectation is not particularly high... I don't expect very much' (NN6).
(ii) Lack of experienced nurses: Participants were concerned about the lack of skilled nursing staff in the unit. Participants explained: 'I think that the problems in the private sector... and I don't know what it's like in the province... Certainly in the private sector, we have a lot of inexperienced nurses' (NN6); 'We are using a lot more staff that don't have the correct level of experience to be in an ICU. It's just a sign of the times' (N2). Non-nursing participants were concerned that the use of non-registered nurses in the ICU meant that their patients would not receive adequate care, as these nurses did not have the capability to participate in AMS: 'Can't just assume an enrolled nurse will know what an MC&S is... How are they going to know about a MC&S and bugs and antibiotics and stuff? I mean... it's ridiculous' (NN7).
The participants went on further to say that placement in an acute care unit such as ICU without the necessary training and skills may affect nurse attitude. A participant said: 'I can see them in ICU... I can see those that are there, and want to be there, and want to do the best for the patients... and I can see those who don't... and we have got lots of those...' (NN4).
( iii) Inadequate nursing staffing to provide in-service training: Nursing participants said that the unit was often too busy to provide in-service training on AMR and AMS, and that nurses as a result often did not have the opportunity to learn necessary skills. A participant explained: 'You try and do it while everybody is on duty and then the phone is ringing and doctors are coming and the patient's unstable, ... so it is difficult to get them all together' (N1).
( iv) Strategies to address the lack of experienced nurses: The participants suggested strategies to address the barrier of inexperienced nurses, and these included: to continue to employ ICU trained nurses and to identify ICU trained nurses working in this ICU in order to facilitate communication between members of the AMS team. No recommendations were suggested by either the nursing or non-nursing participants to facilitate in-service training in AMS (Table 3).
Discussion
The successful implementation of a new AMS programme within a hospital requires 'buy-in' from doctors, and is more likely to be achieved if they are involved in the AMS programme from the start.[16] Many ICUs in the private healthcare sector in SA are not managed by intensivists but by independent specialists with autonomous practice, resulting in what is known as 'open units'.[17] The dynamics of an 'open unit' are that doctors are generally not based within the ICU itself but in 'rooms' within the hospital, and multidisciplinary 'ward' rounds in ICUs with discussions regarding shared patient treatment are not common practice.[18] Regular formal meetings are essential to provide an opportunity for the pharmacist [16] and microbiologist to meet with the doctors and participate in decision-making regarding the general management of antibiotics within the ICU, use of generic antimicrobial medicines, optimal management of resistant pathogens of individual patients, and for audit feedback. Importantly, this also allows the ICU unit manager, ICU shift nurses, and the IPC nurse specialist a platform to discuss concerns regarding antibiotic choices, ongoing management of infection control within the unit, optimal nurse/patient allocations, and forward planning for in-service AMS teaching for nurses in the ICU.[5,7,19] Both nursing and non-nursing participants in the current study felt that there was a need for diplomacy in interactions between nurses and doctors, and that including nurses in AMS interventions would assist in encouraging the bedside nurse to take an interest in the AMS initiative. No recommendations were made by participants to improve doctor and pharmacist participation within the AMS program.
The responsibilities of the ICU nurse within an AMS programme are organisation of the programme itself in accordance with evidence-based AMS principles, advocacy of patient care with respect to optimal antimicrobial therapy, timely identification of changes in the patient's clinical condition, and communication of any changes to other members of the AMS team.[11] This is almost impossible if nursing staff are unable to fully comprehend the consequences of AMR, or cannot fully participate in AMS strategies. Improving nurse awareness of antimicrobial use and the impact of antibiotic therapy on infection outcomes contributes to the goals of AMS.[2] Participants' concerns in the current study regarding basic safety measures such as handwashing suggest that nurses within the unit are either not aware of the consequences of non-compliance with best practice,[20] or are aware, but too busy or possibly even unwilling to follow IPC guidelines. This should not be overlooked, as hand hygiene is globally recognised as the foundation of universal standard IPC precautions.[21] Not understanding, or missing important laboratory information can lead to adverse events.[22] If the bedside nurse does not have the competence to recognise a newly identified pathogen in microbiology laboratory reports, and does not understand the significance of this with regard to the management of the ill patient, this may not be brought to the doctor's attention. Similarly, should the nurse not understand the challenges of antimicrobial resistance, or know and understand current antimicrobial guidelines, the significance of a particular prescription may be missed. This raises concerns about medication safety[23] and the correct administration of antimicrobial medicines. [24] Nursing leadership, both in the specialist role of the nurse manager and in the senior-junior bedside nurse relationship, is vitally important in ensuring an environment that allows opportunities for learning,[25] both to support the development of the ICU nurse's role within AMS and for the development of general nursing knowledge and skills. Participants in the current study suggest that the bedside nurse needs to be made aware of the importance of the AMS role, and that it is important to cultivate and support nursing interest and commitment to AMS.
High bed occupancy and patient turnover in the private healthcare sector, exacerbated by the shortage of appropriately trained nursing workforce,[17] has created an almost untenable nurse workload.[18,25] The practice of using generalist nurses in ICUs in the private healthcare sector has become commonplace in SA,[17] as has the use of nonprofessional nurses to care for patients with lower acuity scoring in the ICU.[26] Providing 'on the job' training becomes even more important when inexperienced and untrained nurses are used to care for patients in ICU. Time constraints within a busy unit affect additional duties such as AMS;[2] therefore ensuring adequate staffing is crucial to provide for the provision of in-service training in such programmes. The global literature clearly documents the link of sub-optimal staffing with increased morbidity and mortality from infection,[27,28] and should be acknowledged by hospital and nursing management as a major contributing factor to hospital-acquired infections and microbial resistance.[29] Allowing opportunities for in-service education shows a willingness to invest in nursing resources,[2] and underscores the message that the institution wishes to deliver with regard to controlling AMR in the ICU. The provision of on-going training supports the principles of professional nursing practice where it is expected that requisite knowledge, skills and competencies are maintained by an individual, and supported by the healthcare organisation.[30]
Recommendations
It is essential that hospital and nursing management ensure that sufficient numbers of appropriately trained nursing staff are placed in specialised acute care areas such as the ICU in order to provide supervision and guidance to generalist and enrolled nurses, with regard to both general nursing care and AMS concepts and duties. Allocation of nurses to individual patients within the ICU should be carried out with consideration to matching nurse competencies to patient acuity and needs. Every provision should be made by hospital and nursing management to provide an environment which ensures nurse education and patient safety. Research needs to be carried out into ICU nurse attitudes and performance in order identify appropriate training for personal skills such as organisational and communicative 'soft' skills. Healthcare professionals of all disciplines should have exposure to interdisciplinary AMR and AMS education at various stages of undergraduate education to promote respect and collegiality and improve collaborative efforts.
Study limitations
This study was conducted in a single setting, namely a new private hospital; thus these findings are contextual and specific to the setting. Interviews were held during tea/lunch breaks resulting in participant concerns about needing to return to the unit. The researcher was known to all participants; however, this was found to facilitate ease of the interview, and participant contributions were perceived by JR to be honest opinions.
Conclusion
The successful implementation of an AMS programme requires the 'buy-in' of all healthcare professionals. This is especially important in acute areas such as the ICU which faces unprecedented rates of AMR. Effective AMS requires knowledgeable bedside nurses who understand AMS goals and can support AMS strategies. Hospital management must ensure adequate staffing in ICUs to allow opportunities for nurse education, in order for bedside nurses to participate actively and effectively in AMS.
Declaration. None.
Acknowledgements. We wish to acknowledge Dr J de Beer for her assistance in conceptualising the study.
Author contributions. JR collected the data, JR and PB analysed the data, drafted the manuscript and approved it for submission.
Funding. None.
Conflicts of interest. None.
References
1. Kaki R, Elligsen M, Walker S, Simor A, Palmay L, Daneman N. Impact of antimicrobial stewardship in critical care: A systematic review. J Antimicrob Chemoth 2011;66(6):1223-1230. https://doi.org/10.1093/jac/dkr137 [ Links ]
2. Edwards R, Drumright L, Kiernan M, Holmes A. Covering more territory to fight resistance: Considering nurses' role in antimicrobial stewardship. J Infect Prevent 2011;12(1):6-19. https://doi.org/10.1177%2F1757177410389627 [ Links ]
3. Canadian Nurses Association. Antimicrobial resistance in Canada: Brief for the Standing Committee on Health, 2017. https://www.cna-aiic.ca/~/media/cna/page-content/pdf-en/antimicrobial-resistance-in-canada-brief-for-the-standing-committee-on-health.pdf?la=en (accessed March 2019). [ Links ]
4. Barlam T, Cosgrove S, Abbo L, et al. Implementing an antibiotic stewardship program: Guidelines by the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America. Clin Infect Dis 2016;62(10):e51-e77. https://doi.org/10.1093/cid/ciw118 [ Links ]
5. American Association of Nurses. White Paper. Redefining the antibiotic stewardship team: Recommendations from the American Nurses Association/Centers for Disease Control and prevention workgroup on the role of registered nurses in hospital antibiotic stewardship practices, 2017. http://www.nursingworld.org/ANA-CDC-AntibioticStewardship-WhitePaper (accessed December 2018). [ Links ]
6. Olans RD, Olans RN, Witt D. Good nursing is good antibiotic stewardship. Am J Nurs 2017;117(8):58-63. https://doi.org/10.1097/01.NAJ.0000521974.76835.e0 [ Links ]
7. Australian Commission on Safety and Quality in Health Care. Antimicrobial stewardship in Australian health care, 2018. https://www.safetyandquality.gov.au/our-work/healthcare-associated-infection/antimicrobial-stewardship/book/ (accessed December 2018). [ Links ]
8. Carter E, Greendyke W, Furuya Y, et al. Exploring the nurses' role in antibiotic stewardship: A multisite qualitative study of nurses and infection preventionists. Am J Infect Control 2018;46(5):492-497. https://doi.org/10.1016/j.ajic.2017.12.016 [ Links ]
9. Charani E, Castro-Sanchez E, Holmes A. The role of behaviour change in antimicrobial stewardship. Infect Dis Clin North Am 2014;28(2):169-175. https://doi.org/10.1016/j.idc.2014.01.004 [ Links ]
10. Brink A, van den Bergh D, Mendelson M, Richards G. Passing the baton to pharmacists and nurses: New models of antibiotic stewardship for South Africa? S Afr Med J 2016;106(10):947-948. https://doi.org/10.7196/SAMJ.2016.v106i10.11448 [ Links ]
11. Rout J, Brysiewicz P. Exploring the role of the ICU nurse in the antimicrobial stewardship team at a private hospital in KwaZulu-Natal, South Africa. South Afr J Crit Care 2017;33(2):46-50. https://doi.org/10.7196/SAJCC.2017.v33i2.331 [ Links ]
12. Sumner S, Forsyth S, Collette-Merrill K, et al. Antibiotic stewardship: The role of clinical nurses and nurse educators. Nurse Educ Today 2018;60:157-160. https://doi.org/10.1016/j.nedt.2017.10.011 [ Links ]
13. Erlingsson C, Brysiewicz P. A hands-on guide to doing content analysis. Afr J Emerg Med 2017;7(3):93-99. https://doi.org/10.1016/j.afem.2017.08.001 [ Links ]
14. Erlingsson C, Brysiewicz P. Orientation among multiple truths: An introduction to qualitative research. Afr J Emerg Med 2012;3(2):92-99. https://doi.org/10.1016/j.afjem.2012.04.005 [ Links ]
15. Lincoln S, Guba E. Naturalistic inquiry. In: Pearson E. The Handbook of Social Work Research Methods. Thousand Oaks: Sage, 1985:416. [ Links ]
16. Cotta M, Robertson M, Marshall C, Thursky K, Liew D, Buising K. Implementing antimicrobial stewardship in the Australian private hospital system: A qualitative study. Aust Health Rev 2015;39(3):315-322. https://doi.org/10.1071/AH14111 [ Links ]
17. De Beer J, Brysiewicz P, Bhengu B. Intensive care nursing in South Africa. South Afr J Crit Care 2011;27(1):6-10. https://doi.org/10.7196/SAJCC.111 [ Links ]
18. Mitchell W. Malpractice in the intensive care unit. South Afr J Crit Care 2011;27(1):2-4. https://doi.org/10.7196/SAJCC.114 [ Links ]
19. Wang Y, Wan Q, Lin F, Zhou W, Shang S. Interventions to improve communication between nurses and physicians in the intensive care unit: An integrative literature review. Int J Nurs Sc 2018;5:81-88. https://doi.org/10.1016/j.ijnss.2017.09.007 [ Links ]
20. Whitelaw A. Role of infection control in combating antibiotic resistance. S Afr Med J 2015;105(5). https://doi.org/10.7196/SAMJ.9650 [ Links ]
21. World Health Organization. WHO guidelines on hand hygiene in health care. Geneva: WHO 2009. https://apps.who.int/iris/bitstream/handle/10665/44102/9789241597906_eng.pdf;jsessionid=8DF9022271C3BE1A61EA1FA33DCB22DB?sequence=1 (accessed June 2019). [ Links ]
22. Callen J, Georgiou A, Li J, Westbrook J. The safety implications of missed test results for hospitalised patients: A systematic review. BMJ 2011;20:194-199. https://doi:10.1136/bmjqs.2010.044339 [ Links ]
23. Shamsuddin A, Shafie D. Knowledge of nurses in the preparation and administration of intravenous medications. Procedia Soc Behav Sci 2012;60:602-669. https://doi.org/10.1016/j.sbspro.2012.09.429 [ Links ]
24. Rout J, Essack S, Brysiewicz P. Are nursing infusion practices delivering full dose antimicrobial treatment? J Antimicrob Chemother 2019;74(12):3418-3422. https://doi.org/10.1093/jac/dkz365 [ Links ]
25. Botma Y, Botha H, Nel M. Transformation: Are nurse leaders in critical care ready? J Nurs Manag 2011;20(7):921-927. https://doi.org/10.1111/j.1365-2834.2011.01339.x [ Links ]
26. Uys L, Klopper H. What is the ideal ratio of categories of nurses for the South African public health system? S Afr J Sci 2013;109(5/6):1-4. https://doi.org/10.1590/sajs.2013/a0015 [ Links ]
27. Lee A, Cheung Y, Joynt G, Leung C, Wong W, Gomersall C. Are high nurse workload/staffing ratios associated with decreased survival in critically ill patients? A cohort study. Ann Intensive Care 2017;7(46):1-9. https://doi.org/10.1186/s13613-017-0269-2 [ Links ]
28. Mitchell B, Gardner A, Stone P, Hall L, Pogorzelska-Maziarz M. Hospital staffing and health care-associated infections: A systematic review of the literature. Jt Comm J Qual Pat Saf 2018;44(10):613-622. https://doi.org/10.1016/j.jcjq.2018.02.002 [ Links ]
29. Hugonnet S, Harbarth S, Sax H, Duncan R, Pittet D. Nursing resources: A major determinant of nosocomial infection? Curr Opin Infect Dis 2004;17(4):329-333. https://doi.org/10.1097/01.qco.0000136931.83167.d2 [ Links ]
30. Broom A, Gibson A, Broom, J, Kirby E, Yarwood T, Post Y. Optimizing antibiotic usage in hospitals: A qualitative study of the perspectives of hospital managers. J Hosp Infect 2016;94(3):230-235. https://doi.org/10.1016/j.jhin.2016.08.021 [ Links ]
 Correspondence:
Correspondence:
J Rout
joanrout@worldonline.co.za
Accepted 6 May 2020
Contribution of the study
Nurses are not well-integrated into antimicrobial stewardship. Insufficient training and education on aspects of antimicrobial stewardship are available to nurses.


{kind=link}
{kind=link}
{kind=link}