










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouthern African Journal of Critical Care (Online)
On-line version ISSN 2078-676X
Print version ISSN 1562-8264
South. Afr. j. crit. care (Online) vol.35 n.2 Pretoria Nov. 2019
http://dx.doi.org/10.7196/SAJCC.2019.v35i2.370
RESEARCH
Early identification and referral of organ donors in five private hospitals: A survey to determine the knowledge and views of critical care professional nurses pre and post a PowerPoint training intervention
L PrinsI; L HumanII
IRN, Hon Nursing, OrcID 0000-0003-2536-3572 Transplant Division, Netcare Christiaan Barnard Memorial Hospital, Cape Town, South Africa
IIM Nursing; Transplant Division, Netcare Christiaan Barnard Memorial Hospital, Cape Town, South Africa. OrcID 0000-0001-8418-1168
ABSTRACT
BACKGROUND. Internationally, the declining number of organ donors does not meet the rising demand for life-saving solid organ transplant operations. Critical care professional nurses play an important role in the identification of organ donors. A deeper understanding is needed of the missed opportunities of identification and referral of potential organ donors to organ transplant co-ordinators in the critical care environment.
OBJECTIVES. To describe the knowledge and views of critical care professional nurses (CCPNs) in South Africa concerning the early identification and referral of organ donors, and to describe the short-term effect of implementing a PowerPoint training intervention on nurses' knowledge in this domain.
METHODS. A mixed method, experimental, exploratory, descriptive study design was followed. Critical care professional nurses in seven intensive care units at five private hospitals completed a data collection instrument comprising 11 quantitative and three qualitative questions, before and after completing a PowerPoint training intervention. The post test was done directly after the training intervention due to the environment of nursing shift work.
RESULTS. A total of 173 (79%) CCPNs participated, from a population of 218. The median (interquartile range) score for all participants increased from 60% (48 - 76) prior to the PowerPoint training intervention, to 96% (88 - 96) after the intervention (p<0.0001). Three main themes emerged from the qualitative questions: stress experienced by the CCPNs during the organ donor process (62%); inadequate collaboration between doctors and nurses (34%); and the need for a policy (9%) to guide the donor referral process.
CONCLUSION. CCPNs' knowledge regarding the early identification and referral of potential organ donors increased significantly following a targeted PowerPoint training intervention. The identified themes suggest that CCPNs require support in order to effectively communicate with the donor's family and medical staff.
Keywords: Organ donor, identification, referral, organ transplant coordinators (OTCs), critical care professional nurses (CCPNs), doctors, PowerPoint training intervention (PPTI), barriers, education, collaboration, communication.
South Africa (SA) has a rich history in solid organ transplantation, with the first heart transplant performed at Groote Schuur Hospital, Cape Town, in 1967.[1] Organ donation is a prerequisite for transplantation, and it is therefore concerning that the number of organ donors in the Western Cape Province and nationally has decreased over the last decade.[2] Prompt identification and referral of potential brain stem dead donors in the intensive care units (ICUs) and emergency departments is of utmost importance, according to international studies.[3-5
The consent rate among families of potential donors in SA decreased from 55% in 1991 to 50% in 2001, and to 32% in 2011.[6,7] SA has a very low donor rate of 1.7 per million population,[2] in comparison with Spain, the world leader in organ donation, with a 40 per million population rate.[8] Spain is an international leader in the management of deceased organ donation, and by 2015 the country had trained 16 000 healthcare professionals regarding organ donation.[8] This illustrates that training and increased knowledge play a role in the early identification and referral of potential organ donors. In SA, there are currently 22 procuring organ transplant co-ordinators (OTCs),[9] which is clearly inadequate for a population of 57.73 million.[10]
The three OTCs (specifically responsible for organ procurement) for private hospitals in Cape Town visit 32 private hospitals from all the hospital groups in the Cape Peninsula and surrounding area on a monthly basis to provide training on appropriate identification and referral of organ donors. Potential organ donors are usually admitted to ICUs. After completion of brain stem death (BSD) tests by two qualified doctors, the potential donor should be referred to the OTC on call by the primary doctor, or the critical care professional nurses (CCPNs) after liaison with the primary doctor. In the absence of a national policy in hospitals on the identification and referral of organ donors to OTCs, this routine of referral was established by active communication with all role players (doctors and CCPNs). SA studies recommend that protocols and policies regarding the organ donation process should be implemented to ensure a formal, unified referral process.[6,11] The success of organ donation depends on a robust identification and referral process, the key role of the intensivists, the importance of protocols and excellent communication between the CCPNs and the procurement team.[3-5] CCPNs experience uncertainty, insecurity and a lack of clarity regarding their roles in organ donation; therefore a nationally endorsed protocol could solve this problem.[11-13]
International studies have reported barriers or challenges to donor identification and the donation process,[14-16] which include unfamiliarity with BSD diagnosis and the donor process, and inadequate training in stressful experiences such as discussing BSD and organ donation with donor families.[15] A Polish study concluded that poor physician communication and skills and fears about the procurement process may have affected involvement in organ procurement practice, with formal BSD diagnoses not being made by 41% of physicians owing to a lack of experience.[15]
Many missed opportunities for identification of organ donors have been linked to behaviours of healthcare professionals.[6,14,15,17] Floden et al[16]reported that 39% of CCPNs had experienced occasions where the subject of organ donation was never raised with the families of BSD patients. Nair[13] suggested that primary doctors managing brain dead patients do not want to be forced to contact OTCs.
An SA study suggested that CCPNs were also not aware of international extended selection criteria, for example that HIV-positive donors can donate organs to HIV-positive recipients, in order to increase the organ donor pool.[18] This lack of knowledge among nurses and other healthcare professionals about the organ donor process is experienced worldwide.[7,12,19]
The objective of this study was therefore to describe the knowledge and views of CCPNs on the early identification and referral of organ donors, and the impact of a PowerPoint (Microsoft, USA)-facilitated training intervention on knowledge scores.
Methods
Ethical considerations
Ethical approval (ref. no. 0-2015-0012) for in-house research was obtained from the research ethics committee of the private hospital group in which the study was conducted. Permission to undertake the study was obtained from the hospital managers, nursing and unit managers of the participating hospitals. The participants consented in writing to informed, anonymous and voluntary participation. The raw data were only available to the researchers, and kept in a secure place. The final in-house study was presented to and approved by the research ethics committee of the hospital group.
Research setting
The present study was conducted in seven ICUs (two medical, two surgical and three general) of five private hospitals in the Cape Peninsula. Biographical data are discussed under the data collection instrument.
Study design
A mixed-method, experimental, exploratory, descriptive design was followed to determine the knowledge and views of the CCPNs regarding the early identification and referral of organ donors. The mixed method comprised both quantitative and qualitative components to afford a method of triangulation, which has the potential to strengthen the rigour and enrich the findings of the study.[20,21]
Population
The total population (N=218) included male and female CCPNs, both permanent and regular agency, on the duty registers of the seven ICUs.
Sample
The participant sample comprised 173 CCPNs from 7 ICUs in 5 private hospitals. Permanent and regular agency CCPNs who were interested in the study and the PowerPoint training intervention were eligible for inclusion in the study. Enrolled nurses and enrolled auxiliary nurses were excluded.
Sampling
Non-probability purposive sampling was used to select the potential participants.'20,221 Not every element of a population has an opportunity to be selected for the study; thus the sample representativeness is decreased.[20,22] Purposive sampling, often used in nursing research, is also called selective sampling, as the researcher consciously selects certain subjects.[20]
Participation in the study was voluntary, and informed consent was obtained from all participants.
Data collection instrument
The researchers developed a data collection instrument appropriate for the SA organ donation context. The biographical data comprised participant age, whether they were permanent or agency staff, night or day staff, male or female and the hospital that they worked at. The researchers did not distinguish between ICU-trained and ICU-experienced CCPNs.
Eleven multiple choice questions were asked in the quantitative section of the data collection instrument. In the post tests, three open-ended questions were included in the qualitative section in order to obtain a richer description of CCPNs' views and experiences regarding the process of early identification and referral of organ donors.[20,22]
The multiple choice questions comprised 11 items with between 2 and 6 alternatives.[20,23] It was clearly stipulated on the data collection instrument, and communicated verbally to the participants, that more than one alternative could be correct. The objective scoring of multiple choice items was chosen in order to avoid scorer inconsistency. [20,23]
In the quantitative section, the following domains were included in the multiple choice questions:
• identification of potential donors (questions 1 and 2)
• extended selection criteria (question 3)
• definition of BSD (question 4, 7 and 8)
• early identification and referral of the BSD patient (questions 5 and 6)
• legal and ethical aspects (question 9)
• donor management (question 10)
• staff reflection and debriefing (question 11).
The qualitative section comprised three open-ended questions (questions 12 - 14) on the CCPNs' experiences in the organ donor process. These questions asked what was experienced as the most difficult or stressful part of organ donor management, what problems were experienced with the organ donor process and what could be done to improve the donor programme.
Validity
Face validity is a cursory review to verify that the data collection instrument measures the desired content.[20,22] Content validity refers to an in-depth evaluation of the extent to which the data collection instrument accurately reflects the concept being examined.[20,22] The data collection instrument was developed to measure the knowledge (quantitative section) and to describe the views (qualitative section) of CCPNs in ICUs on the early identification and referral of organ donors. A pilot study was not done, but both aspects of validity were established through review of the data collection instrument and the PowerPoint training intervention by two independent experts, namely an OTC with 20 years' experience in organ transplantation, and the research project manager of the private hospital group. Recommended changes were made by the researchers, whereupon the experts repeated the in-depth review.
Reliability
Reliability was improved by distributing the same instrument to all participants and by keeping the questions simple. During the completion of the data collection instruments by the CCPNs, the researchers were present to clarify any ambiguity.[20,22] The internal consistency of the pre-test and post-test data collection instruments was determined using Cronbach's a coefficient by an independent person with statistical expertise.
Qualitative data
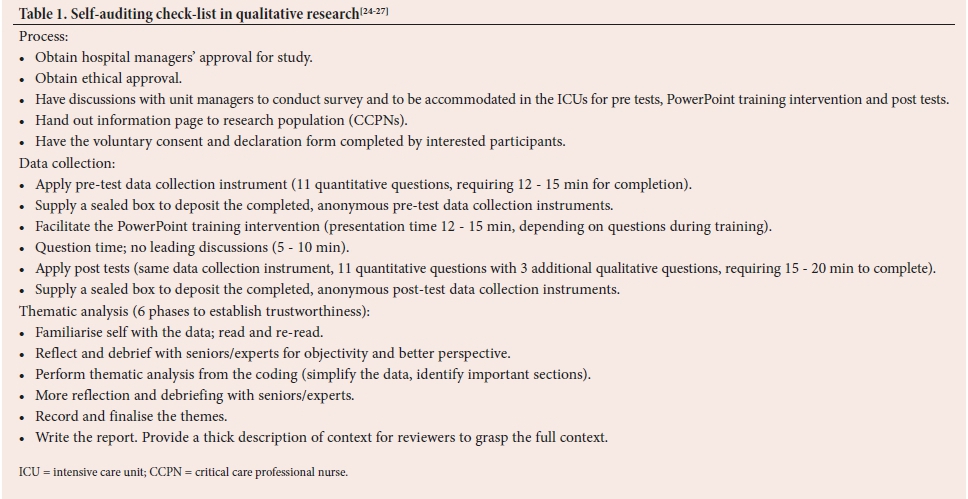
In order to enhance rigour and ensure trustworthiness of the qualitative component of this study, the researchers followed specific self-auditing steps (Table 1), compiled from the recommendations of other researchers.[20,24-27]
Trustworthiness
The criteria for trustworthiness below were applied to the qualitative section of the questionnaire results.[24-27]
Credibility
Familiarity: Early familiarity was established with the population, as monthly training was done on various topics of organ donation in the 7 ICUs of the 5 private hospitals where the study was conducted.[24,27]
Experience: Both researchers are ICU qualified nurses, and have extensive experience as OTCs.
Consent: The participants signed the consent and declaration voluntarily. They considered participation in the study as advantageous to them, as a form of in-service training, and they were interested in the topic of organ donation.
Researcher debriefing: The methods of the study were frequently discussed with an experienced OTC, as well as with the research project manager within the private hospital group. This contributed to the researchers' ability to keep perspective and widen their vision on the study.[25,26]
Validity: Appropriateness of the tools, processes and data enhance the quality and trustworthiness of qualitative research results.[27] Validity in this study was enhanced by using a mixed method to collect both quantitative and qualitative data on the same topic components, to afford a method of triangulation. This merged different perspectives, thus improving clarity of the data.[20,22] The two researchers worked together on the systematic manual coding of the data to provide a clearer understanding of the problem. The self-auditing check-list (Table 1) assisted in enhancing the appropriateness/validity of the analysis process[26,27]
Transferability
Other OTCs may apply the same qualitative questions to the ICUs where they perform training. They can judge transferability by the thick descriptions of the participants' responses.[24,27]
Dependability
The researchers ensured that the qualitative research process was logical, traceable and clearly documented to establish reliability.[25,26]
Confirmability
Confirmability involves establishing that the findings are based on participants' responses instead of the researcher's own preconceptions and biases, thus maintaining researcher objectivity.[20,24
PowerPoint training intervention
The training intervention was developed using an MS PowerPoint format. Sixteen informative slides were developed by the researchers regarding early identification and referral of potential organ donors. The main topics discussed in the slides were developed from the questionnaire (available at https://http://sajcc.org.za/public/sup/sajcc_370_survey.docx). The content was derived from two online courses on the organ donation process that were completed by both researchers.[28,29] The two researchers, who presented the training, utilised the PowerPoint training intervention in the ICUs, with between one and five participants at a time.
Data collection
Data were collected from May 2017 to July 2017. Both day and night shifts were included. After the participants had completed the pre-test questionnaire, the PowerPoint training intervention was presented by the researchers, and short discussions in the form of question time were held afterwards in relation to the training intervention. The data collection instrument (post test; the same 11 qualitative questions as in the pre test, with three additional qualitative questions) was then completed immediately after the PowerPoint training intervention. The anonymous data collection instruments were deposited in a sealed box and locked in the researchers' office.
Data analysis
The reliability of the data collection instrument (both pre and post the PowerPoint training intervention) was analysed using Cronbach's a statistic, which evaluates the internal consistency of data collection instrument items. A Cronbach's a of >0.7 was considered acceptable.[20,22]
The quantitative raw data were manually captured from the data collection instruments by one researcher (LP) on an Excel (Microsoft, USA) spreadsheet, with the second researcher (LH) performing data verification and entry checks.
Continuous data (data collection instrument scores) were tested for normality, and are presented as median (interquartile range (IQR)), as appropriate for nonparametric variables. The change in score from pre to post intervention was analysed using repeated analysis of variance (Anova) measures, and the effect of the participant's institution was evaluated using a two-way (between and within-group) Anova. A significance level of p<0.05 was considered statistically significant.
The data analysis for the qualitative responses occurred in three stages: description; analysis; and interpretation. The researchers read the answers to the open-ended questions several times to get a sense of the whole, and subsequently the data underwent coding and thematic analysis.[20,22]
Results
Data collection instrument reliability
Cronbach's a on the pre-test data collection instrument was 0.76, and the post-test a was 0.71, indicating acceptable internal consistency/ reliability of the pre and post tests.[20,22]
Population, sample and response rate
Pre-test questionnaires were made available to the total population of CCPNs (N=218), with a response rate of 173 (79.4%), giving a 3% margin of error at a 95% confidence interval. The 173 CCPNs who completed the questionnaire gave informed consent, completed the training intervention and were included in the final study sample.
Demographic characteristics
Of the 173 participants, 90% (n=156) were female and 10% (n=17) male; 58% (n=101) were on day duty and 42% (n=72) on night duty; 82% (n=141) were permanent and 18% (n=32) agency staff. The majority of nurses, 34% (n=59), were between 36 and 45 years old.
Quantitative data collection instrument responses
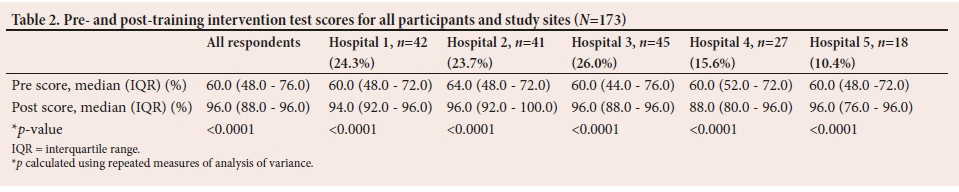
Participants overall scored a median (IQR) of 60% (48.0 - 76.0) before the intervention, and 96.0% (88.0 - 96.0) following (p<0.0001) (Table 2), with no difference in scores or change of scores among individual hospital sites (p=0.7). Data were not normally distributed, and therefore are correctly expressed as median (IQR).
The percentage of incorrect individual answers pre and post intervention are presented in Fig. 1. The worst-scoring baseline questions were those related to donor selection and brain death criteria. There was a marked improvement in scores for all questions (1 - 10) following the PowerPoint training intervention (Fig. 1).
Qualitative section
Question 12 on the difficult/stressful aspects of organ donor management was answered by 62% (n=108) of the participants.
Question 13 (problems experienced in the organ donor process) and question 14 (recommendations) in the qualitative section were both answered by 86 participants (50%).
In the qualitative section, three main themes were selected from the answers to the three open-ended questions.
Theme 1: The organ donor process is stressful
In question 12, 100% (n=108) of participants reported that they experienced stress in dealing with the donor's family, managing the donor and convincing 'resistant doctors' to refer the brain dead patient to the OTCs. The participants commented that the following caused them stress while dealing with the donor families: 'comforting the family'; 'some relatives are rude'; 'I get too emotional'; 'angry, aggressive family'; 'not enough time to deal with the family'; 'the emotions, and comforting the family'; 'the whole process is stressful'; and 'approaching the family of a potential donor'. Other stressors identified, which related to dealing with the brain dead patient's family, include the following: 'it is stressful dealing with the family'; 'stressful to comfort them [the family] and at times unable to inform them about the truth [patient being brain dead]'; 'it is stressful managing/ nursing the deceased donor'' 'to explain to the family why the patient is maintained on ventilation although brain dead'; 'poor cascade of communication with the doctors'; 'family's acceptance of the patient's brain dead status meaning death'; and 'management of family, very emotional'.
A total of 33% (n=28) of the participants reported in Question 13 that nursing and managing the brain stem dead donor caused them stress: 'there is lots to be done, doing all the paperwork, managing the electrolytes and the family'; 'patient and whole process is stressful'; 'trying to keep organs well perfused'; and 'knowing that the donor is actually dead'.
The participants responded that doctors were also a source of stress in the early identification of organ donors: 'doctors not keen and open to organ donation'; 'when doctors give orders other than those of the OTCs'; [to] 'convince doctor that patient is a potential donor'; and difficulties 'getting doctors involved'.
Theme 2: Inadequate collaboration
between doctors and nurses In question 13, 34% (n=29) of participants replied that some doctors contribute to problems (also termed barriers or challenges in international studies), by not identifying and referring potential organ donors. The CCPNs stated that 'some doctors are not encouraging the programme'; 'doctors [are] not always approachable', 'resistant doctors cause stress'; 'some doctors [are] not keen' to refer the potential organ donor; 'educate the doctors'; 'doctors [are] not committed to the process'; and 'approaching the doctors' causes problems and stress.
Theme 3: The need for a national organ donation policy and further training of CCPNs and doctors
Eight (9%) participants recommended in question 14 that a national protocol or policy would contribute to improved referral of potential organ donors. The participants referred to: 'lack of protocol'; 'a policy to be in place'; 'a policy is required'; 'get a policy'; and 'a policy will make referral easier.'
The CCPNs responded in question 14 with recommendations for the organ donor process that: they 'need training - [do] not [get] enough exposure'; they need 'in-service training every 6 months'; the 'presentation was done excellently, but [they] need regular training'; and there is a need to 'educate doctors' on the early referral of organ donors.
Discussion
This was the first SA study to use mixed methods to investigate the level of knowledge and views of CCPNs relating to early identification and referral of organ donors.
Demographic data
The study was strengthened by sampling interested CCPNs on all four shifts in the ICUs, on day and night duty, including both permanent and regular agency CCPNs. This resulted in a high response rate of 79% (n=173/218), and ensured that the sample adequately reflected the population.
Quantitative section
Prior to the PowerPoint training intervention, there was a median gap in knowledge of 40% related to the early identification, referral and management of organ donors. After the intervention, there was a median overall improvement of 36% (from 60 - 96) in knowledge scores (Table 2), with marked improvements in the domains identified as having poor knowledge at baseline (Fig. 1); however, areas needing further training were identified, as discussed below.
Ongoing training required
It was of concern that the CCPNs did not score well even after the PowerPoint training intervention in the post-test questions pertaining to the identification of a potential organ donor (question 1), and the criteria for declaring a patient brain stem dead (question 8), as reflected in Fig. 1. This identifies a need for further training in these areas. International studies support the need for ongoing training in the organ donor process.[8,9,15,16]
Ongoing training is required regarding the organ donor process in the light of CCPNs' working shifts, and the frequent rotation of CCPNs in ICUs. Currently the OTCs visit the
ICUs on a monthly basis to share information and new research, and to perform training on the organ donor process.
When to call the OTC
The best scores were obtained by the participants in questions 2, 4 and 5 (Fig. 1). In question 5, a total of 96% (n=166) of the CCPNs knew in the post test when to contact the OTCs. However, a number of problems (internationally also called barriers or challenges'[15,16]) were identified by the participants in the open-ended, qualitative questions, which prevented them from referring potential organ donors to the OTCs. Naidoo et al.[6]state that national standardisation, with a policy and training opportunities for all relevant stakeholders in the organ donor process, are essential for referral of potential organ donors.
Extended selection criteria
A remarkable improvement in knowledge was noted following the PowerPoint training intervention for the question on HIV-positive brain stem dead patients being able to donate to HIV-infected recipients, an extended criterion for HIV-positive organ donors. This is an important area in the SA context, given the high prevalence of HIV infection in our population.[18]
Legal and ethical aspects
Ongoing training regarding the ethical aspects involved in the organ donor process was identified as required, as 27% (n=47) of participants were incorrect after the PowerPoint training intervention. There are many guiding and controlling conditions for organ donation contained in Chapter 8 of the National Health Act No. 61 of 2003.[30] It is, for example, crucial for the CCPNs to know that the donor family may revoke consent at any stage during the process of organ donation, and that the BSD tests should not be done while the patient is under sedation, or for 12 hours after a sedation infusion is discontinued.[30]
Qualitative section
In question 12, on the difficult/stressful aspects of organ donor management, all participants (100%) alluded to the stress they experience in dealing with the families of donor patients, the management of the donor and the reluctance of doctors to refer the potential donors to the OTCs.
Questions 13 and 14 were answered by only 50% of the participants. This was probably owing to the fact that not all CCPN participants had previously nursed organ donors in ICU, and were therefore unable to express opinions or describe experiences. Those who responded to these questions provided valuable information that could improve the organ donor process.
The three recurring main themes derived from these qualitative questions after exploration of the answers are discussed below.
Theme 1: Stress in the donor process
In answer to the question on difficult/stressful situations in the donor process (question 12), the participants reported experiencing stress in response to the administrative load of the organ donation process, the clinical management of the donor and dealing with the family of the donor. The stress related to the donor families was twofold: they can be demanding regarding information and patient care, and intense emotions are involved pertaining to the death of a family member. The critical care staff and the OTCs must form a strong team to optimally facilitate the questions and the grief of the family, to relieve the emotional burden on the CCPNs.[16,32] Managing the families of organ donors is emotionally and psychologically challenging, and increases the demands on an already stretched team.[15,161]
A total of 90% of participants responded in question 11 that the OTCs should perform reflection and debriefing sessions with the CCPNs after an organ donation process. The function of debriefing is to identify aspects of team performance that went well, and those that did not, and to determine opportunities for improvement of the process.[32,33]
Reflection and debriefing sessions with the healthcare professionals involved should be routinely conducted during and after procurement of organs.[16,32,33]
Theme 2: Inadequate collaboration between CCPNs and doctors
The vast majority (96%) of the CCPNs knew in the post test when to contact the OTCs (question 5, quantitative section). Interestingly, however, although no questions were posed specifically related to the referring doctors in either the quantitative or qualitative sections of the data collection instrument, communication/collaboration with referring doctors was identified as a major barrier to the organ donation referral process. Slabbert and Venter[12] suggest that the general attitude of SA physicians is that the living have a higher priority than end-of-life patients; therefore bed availability is more important than referring an organ donor.
Researchers have also alluded to the problem that doctors at the bedside often close the case of the potential organ donor to avoid the long donor procedure.[3,13-15] It is argued [12,15] that physicians cannot avoid death management in their daily activities, but it is possible to avoid the purported extra work involved in organ donation by not referring the brain dead patient as an organ donor. A possible solution would be to simultaneously educate the doctors and implement the policy regarding organ donor referral.'14-161 Some physicians, according to a Dutch study, may give relatives the impression that they have to make a rapid decision regarding organ donation, which does not reflect best practice and could lead to organ donor consent being lost. [34] Communication among the intensivist, the CCPNs in the ICUs and the OTCs needs to improve, and it is suggested that the key role of the intensivist in the organ donation process be optimised.'31
Theme 3: The need for a national organ donation policy, and further training
It was concluded by a small number of the participants in the present study, and has been underpinned by other studies,[6,11] that owing to the lack of a nationally endorsed protocol or policy on organ donor referral, CCPNs are reluctant to refer organ donors independently from the doctors, as they fear reprisal and the burden of caring for a mechanically ventilated donor.'161 The need for a national policy has been previously raised in SA, but at that time (2017) the SA Medical Association chairperson declared that doctors must first be educated prior to enforcing a policy. [13] Currently in SA it is argued that a routine legislated donor referral policy should be followed by all hospitals.[6,11,12]Martin-Loeches et al. [3] concluded that clinical protocols are important for an improved multidisciplinary approach to organ donation. There are many accessible examples of such policies.[5,35]
Participants in our study spontaneously recommended that increased in-service training should be performed for early identification and referral of organ donors, to promote the organ donation programme. The three OTCs from the private sector in the Cape Peninsula are committed to monthly training visits to the ICUs and emergency departments of 32 hospitals on the Cape Peninsula and in the non-urban areas of the Western Cape Province. The importance of ongoing staff training in the organ donor process is supported by national and international researchers.[7,8,11,16]
There was potential for the introduction of researcher bias in the qualitative section; however, we adhered to the self-auditing checklist (Table 1), and consulted frequently with experts to improve objectivity.'20,221 In retrospect, we had made the assumption that the lack of knowledge among CCPNs was a contributing factor for the low referral rate of brain dead patients as organ donors, and this may have introduced bias. The study results in the qualitative section, however, suggested more intricate challenges and barriers. The CCPNs alluded to stress in dealing with the donor family, and doctors' negative attitudes toward referral of potential donors to the OTCs.
Strengths and limitations
The data collection instrument for this study was compiled by the researchers, as a validated tool was not available in the SA context. This data collection instrument can be used by other OTCs in SA. However, although attempts were made to ensure content and face validity, and the data collection instrument had a high level of internal consistency, the lack of formal validation and reliability testing is a limitation of this study.
The study is further limited by only having sampled five hospitals within one hospital group, which may limit the external validity and generalisability of the study. The study was, however, strengthened by the very high response rate to the survey, and the high level of attendance at the PowerPoint training interventions.
The study was also limited by testing participants before and soon after the PowerPoint training intervention, and it is not known whether there was retention of knowledge in the longer term - this requires further investigation. There is much argument about performing the post test immediately after any PowerPoint training intervention;[36,371 however, this immediate post-test was a practical solution owing to time constraints and the logistical problems of sampling the same staff members again for post tests after a month in an environment of shift work. In the present study, no attrition of participants occurred in the post test that was applied immediately after the PowerPoint training intervention, in contrast to a Botswana nursing study[371 that concluded a reduction in participants from 154 to 85 in a post test 6-months after the initial test.
Although there was a reduced response rate to questions 13 and 14 in the qualitative section, it is of note that the CCPNs who completed that section had mostly managed an organ donor case, and therefore reported on first-hand experiences. The qualitative section supplemented the quantitative section in triangulation, and thus highlighted barriers (problems, challenges) that we would not otherwise have been aware of. These problems/barriers comprised stress experienced by the CCPNs, the need for a policy and the lack of collaboration between doctors and CCPNs in the donor referral process, as underpinned by other research studies.[6,14-161
Unfortunately, data were not collected on whether respondents were ICU trained or not, or if they had managed an organ donor in ICU before, and these two aspects should be added to the demographic data on the data collection instrument for future research.
Owing to time constraints in the ICUs, no in-depth interviews were completed with the participants. However, the results of the three qualitative questions on the data collection instrument added valuable information to the study in emphasising aspects that the researchers did not anticipate, for example, the stress experienced in managing the donor and the family, inadequate collaboration between CCPNs and doctors and the need for a policy on the organ donor process. Further qualitative research using interviews is recommended to confirm and further explore the findings of this study.
Conclusion
It is recommended that this data collection instrument and PowerPoint training intervention be utilised by OTCs for further research and training of CCPNs in all hospital groups, considering the improvement in knowledge demonstrated after a single such intervention. The need for ongoing training and the long-term retention of the knowledge gained requires further research.
Although the majority of CCPNs in the present study knew when to refer a potential organ donor to the OTCs, several barriers were identified that prevented them from doing so in practice. These barriers included the perception that caring for the donor and his or her family is arduous and stressful; therefore, support by the OTCs during donor management and staff debriefing after the donor process is extremely important. The CCPNs experienced stress due to the lack of a common policy to guide the donor process. The drafting of a nationally endorsed policy on the early identification and referral of organ donors is strongly recommended.
Many missed opportunities for the identification of organ donors have been linked to the behaviour and attitudes of healthcare professionals. The success of the organ donor process greatly depends on the early identification and referral of brain dead patients in ICUs, and therefore collaboration between the CCPNs, physicians and surgeons and OTCs is of utmost importance, to streamline referrals. Most of the CCPNs knew when they should refer the potential organ donor, but were concerned about the reluctance of doctors to refer the potential donors to the OTCs. Inadequate collaboration between doctors and nurses was spontaneously identified by respondents as a major barrier in the organ donation process. Further research is recommended to determine how to overcome these barriers, as optimal team communication and interrelations are of utmost importance in the organ donor process.
Acknowledgements. We are grateful to the CCPNs who participated in this study. We dedicate this paper to the families of deceased donors who consented to organ donation. We acknowledge and thank Prof. Brenda Morrow for her contribution in the interpretation of the statistics, and language editing.
Author contributions. Equal contributions.
Funding. None.
Conflicts of interest. None.
References
1. Wilke M. Chris Barnard's first heart transplant - the night he stared into an empty chest. Health 24, 2017. http://www.health24.com/Medical/Heart/Heart-transplants/chris-barnards-nrst-heart-transplant-the-night-he-stared-into-an-empty-chest-20170929 (accessed 15 June 2018). [ Links ]
2. Organ Donor Foundation of South Africa. Statistics, how we create public awareness, Transplant centres in South Africa. http://www.odf.org.za (accessed 27 Nov 2017). [ Links ]
3. Martin-Loeches I, Sandiumenge A, Charpentier J, et al. Management of donation after brain death (DBD) in the ICU: The potential donor is identified, what's next? Intensive Care Med 2019;45(3):322-330. https://doi.org/10.1007/s00134-019-05574-5 [ Links ]
4. Rudge C, Matesanz F, Delmonico FL, Chapman J. International practices of organ donation. Br J Anaesth 2012;108(1):i48-i55. https://doi.org/10.1093/bja/aer399 [ Links ]
5. Donor Identification and Referral Strategy Group, NHS Blood and Transplant. Timely identification and referral of potential organ donors: A strategy for implementation ofbest practice. https://nhsbtdbe.blob.core.windows.net/umbraco-assets-corp/1337/timely-identification-and-referral-of-potential-organ-donors-nhsbt.pdf (accessed 27 Nov 2017). [ Links ]
6. Naidoo P, Etheredge HR, Rambiritch V, Singh A, Mahoney S, Naidu V. Non-referral of potential organ donors in South Africa: Insights, challenges and ethical dilemmas. Pan Afr Med J 2018;29:223. https://doi.org/10.11604%2Fpamj.2018.29.223.14756 [ Links ]
7. Kahn D, McCurdie F, Michaelides A. Socioeconomic factors, as well as race, impact on consent rates for organ donation. Proceedings of the 25th Southern African Transplantation Society Congress, 29 July - 2 August 2013. Durban: South African Transplant Society, 2013. [ Links ]
8. Badcock J. How Spain became the world leader in organ donation. Newsweek Magazine, 20 February 2015. www.newsweek.com/2015/02/20/spain-has-become-world-leader-organ-donations-305841.html (accessed 16 April 2016). [ Links ]
9. Etheredge HR. 'Hey sister! Where's my kidney?': Exploring ethics and communication in organ transplantation in Gauteng, South Africa. PhD thesis. Johannesburg: University of Witwatersrand, 2015. http://wiredspace.wits.ac.za/bitstream/handle/10539/21425/Hey%20sister%20-%20where%27s%20my%20kidney.pdf?sequence=2&isAllowed=y (accessed 25 October 2019). [ Links ]
10. Statistics South Africa. Mid-year population estimates, 2018. https://www.statssa.gov.za/publications/P0302/P03022018.pdf (accessed 13 July 2019). [ Links ]
11. Crymble K, Etheredge HR, Fabian J, Gaylard P. Nurses' knowledge about and attitudes toward organ donation in state and private hospitals in Johannesburg, South Africa. South Afr J Crit Care 2017;33(2):52-57. https://doi.org/10.7196%2F322 [ Links ]
12. Slabbert M, Venter B. Routine referrals: A possible solution for transplantation shortages. S Afr J Bioethics Law 2017;10(1):15-19. https://doi.org/10.7196%2Fsajbl.498 [ Links ]
13. Nair N. Body donors could help as many as 60 people. Sunday Times, 14 August 2017. https://www.timeslive.co.za/sunday-times/lifestyle/health-and-sex/2017-08-14-donating-sons-organs-would-have-been-what-he-wanted/ (accessed 27 November 2017). [ Links ]
14. Girlanda R. Deceased organ donation for transplantation: Challenges and opportunities. World J Transplant 2016;6(3):451-459. https://doi.org/10.5500%2Fwjt.v6.i3.451 [ Links ]
15. Kosieradzki M, Jakubowska-Winecka A, Feliksiak M, et al. Attitude of healthcare professionals: A major limiting factor in organ donation from brain-dead donors. J Transplant 2014:296912. https://doi.org/10.1155/2014/296912 [ Links ]
16. Flodén A, Persson L, Rizell M, Sanner M, Forsberg A. Attitudes to organ donation among Swedish ICU nurses. J Clin Nursing 2011;20(21-22):3183-3195. https://doi.org/10.1111/j.1365-2702.2011.03756.x [ Links ]
17. Butler HE. Nurses' intentions and behaviours regarding organ donation: A scoping review. MSc thesis. Vancouver: University of British Columbia, 2017. http://hdl.handle.net/2429/63107 (accessed 15 Jan 2018). [ Links ]
18. Muller E, Barday Z, Mendelson M, Kahn D. Renal transplantation between HIV-positive donors and recipients justified. S Afr Med J 2012;102(6):497-498. [ Links ]
19. Cebeci F, Sucu G, Karazeybek E. The roles of nurses to augment organ donation and transplantation: A survey of nursing students. Transplant Proc 2011;43(2):412-414. https://doi.org/10.1016/j.transproceed.2011.01.048 [ Links ]
20. Burns N, Grove SK, Gray JR. Understanding Nursing Research: Building an Evidence-Based Practice. 6th edition. St. Louis: Saunders Elsevier, 2014. [ Links ]
21. Shorten A, Smith J. Mixed methods research: Expanding the evidence base. Evid Based Nurs 2017;20(3):74-75. https://doi.org/10.1136/eb-2017-102699 [ Links ]
22. Polit DF, Beck CT. Essentials Of Nursing Research: Appraising Evidence for Nursing Practice. 9th edition. Philadelphia: Lippincott Williams and Wilkins, 2010. [ Links ]
23. Brame CJ. Writing good multiple choice test questions. https://wp0.vanderbilt.edu/cft/guides-sub-pages/writing-good-multiple-choice-test-questions (accessed 15 February 2017). [ Links ]
24. Guba EG. ERIC/ECTJ Annual review paper: Criteria for assessing the trustworthiness of naturalistic inquiries. Educ Commun Techn J 1981;29(2):75-91. [ Links ]
25. Shenton AK. Strategies for ensuring trustworthiness in qualitative research projects. Educ Inform 2004;22(2):63-75. [ Links ]
26. Nowell LS, Norris JM, White DE, Moules NJ. Thematic analysis: Striving to meet the trustworthiness criteria. Int J Qualit Meth 2017;16:1-13. [ Links ]
27. Leung L. Validity, reliability and generalisability in qualitative research. J Family Med Prim Care 2015;4(3):324-327. [ Links ]
28. Transplant Procurement Management, Donation & Transplantation Institute. Self-study online course in organ donation. Barcelona: University of Barcelona, 2016. https://tpm-dti.com/training/self-study-online-course-in-organ-donation/ (accessed 24 August 2016). [ Links ]
29. Thomson D. Organ donation: from death to life. Cape Town: University of Cape Town: Coursera, 2018. www.coursera.org/learn/organ-donation (accessed 16 March 2018). [ Links ]
30. South Africa. National Health Act No. 61 of 2003. [ Links ]
31. Wisdom J, Creswell JW. Mixed methods: Integrating quantitative and qualitative data collection and analysis while studying patient-centred medical home models. Rockville, MD: Agency for Healthcare Research and Quality, 2013. [ Links ]
32. De Azevedo Guido L, da Costa Linch GF, Andolhe R, Conegatto CC, Tonini CC. Stressors in the nursing care delivered to potential organ donors. Rev Lat Am Enfermagem 2009;17(6):1023-1029. https://doi.org/10.1590/S0104-11692009000600015 [ Links ]
33. Elliott D, Aitken L, Chaboyer W. ACCCN's Critical Care Nursing. 2nd edition. Australia: Elsevier, 2011. [ Links ]
34. De Groot J, Vernooij-Dassen M, de Vries A, et al. Intensive care staff, the donation request and relatives' satisfaction with the decision: A focus group study. BMC Anesthesiol 2014;14:52. https://doi.org/10.1186/1471-2253-14-52 [ Links ]
35. East Cheshire NHS. Operational policy for organ donation and required referral. https://www.eastcheshire.nhs.uk/About-The-Trust/policies/O/Operational%20Organ%20Donation%20Policy%20and%20Required%20Referral%20ECT2566.pdf (accessed 15 January 2018). [ Links ]
36. Kumari V, Devi S, Narayani A. A study of pre- and post-test knowledge score of nurses on care of patient with central venous access devices in selected oncology hospital of Bangalore. Int J Public Health Epidemiol 2016;5(1):220-230. [ Links ]
37. Rajeswaran L, Cox M, Moeng S, Tsima BM. Assessment of nurses' cardiopulmonary resuscitation knowledge and skills within three district hospitals in Botswana. Afr J Prim Health Care Fam Med 2018;10(1):1633. https://doi.org/10.4102/phcfm.v10i1.1633 [ Links ]
 Correspondence:
Correspondence:
L Prins
Lettieprins@isp247.co.za
Accepted 29 August 2019
Contribution of study
• The findings of this study will contribute to the increase in organ donor referrals. Increased education of critical care professional nurses and doctors on effective communication, and the early identification and referral of organ donors, will expectedly help to resolve the critical barriers in the organ donor process.


{kind=link}
{kind=link}
{kind=link}