










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouthern African Journal of Critical Care (Online)
On-line version ISSN 2078-676X
Print version ISSN 1562-8264
South. Afr. j. crit. care (Online) vol.35 n.2 Pretoria Nov. 2019
http://dx.doi.org/10.7196/SAJCC.2019.v35i2.394
RESEARCH
Contamination of pulse oximeter probes before and after decontamination in two intensive care units
F DesaiI; J ScribanteII; H PerrieIII; M FourtounasIV
IBSc, MB BCh, DA (SA); Department of Anaesthesiology, School of Clinical Medicine, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa. OrcID 0000-0003-1834-8358
IIPhD; Department of Anaesthesiology, School of Clinical Medicine, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa. OrcID 0000-0002-2221-5024
IIIMSc; Department of Anaesthesiology, School of Clinical Medicine, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa. OrcID 0000-0002-9890-7887
IVMB ChB, DA (SA), FCA (SA), MMed (Anaes), Dip HIV Man (SA); Department of Anaesthesiology, School of Clinical Medicine, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa. OrcID 0000-0002-3678-018X
ABSTRACT
BACKGROUND. The internal surfaces of pulse oximeter probes may be overlooked as hot spots for pathogenic microorganisms in an intensive care unit (ICU), thereby contributing to the high incidence of hospital-acquired infections.
OBJECTIVES. To determine the growth and identification of microorganisms on pulse oximeter probes in the multidisciplinary ICU (MICU) at Charlotte Maxeke Johannesburg Academic Hospital and the burns ICU (BICU) at Chris Hani Baragwanath Academic Hospital, before and after decontamination.
METHODS. This was a cross-sectional, comparative and contextual study, using purposive sampling. Data were collected from the internal surfaces of 34 pulse oximeter probes in a MICU and BICU. Each pulse oximeter probe was swabbed before and after decontamination. The endemic microorganism profile for the two ICUs was obtained from a laboratory database.
RESULTS. Internal surfaces of 31 (91%; 95% confidence interval (CI) 0.76 - 0.98) pulse oximeter probes were contaminated with 9 different pathogenic microorganisms pre decontamination. Acinetobacter baumannii, Klebsiella pneumoniae and Pseudomonas aeruginosa were endemic to both ICUs, and were the most-frequently isolated microorganisms. Staphylococcus aureus was the most common microorganism endemic to both ICUs, isolated on the internal surfaces of only 2 pulse oximeter probes. Of the internal surfaces of pulse oximeter probes, 6 (18%; 95% CI 0.07 - 0.35) remained contaminated post decontamination, with a microorganism growth reduction of 80% (p=0.0001).
CONCLUSION. The internal surfaces of pulse oximeter probes may serve as hot spots for an array of pathogens with the potential to cause infection and outbreaks in ICUs. Decontamination of the internal surfaces of pulse oximeter probes should be emphasised.
Keywords: Contamination, decontamination, microorganisms, pulse oximeter probes, intensive care units.
Pulse oximeter probes are non-critical devices, but while they may require either only low-level disinfection, if not soiled with blood, or high-level disinfection if soiled with blood,[1] they may be a source of infection. Pulse oximeter probes are regularly used as part of basic monitoring during the transport of critical patients to and from intensive care unit (ICU) settings, and form part of standard monitoring equipment within the ICU.[2] It is questionable whether the internal crevices that house the diodes are cleaned adequately, particularly in a busy hospital environment with a high patient turnover and limited time for adequate decontamination of equipment.[3] A patient's finger can occupy a pulse oximeter probe for a long time during ICU admission, leading to sebum build-up and, ultimately, becoming a cocoon for microorganisms.'41 The internal surfaces of pulse oximeter probes are frequently soiled with various materials. Soiling can impede the inactivation of microorganisms, and inhibit the activation of disinfectants used.'51 Prolonged contact between pulse oximeter probesand patients' skin may lead to overheating and skin injury.[6] Furthermore, the tight application may lead to necrosis,[6] compromising the innate immunity offered by the skin.[7]
Previous research has shown non-critical devices to be unsuspected reservoirs housing significant numbers and strains of microorganisms.[8-20] Studies have reported non-critical devices to be responsible for outbreaks of pathogens.[8,10] Most research on non-critical devices has come from developed countries, and implicated sphygmomanometer cuffs,[12] electrocardiograph leads,'13-stethoscopes[14] and temperature probes[15] as reservoirs. Other devices such as orthopaedic tourniquets,'161 sharps containers,[17] computer keyboards,[18] gloves'191 and telephones'201 have also been implicated. A few studies have found pulse oximeter probes to play a role in hospital-acquired infection (HAI) transmission,[3,4,21-24] and three of these studies describe outbreaks traced back to pulse oximeter probes as unsuspected sources of HAI.[21,22,24]
Burns and HIV are two of the main causes of immunosuppression in patients admitted to ICUs. In South Africa (SA), burn injuries account for the highest number of unnatural causes of death in children.'25 Furthermore, HIV-associated diseases accounted for 50% of hospital admissions in 2011, and it is predicted that HIV-positive patients will account for up to 70% of hospital costs in the future.'261 The innate immunity offered by the skin in patients with a burn injury is markedly reduced,'271 and HIV-positive patients are likely to have dry skin.'28 Therefore, the skin of such patients is more likely to be breached by microorganisms, placing them at higher risk of cross-contamination from contaminated pulse oximeter probes.'291 Ideally, disposable devices should be used on these patients to avoid cross-contamination.'30 However, in a resource-limited country such as SA, disposable devices are not usually attainable in the public sector. In Johannesburg, SA, at Charlotte Maxeke Johannesburg Academic Hospital (CMJAH) and Chris Hani Baragwanath Academic Hospital (CHBAH), the burden of HAI is of significance in the multidisciplinary and burns ICUs (MICUs and BICUs), respectively, as both ICUs are occasionally closed down during outbreaks of extensively drug-resistant microorganisms. No research could be identified that has addressed non-critical devices, or specifically pulse oximeter probes, as potential reservoirs for HAI in SA. The aim of this study was to determine the growth and identification of microorganisms on pulse oximeter probes in the MICU at CMJAH and the BICU at CHBAH, before and after decontamination.
Methods
This was a cross-sectional, comparative and contextual study. An ethics waiver from the Human Research Ethics Committee (Medical) (ref. no. W-CBP-180601-01), and approval from other relevant authorities, were obtained.
The MICU at CMJAH and the BICU at CHBAH were chosen because they are known to experience outbreaks of Acinetobacter baumannii. All available pulse oximeter probes within the ICUs were sampled, to formulate a pool of pulse oximeter probes to meet sample size. The growth of microorganisms between the two ICUs was not compared. Each pulse oximeter probe was given a study number. In consultation with a biostatistician, a sample size of at least 33 pulse oximeter probes for each group was determined to have a significance of 5% and statistical power of 90%, with the proportion of contaminated pulse oximeter probes being estimated to be 0.6 pre decontamination, and 0.3 post decontamination, based on proportions of contaminated and decontaminated pulse oximeter probes identified in the literature.'4,231 Group 1 consisted of pulse oximeter probes pre decontamination, and group 2 of the same pulse oximeter probes post decontamination.
The unit nursing managers confirmed that no written protocols were available within the ICUs regarding the decontamination of equipment. The ICUs' standard decontamination practices consisted of cleaning soiled pulse oximeter probes with a Webcol swab (70% isopropyl alcohol) followed by disinfection with QualiClean (a chlorine-based disinfectant) (personal communication: Sr Rafu, MICU CMJAH; Sr Churu, paediatric BICU CHBAH; Sr Dlamini, Adult BICU CHBAH; 20 June 2017).
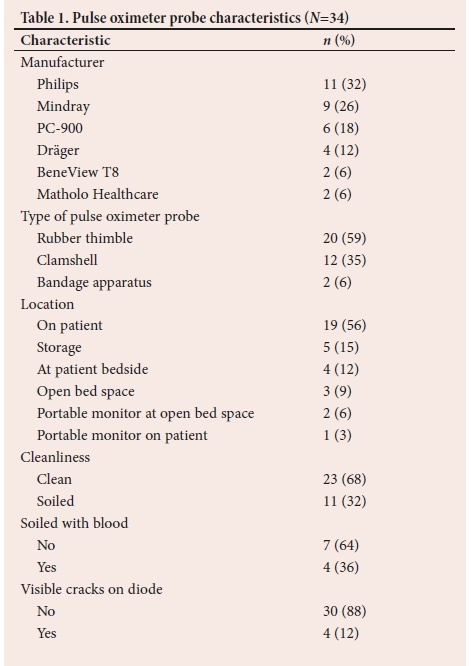
The characteristics (manufacturer; type of pulse oximeter probe; location; cleanliness; soiled with blood; and visible cracks on diode) of each pulse oximeter probe were captured on a data collection sheet.
The first author was the sole data collector. Without prior warning to unit nursing staff, all samples were collected on 4 September 2018. The internal surfaces of pulse oximeter probes housing the diode sensors served as test surfaces. Test surfaces were swabbed in a standardised manner using a swabbing technique adapted from Nandy et al.[1]Strict barrier precautions were maintained. The data collector's hands were disinfected with D-Germ hand antiseptic, and sterile gloves were donned. Test surfaces were swabbed using sterile, M40-compliant transwabs in Amies transport medium. A continuous rolling method from point A to point B, following the arrows as illustrated in Fig. 1, was used, until the entire test surface was covered. This process was repeated on the opposite test surface of the same pulse oximeter probe with the same swab. The swab was then cautiously placed back in the transport medium without touching the rim of the container. Old gloves were discarded, and new sterile gloves donned. Test surfaces were cleaned with a Webcol swab (70% isopropyl alcohol) vertically, from top to bottom, with three strokes.[4] Intermediate-level disinfection of the test surfaces was carried out using sterile gauze (folded 2 cm wide) soaked in Qualiclean (30 g sachet diluted in 10 L cold water until a clear solution was achieved, as per manufacturer instructions, yielding a chlorine strength of 250 ppm), in three vertical strokes, from top to bottom.[4] Test surfaces were allowed to dry for 30 seconds (exposure time for Qualiclean). Old gloves were discarded, and new sterile gloves donned. The test surfaces of the decontaminated pulse oximeter probes were re-swabbed using the technique described.

Samples were labelled according to the Vermaak and Partners Pathologists Laboratory's standardised form for identifying specimens, and transported to the laboratory in Rosebank, Johannesburg, without delay. Samples were processed according to good laboratory practice. Following the identification of microorganisms, viable counts were determined using a colony count, which is a semiquantitative method of streaking out on miniature plates.
The laboratory defined colony count scores of 0+, 1+, 2+ and 3+ to reflect scanty growth, low-level contamination, medium-level contamination and high-level contamination, respectively. Sensitivity testing was not performed, owing to financial constraints.
The endemic microorganism profile for the two ICUs represented a 4-month period around data collection. All clinical specimens received by the National Health Laboratory Service from the two ICUs for the period 1 June 2018 to 30 September 2018 were obtained from the National Health Laboratory Service database. Culture-positive clinical specimens provided a reflection of the microbiological epidemiology of the ICUs for this period.
Data were entered into an Excel (Microsoft, USA) spreadsheet, and statistical analysis was performed in consultation with a biostatistician.
Descriptive statistics (counts and percentages) were used for categorical data. The proportions of pulse oximeter probes contaminated before and after disinfection were compared using McNemar's test. A p-value of <0.05 was considered to be statistically significant.
Results
A total of 34 pulse oximeter probes were sampled between the two ICUs. Of these, 26 (77%) were at the bedside and 8 (24%) were from portable monitors, or found in storage. Nine (26%) pulse oximeter probes were sampled from the MICU at CMJAH, and 25 (74%) from the BICU at CHBAH. Eleven (32%) pulse oximeter probes were sampled from the paediatric BICU, and 14 (41%) from the adult BICU. Table 1 shows the characteristics of the pulse oximeter probes.
From the test surfaces of the 34 pulse oximeter probes sampled before decontamination, 31 (91%; 95% CI 0.76 - 0.98) were contaminated. Of these, 8/9 (89%; 95% CI 0.52 - 0.99) and 23/25 (92%; 95% CI 0.74 - 0.99) pulse oximeter probes from the MICU and BICU were contaminated, respectively. Twenty-five (81%) contaminated pulse oximeter probes isolated one microorganism each, and 6 (19%) contaminated pulse oximeter probes isolated two microorganisms each.
Of the test surfaces of the 34 pulse oximeter probes sampled after decontamination, only 6 (18%; 95% CI 0.72 - 0.35) were contaminated. Of these, 2/9 (22%) and 4/25 (16%) were from the MICU and BICU, respectively.
The results of bacterial contamination of pulse oximeter probes before and after decontamination are presented in Table 2.
Microorganism growth was reduced by 80% after cleaning with a Webcol swab and disinfection with Qualiclean, which was statistically significant (p=0.0001).
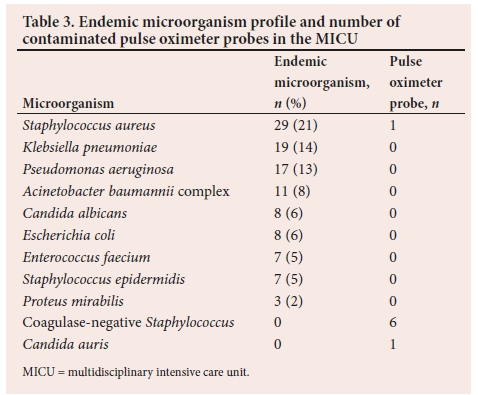
The endemic microorganism profile and the microorganisms grown before decontamination of pulse oximeter probes in the MICU and BICU, respectively, are shown in Tables 3 and 4. A total of 135 and 192 samples were cultured from the MICU and BICU, respectively, between 1 June and 30 September 2018. The tables represent the most common microorganisms isolated from pulse oximeters probes prior to decontamination within both ICUs.
Discussion
HAIs negatively affect patient safety.[31] SA has a high HIV prevalence, which increases the risk of HAI acquisition.[26] Infection control is important to prevent HAI transmission[32] and empirical antibiotic practices that could lead to antibiotic resistance.[33] A possible step toward reducing the risk of acquiring a HAI is the identification of hot spots through target-surface sampling of equipment. Hot-spot identification could lead to the detection of overlooked reservoirs that harbour pathogenic microorganisms.[21]
The internal surfaces of pulse oximeter probes may be overlooked as hot spots for infection, placing ICU patients at risk for HAIs. Pulse oximeter probes contaminated with pathogenic microorganisms in close contact with the skin of susceptible ICU patients are a cause for concern.[34]
In the present study, 91% of the internal surfaces of pulse oximeter probes were contaminated before decontamination. The literature shows microorganism contamination of pulse oximeter probes ranging from 66 to 80%.[3,23,24] In the present study, the higher contamination of pulse oximeter probes and proportion of pathogenic microorganisms identified are difficult to compare with previous studies, which sampled pulse oximeter probes from different wards and ICUs. Furthermore, no previous studies could be identified that sampled pulse oximeter probes within a BICU, which has favourable conditions (a warm environment) for microorganism growth and persistence on environmental surfaces.[35]
Of the contaminated pulse oximeter probes prior to decontamination in this study, 68% isolated 9 different pathogenic microorganisms, with predominantly high-level contamination, namely: Acinetobacter baumannii complex; Klebsiella pneumoniae; Pseudomonas aeruginosa; Staphylococcus aureus; Enterobacter cloacae complex; Candida auris, Escherichia coli; Enterococcus faecalis; and Enterobacter hormaechei. Wilkins[23] sampled pulse oximeter probes from various units in 15 different hospitals in the USA. Of the 44 pulse oximeter probes sampled, 29 (66%) were contaminated, of which only 4 (14%) isolated pathogenic microorganisms, namely: S. aureus, S. haemolyticus, Enterococcus faecalis and Klebsiella oxytoca. Three of these pulse oximeter probes were from ICUs.[23] Davis[3] sampled pulse oximeter probes in an emergency department within a rural hospital in Australia. Of the 15 pulse oximeter probes sampled, 12 (80%) were contaminated, of which only 2 (13%) isolated pathogenic microorganisms, namely Staphylococcus aureus and Bacillus species.[3] Morter et al.[24]sampled various equipment from different wards in a hospital in the UK to isolate sources for a norovirus outbreak. Of the 6 pulse oximeter probes sampled, 4 (67%) were contaminated with the norovirus.[24]
Staphylococcus aureus was the most common endemic microorganism in both ICUs. In this study, however, only two 2 oximeter probes isolated Staphylococcus aureus, each with medium-level contamination. Previous studies have similarly shown only a few pulse oximeter probes to isolate Staphylococcus aureus.[3,23]Nevertheless, considering that Staphylococcus aureus can persistently adhere to environmental surfaces with its peptidoglycan-containing cell wall,[36] and that Parer et al.[21] traced an outbreak-inducing heterogeneous glycopeptide-intermediate Staphylococcus aureus strain to the internal surface of a pulse oximeter probe within a trauma ICU, the mere growth of Staphylococcus aureus on pulse oximeter probes warrants alertness.
In this study, Acinetobacter baumannii complex was the most frequently isolated microorganism prior to decontamination, with the contamination levels ranging from low to high. This microorganism had a high endemic growth within the BICU (28%) and MICU (11%), and was present on 5 of the 6 pulse oximeter probes that isolated 2 pathogens each. Klebsiella pneumonia and Pseudomonas aeruginosa were among the most frequent pathogens endemic to both ICUs, and the third-most frequently isolated microorganisms on the internal surfaces of the pulse oximeter probes. One pulse oximeter probe soiled with blood had high-level contamination of both of these pathogenic microorganisms.
These 3 microorganisms have the potential to cause HAIs in immunocompromised patients.[35-37] Their presence on the internal surfaces of pulse oximeter probes is clinically significant because they are responsible for frequent extensively drug-resistant outbreaks in the BICU at CHBAH (personal communication: Dr Wadula, pathologist-in-charge, clinical and infectious diseases, CHBAH, 6 March 2018), placing strain on last-resort antibiotics such as colistin, and highlighting the emergence of antibiotic-resistant Gram-negative bacilli within SA.[M
In this study, 6 (19%) contaminated pulse oximeter probes isolated 2 different pathogenic microorganisms each, pre decontamination. Additionally, 6 (18%) pulse oximeter probes remained contaminated post decontamination, of which 4 were contaminated with skin commensals, namely: coagulase-negative Staphylococcus and Pseudomonas lautus. Of note, these decontaminated pulse oximeter probes were on patients' fingers pre-decontamination, 3 of which were visibly soiled with blood, and 2 of which had visible cracks on their internal surfaces. These characteristics possibly reflect the build-up of tissue residuals (sebum, blood, debris) on pulse oximeter probes that impede terminal decontamination processes[39] and promote microorganism persistence on environmental surfaces,'41 despite adhering to the manufacturer and hospital guidelines. No previous studies could be identified that investigated the contamination of pulse oximeter probes after decontamination.
Following decontamination, microorganism growth was reduced by 80%. The reduction in contaminated pulse oximeter probes was statistically significant, reflecting the effectiveness of cleaning with a Webcol swab followed by disinfecting with Qualiclean (decontamination processes that are already employed within both ICUs during regular scrub-down processes). While an 80% reduction in contamination is acceptable, 20% contaminated pulse oximeter probes still remains a risk to patients. In this study, attributable causes for remnant contamination might be the cracks and crevices present on pulse oximeter probes. In addition to following manufacturer and unit decontamination guidelines, possible improvements might be to cease using cracked pulse oximeter probes, and to target the crevices around diodes more closely during decontamination processes.
A limitation of this study is that it was done contextually in CHBAH and CMJAH, and therefore cannot be generalised to ICUs in other hospitals. Sensitivity testing could not be done due to funding constraints. Future studies investigating the sensitivity of pathogens isolated from pulse oximeter probes are recommended.
Conclusion
This study has shown that the internal surfaces of pulse oximeter probes may serve as hot spots for an array of pathogens with the potential to cause infection. Cleaning and disinfecting the internal surfaces of pulse oximeter probes should be emphasised, and possibly incorporated into a target-surface sampling protocol in an ICU setting, where it is not practical to have cubicles vacant for prolonged periods while an outbreak is being addressed.
Declaration. This research was done and completed in partial fulfilment of an MMed degree.
Acknowledgements. The authors thank Dr Warren Lowman for his substantial assistance with the microbiology data, Vermaak and Partners Pathologists Laboratory for the efficient processing of samples and the SA Society of Anaesthesiologists Jan Pretorius Research Fund for their financial assistance.
Author contributions. FD: conceived and designed the analysis, collected data, analysed data and wrote the article. JS, HP and MF: proofreading and assessment of research report process.
Funding. SA Society of Anaesthesiologists Jan Pretorius Research Fund.
Conflicts of interest. None.
References
1. Rutala WA, Weber DA. Disinfection and sterilisation in healthcare facilities: An overview and current issues. Infect Dis Clin N Am 2016;30(3):609-637. https://doi.org/10.1016/j.idc.2016.04.002 [ Links ]
2. Andrews FJ, Nolan JP. Critical care in the emergency department: Monitoring the critically ill patient. Emerg Med J 2005;23(7):561-564. https://doi.org/10.1136/emj.2005.029926 [ Links ]
3. Davis C. Blood pressure cuffs and pulse oximeter sensors: A potential source of cross-contamination. Australas Emerg Nurs J 2009;12(3):104-109. https://doi.org/10.1016/j.aenj.2009.03.004 [ Links ]
4. Nandy P, Lucas AD, Gonzalez EA, Hitchins VM. Efficacy of commercially available wipes for disinfection of pulse oximeter sensors. Am J Infect Control 2016;44(3):304-310. https://doi.org/10.1016/j.ajic.2015.09.028 [ Links ]
5. Sharbaugh RJ. Cleaning reusable equipment in the ICU. Crit Care Nurs Q 2001;24(2):48-54. https://doi.org/10.1097/00002727-200108000-00007 [ Links ]
6. Ortega R, Hansen CJ, Elterman K, Woo A. Pulse oximetry. N Engl J Med 2011;364(16):e33-e36. https://doi.org/10.1056/NEJMvcm0904262 [ Links ]
7. Adkinson NF, Bochner BS, Burks AW, et al. Structure of the skin and cutaneous immunology. In: Plager DA, Bieber T, Pittelkow MR, eds. Middelton's Allergy: Principles and Practice. 8th edition. Philadelphia: Elsevier Saunders, 2014:518-539. [ Links ]
8. Dumford DM III, Nerandzic MM, Eckstein BC, Donskey CJ. What is on that keyboard? Detecting hidden environmental reservoirs of Clostridium difficile during an outbreak associated with North American pulsed-field gel electrophoresis type 1 strains. Am J Infect Control 2009;37(1):15-19. https://doi.org/10.1016/j.ajic.2008.07.009 [ Links ]
9. Alfandari S, Gois J, Delannoy PY, et al. Management and control of a carbapenem-resistant Acinetobacter baumannii outbreak in an intensive care unit. Med Mal Infect 2014;44(5):229-231. https://doi.org/10.1016/j.medmal.2014.03 [ Links ]
10. Harnett SJ, Allen KD, Macmillan RR. Critical care unit outbreak of serratia liquefaciens from contaminated pressure monitoring equipment. J Hosp Infect 2001;47(4):301-307. https://doi.org/10.1053/jhin.2001.0941 [ Links ]
11. Devine J, Cooke R, Wright E. Is methicillin-resistant Staphylococcus aureus (MRSA) contamination of ward-based computer terminals a surrogate marker for nosocomial MRSA transmission and handwashing complaince? J Hosp Infect 2001;48(1):72-75. https://doi.org/10.1053/jhin.2001.0955 [ Links ]
12. De Gialluly C, Morange V, De Gialluly E, Loulergue J, van der Mee N, Quentin R. Blood pressure cuff as a potential vector of pathogenic micro-organisms: A prospective study in a teaching hospital. Infect Control Hosp Epidemiol 2006;27(9):940-943. https://doi.org/10.1086/507284 [ Links ]
13. Lestari T, Ryll S, Kramer A. Microbial contamination of manually reprocessed, ready-to-use ECG lead wire in intensive care units. GMS Hyg Infect Control 2013;8(1):1-7. https://doi.org/10.3205/dgkh000207 [ Links ]
14. Maluf M, Maldonado A, Bercial M. Stethoscope: A friend or an enemy? Sao Paulo Med J 2002;120(1):13-15. https://doi.org/10.1590/S1516-31802002000100004 [ Links ]
15. Uneke CJ, Ijeoma PA. The potential for transmission of hospital-acquired infections by non-critical medical devices: The role of thermometers and blood pressure cuffs. World Health Popul 2011;12(3):5-12. https://doi.org/10.12927/whp.2011.22098 [ Links ]
16. Walsh E, Ben-David D, Ritter M, Mechrefe A, Mermel L, DiGiovanni C. Microbial colonisation of tourniquets used in orthopaedic surgery. Orthopaedics 2006;29(8):709-713. [ Links ]
17. Runner J. Bacterial and viral contamination of reusable sharps containers in a community hospital setting. Am J Infect Control 2007;35(8):527-530. https://doi.org/10.1016/j.ajic.2006.09.017 [ Links ]
18. Gray J, McNicholl B, Webb H, Hogg G. Mice in the emergency department: Vector for infection or technological aid? Eur J Emerg Med 2007;14(3):160-162. https://doi.org/10.1097/MEJ.0b013e3280bef922 [ Links ]
19. Luckey J, Barfield R, Eleazer P. Bacterial count comparisons on examination gloves from freshly opened boxes and from examination gloves before treatment v. after dental dam isolation. J Endod 2006;32(7):646-648. https://doi.org/10.1016/j.joen.2005.09.017 [ Links ]
20. Tunc K, Olgun U. Microbiology of public telephones. J Infect 2006;53:140-143. https://doi.org/10.1016/j.jinf.2005.10.022 [ Links ]
21. Parer S, Lotthe A, Chardon P, Poncet R, Jean-Pierre H, Jumas-Bilak E. An outbreak of heterogeneous glycopeptide-intermediate Staphylococcus aureus related to a device source in an intensive care unit. Infect Control Hosp Epidemiol 2012;33(2):167-174. https://doi.org/10.1086/663703 [ Links ]
22. Pusch T, Kemp D, Trevino S, et al. Controlling outbreak of vancomycin-resistant Enterococcus faecium among infants caused by an endemic strain in adult inpatients. Am J Infect Control 2013;41(1):51-56. https://doi.org/10.1016/j.ajic.2012.01.034 [ Links ]
23. Wilkins MC. Residual bacterial contamination on reusable pulse oximetry sensors. Respir Care 1993;38(11):1155-1160. [ Links ]
24. Morter S, Bennet G, Fish J, et al. Norovirus in the hospital setting: Virus introduction and spread within the hospital environment. J Hosp Infect 2011;77(2):106-112. https://doi.org/10.1016/j.jhin.2010.09.035 [ Links ]
25. Rode AH, Cox SG, Numanoglu A, Berg AM. Burn care in South Africa: A micro cosmos of Africa. Pediatr Surg Int 2014;30(7):699-706. https://doi.org/10.1007/s00383-014-3519-5 [ Links ]
26. Crowther-Gibson P, Govender N, Lewis DA, et al. Part IV: Human infections and antibiotic resistance. S Afr Med J 2011;101(8):567-578. https://doi.org/10.7196/SAMJ. 5102 [ Links ]
27. Kravitz M. Immune consequences of burn injury. AACN Clin Issues Crit Care Nurs 1993;4(2):399-413. https://doi.org/10.4037/15597768-1993-2017 [ Links ]
28. Lee D, Benson CA, Lewis CE, Grunfeld C, Scherzer R. Prevalence and factors associated with dry skin in HIV infection: The FRAM study. AIDS 2007;21(15):2051-2057. https://doi.org/10.1097/QAD.0b013e3282eea51a [ Links ]
29. Elfaki ME. Immunosuppression induced by HIV infection. Biol Med 2014;6(3):111-112. https://doi.org/10.1097/00006247-200112000-00016 [ Links ]
30. Gilmore GK. Infection control advances decrease patient and staff risk. Nurse Manage 2001;32(12):51-53. https://doi.org/10.1097/00006247-200112000-00016 [ Links ]
31. World Health Organization World Alliance for Patient Safety. Forward programme 2005. Geneva: WHO, 2004. [ Links ]
32. Huang SS, Datta R, Platt R. Risk of acquiring antibiotic-resistant bacteria from prior room occupants. Arch Intern Med 2006;166(18):1945-1951. https://doi.org/10.1001/archinte.166.18.1945 [ Links ]
33. Ventola CL. The antibiotic resistance crisis. Part 2: Management strategies and new agents. P T 2015;40(5):344-352. [ Links ]
34. Brady RRW, Kalima P, Damani NN, Wilson RG, Dunlop MG. Bacterial contamination of hospital bed-control handsets in a surgical setting: A potential marker of contamination of the healthcare environment. Ann R Coll Surg Engl 2007;89(7):656-660. https://doi.org/10.1308/003588407X209347 [ Links ]
35. Carroll KC, Hobden JA. Pseudomonads and Acinetobacter. In: Carroll KC, Hobden JA, Miller S, et al., eds. Jawetz, Melnick, & Adelberg's Medical Microbiology. 27th edition. New York: McGraw-Hill, 2016. [ Links ]
36. Carroll KC, Hobden JA. The Staphylococci. In: Carroll KC, Hobden JA, Miller S, et al., eds. Jawetz, Melnick, & Adelberg's Medical Microbiology. 27th edition. New York: McGraw-Hill, 2016. [ Links ]
37. Carroll KC, Hobden JA. Enteric Gram-negative rods (Enterobacteriaceae). In: Carroll KC, Hobden JA, Miller S, et al., eds. Jawetz, Melnick, & Adelberg's Medical Microbiology. 27th edition. New York: McGraw-Hill, 2016. [ Links ]
38. Brink A, Feldman C, Richards GA, Moolman J, Senekal M. Emergence of extensive drug resistance (XDR) among Gram-negative bacilli in South Africa looms nearer. S Afr Med J 2008;98(8):586-592. [ Links ]
39. Alfa MJ. Monitoring and improving the effectiveness of cleaning medical and surgical devices. Am J Infect Control 2013;41(2013):S56-S59. https://doi.org/10.1016/j.ajic.2012.12.006 [ Links ]
 Correspondence:
Correspondence:
F Desai
farriels@icloud.com
Accepted 9 September 2019
Contribution of study
• This study identifies internal surfaces of pulse oximeter probes as reservoirs for infection in intensive care units (ICUs), particularly in a burns ICU setting, pinpointing one of many sources of hospital-acquired infections within ICU cubicles.
• The study emphasises the need to clean the internal surfaces of pulse oximeter probes (whether visibly soiled or not) prior to disinfection.


{kind=link}
{kind=link}