










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouthern African Journal of Critical Care (Online)
versão On-line ISSN 2078-676X
versão impressa ISSN 1562-8264
South. Afr. j. crit. care (Online) vol.34 no.1 Pretoria Jul. 2018
http://dx.doi.org/10.7196/sajcc.201.v34i1.339
ARTICLE
Exploring the challenges with infection control practices among managers in intensive care units in South Africa
S MahomedI; J De BeerII
IMB ChB, MMed; School of Laboratory Medicine and Medical Sciences, College of Health Sciences, University of KwaZulu-Natal, Durban, South Africa
IIPhD; College of Nursing, King Saud bin Abdul Aziz University for Health Sciences, Jeddah, Saudi Arabia
ABSTRACT
BACKGROUND. The prevention of healthcare-associated infections has become a health priority globally. Patients in intensive care units (ICUs) are at high risk of acquiring these infections, and infection control is particularly important in this environment. Hospital infection control managers as well as ICU nurses and clinical managers have a vital role to play in ensuring good infection control practices within the ICUs.
OBJECTIVE. To explore the challenges with infection control practices among managers in ICUs in South Africa.
METHODS. An explorative qualitative design was used. Semi-structured interviews were conducted with 11 nurse intensive care managers, 6 clinical intensive care managers, and 5 hospital infection control managers. Content analysis was used to identify themes and sub-themes.
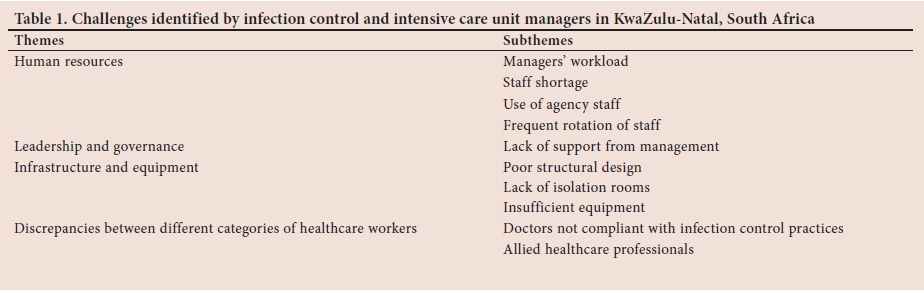
RESULTS. Four themes were identified from the data: challenges with human resources, leadership and governance, infrastructure and equipment, and discrepancies between different categories of healthcare workers. Infection control and nurse managers felt overburdened with work responsibilities which took their time away from infection control in the ICU. Shortage of clinical and nursing staff , insufficient isolation rooms and equipment also presented challenges to implementing adequate infection control measures. Many participants viewed doctors as not being adherent to infection control practices.
CONCLUSION. We identified modifiable challenges to infection control in the intensive care setting. Strategies such as ongoing and regular in-service training on infection control for all cadres of healthcare workers is one of the interventions that can be applied to improve infection control in ICUs. The issue of staff shortages and inadequately trained staff must be addressed at a provincial and national level. It is imperative that hospital managers work with their staff to develop strategies to overcome the challenges in implementing and maintaining good infection practices in ICUs.
The prevention of healthcare-associated infections (HAI) has become a health priority globally. Multidrug-resistant organisms causing HAI result in high patient mortality and morbidity is becoming more frequent in healthcare facilities, particularly in intensive care units (ICUs).[1] Infection control policies and guidelines to mitigate the risk of acquiring HAI are an integral component of all areas in healthcare facilities.
Infection control practices include hand hygiene, isolation precautions, environmental cleaning, bundles for the prevention of device-associated infections, infection prevention committees, antimicrobial stewardship programmes, and continuing staff education programmes.[2,3] ICUs are one of the busiest and most demanding environments within a healthcare facility. Infection control policies and guidelines should be adhered to at all times within ICUs, as patients in these units are often immunocompromised, have breaches in their first line of defence, and are therefore more susceptible to acquiring infections.[4] The continuous care of critically ill patients who require specialised care necessitates a 1:1 nurse to patient ratio, and clinicians with expertise in intensive care medicine.[5]
In South Africa (SA), in addition to an under-resourced public health sector, the high burden of communicable and non-communicable diseases, injuries and violence,[6] places more demand on intensive care services. ICUs are frequently full, resulting in patients having to wait for an ICU bed. Research has shown that work pressures and a non-conducive working environment in the ICU can result in sub-optimal infection control.[7] All healthcare workers are responsible for infection control practices, but managers have to ensure adherence to infection control policies and guidelines. In the ICU, nurse managers are responsible for the maintenance of efficient and effective management of the unit.
The present study was one part of a comprehensive assessment of infection control practices in ICUs. The aim of the research was to explore the challenges with infection control experienced by hospital infection control managers and nursing and clinical managers of the ICUs.
Methods
Study design and setting
This research was conducted using an explorative and qualitative design. The study setting included 6 public-sector ICUs and 5 private-sector ICUs in the eThekwini Health District of KwaZulu-Natal, SA.
Study population
The study population comprised hospital infection control managers and nursing and clinical managers of the ICUs. Each ICU is managed by a nurse manager. A clinical manager is the medical practitioner who is responsible for an ICU and could be a cardiothoracic surgeon, a neurosurgeon, anaesthetist or a surgeon with critical care expertise. Only public-sector ICUs had clinical managers. The infection control manager was responsible for co-ordination of infection control activities within a healthcare facility. We included managers only as they represent a homogenous sample of healthcare workers with similar clinical and administrative duties.
An expert purposive sampling approach was used. The study sample consisted of 22 participants, who included 11 ICU nurse managers, 6 ICU clinical managers and 5 infection control managers.
Data collection
Semi-structured interviews were conducted with each participant by the principal investigator, who used a set of questions and probes. The interviews were conducted at convenient times for participants, between June and December 2014, in a private area within the hospital. Interviews were transcribed verbatim. The main interview questions included: (i) What are the factors that promote adherence to infection control norms/guidelines in the ICU?; (ii) Do you feel that the hospital management is supportive or facilitates the process of improving infection control in the ICU?; (iii) What are some of the challenges with regard to infection prevention and control in the ICU?; and (iv) Do you think infection control practices differ among doctors and nurses?
Data analysis
Data analysis followed an iterative approach using the framework described by Srivastava and Hopwood.[8] According to this framework, data analysis in qualitative research is not a repetitive process but rather reflective. Three questions guided the data analysis process: 'What is the data telling me?'; 'What is it that I want to know?'; and 'What is the dialectical relationship between what the data is telling me and what I want to know?'. Thereafter, a content analysis approach was used by the principal investigator to identify themes and subthemes. The qualitative software package NVivo version 11 (QSR International, Australia) was used. Academic rigour was followed using four principles.[9]
1. Credibility
Peer debriefing was used for external validation of the emerging data. Member checking was also used as this is regarded as the most important technique for establishing credibility.[9] This involved the researcher providing feedback about the emerging data and interpretations to participants to ensure it was a true reflection of their reactions. The study participants did not suggest any changes.
2. Dependability
A dependability audit was completed which involved using an expert in critical care medicine and an expert in infection control to review the transcripts and field notes that the researcher used during this study.
3. Confirmability
A confirmability trail was also established by recording the research activities over time so that others can follow the research process undertaken.
4. Transferability
The researchers provided sufficiently thick descriptions by providing detailed descriptions of the research settings, participants, data collection methods and time frame of data collection described above. This was done to afford readers a proper understanding of the phenomenon at hand, enabling them to compare the phenomenon described in this report with those that they might observe in other studies.
Ethical considerations
Permission to conduct the study was obtained from each hospital manager and the KwaZulu-Natal Department of Health. Ethics approval was obtained from the Biomedical Research and Ethics Committee at the University of KwaZulu-Natal (ref. no. BE53/14). The purpose of the study was explained to each participant before obtaining informed consent. Confidentiality was maintained by not recording the participant's name on the interview sheet.
Results
All the nursing and infection managers were female and all the clinical managers were male. The experience as nursing managers ranged from 11 months to 11 years, and 2 to 7 years for clinical managers. There were similar challenges noted in both the private and public sector (Table 1).
Human resources
There were numerous issues related to the lack of sufficient human resources and infection control. A common challenge cited by all the nurse managers in the public ICUs was the demanding workload that they faced which often made it difficult to give sufficient attention to infection control activities. Administrative duties were identified as being time-consuming. The nurse managers reported that they were under pressure to provide various reports to their managers, prepare work rosters and ensure the smooth running of the ICU.
'We have too many other responsibilities ... there should be one person free to monitor infection control in the ICU! (Nurse manager 1)
'There is too much paperwork for us. Reports and stats have to be sent monthly! (Nurse manager 2)
The infection control managers also voiced similar challenges in that they had many responsibilities throughout the hospital and they were unable to do regular infection control inspections in all the hospital wards.
'Everything in the hospital related to cleanliness becomes our responsibility! (Infection control manager 1)
'There are too many meetings to attend sometimes...we cannot do daily rounds! (Infection control manager 2)
'We have so many things to see to..! (Infection control manager 3)
Nurse managers in both sectors reported that although the nursing staff allocated to the ICU met the 1:1 nurse patient ration for each shift, in practice this did not occur. There were various reasons cited for this lack of nursing staff, including nurses being on leave and attending training. The shortage of nursing staff was cited as a challenge to infection control in all ICUs. Only one ICU had a full complement of critical care trained nurses.
We have a staff shortage, especially at night...sometimes only six nurses working on a night shift and we have ten beds in total! (Nurse manager 3)
In one private sector ICU, the use of nursing staff through recruitment agencies was cited as a major challenge to maintaining infection control standards in the ICU.
Agency staff do not have the same loyalty and vigilance as the other nursing staff...some agency staff don't care about infection control practices..! (Nurse manager 4)
The clinical managers described the frequent rotation of different doctors through the ICU and shortage of trained critical care physicians as a challenge.
'There is no stable workforce in the ICU except for consultants. Every 6 weeks there are new medical officers and registrars...it is difficult to constantly orientate on ICU specific infection control issues.! (Clinical manager 1)
'Staffing is an issue...eight of our doctors are trainees! (Clinical manager 2)
Leadership and governance
Although some of the participants viewed the hospital leadership and governance as being supportive and facilitating the improvement of infection control in the ICU, some participants reported differently.
'Hospital management is not supportive, only the infection control manager. Management needs to be more visible! (Nurse manager 5)
'We don!t deal with management. The infection control manager relates with hospital management. They are not fully supportive because they have been away from the bedside and don!t know the latest. they also don!t release what is needed for infection control.! (Nurse manager 6)
Infrastructure and equipment
In the public ICUs, issues with infrastructure and equipment were cited as important obstacles to infection control. The design of one ICU was such that it opened into a medical high care ward that often housed patients with multidrug-resistant tuberculosis (MDR-TB), putting staff and other patients at risk.
Two of our nurses have been diagnosed with MDR-TB. Medical high care need to be separated from ICU! (Clinical manager 3)
The lack of isolation rooms was a challenge cited in three ICUs, and two of these ICUs also reported a lack of sufficient new equipment.
'We do not have a functional isolation unit...this is a big challenge for us! (Clinical manager 3)
' There is no isolation room. Currently we have a patient with MDR Acinetobacter in the middle of the ward! (Nurse manager 5)
'Many of our patients are immunocompromised and there is a high burden of patients with TB...we have insufficient isolation rooms! (Nurse manager 7)
Furthermore, it was reported that the shortage of equipment often led to sharing of equipment between patients, which compromised infection control.
'We have old cardiac monitors. We received four new monitors, but this is not enough as we have to move the monitors from bed to bed..! (Nurse manager 3)
Discrepancies between different categories of healthcare workers
Except for one clinical manager and one nursing manager, all other participants reported that doctors were less vigilant than nurses with regard to infection control practices. Examples of the deficiencies in practices included not using gloves, having to be reminded to wash hands and not adhering to aseptic protocols when inserting invasive lines. One of the clinical managers also noted that medical students do not receive training on infection control in their undergraduate training; nor is infection control training included in postgraduate training.
'Nurses take infection control more seriously...there is minimal in-service training on infection control for doctors.! (Clinical manager 2)
'Doctors do not attend in-service and do not comply with infection prevention and control.! (Nurse manager 3)
Most doctors think infection control is a nurse thing and it doesn't concern them.! (Nurse manager 8)
Our doctors do not always adhere to handwashing..! (Infection control manager 4)
In addition, nurse managers in the private sector reported that they could not tell doctors what to do and that they had to deal with a variety of specialists, each with their own approach to patient care, and they were unable to tell the doctor if he was doing something that was in disagreement with infection control guidelines.
'Doctors are often in a hurry...do not put on correct gear when inserting a central line.! (Nurse manager 7)
Sometimes doctors do not practise hand hygiene between patients! (Nurse manager 9)
Doctors don't follow the handwashing steps...nurses too sometimes! (Nurse manager 10)
'It is difficult to tell doctors when they don't do the correct thing! (Nurse manager 11)
Patients in ICUs often require care from other clinicians and allied healthcare professionals, such as physiotherapists and occupational therapists. Additionally, radiographers and paramedics also enter the ICU. The managers reported that these healthcare workers did not receive the same infection control training as the ICU staff and therefore did not always adhere to infection control principles and practices. In one public sector ICU, there was an issue with non-clinical staff not being aware of infection control and driving a cart through the ICU to deliver stock. None of the private sector ICUs reported similar challenges.
'Non-ICU staff do not practice infection control...stock is driven into the ICU (Clinical manager 1)
'There are high volumes of people in ICU - nursing students, physiotherapists, emergency services - this is a challenge to infection control as these staff are not always aware of infection control in the ICU.' (Nurse manager 8)
A lot of healthcare workers come into ICU - it is difficult to monitor their practice'. (Nurse manager 11)
Discussion
Participants highlighted numerous challenges in effecting adequate infection control practices within ICUs. The high workload encountered by nurse managers has been cited in ICU settings and departments within other healthcare facilities. High workloads can lead to burnout, and decreased work productivity and have an impact on the rest of the staff within a department.[7] Interestingly, a high workload was not reported as a challenge by nurse managers working in the private sector ICUs. This may be due to different responsibilities allocated to nurse managers in each of the sectors, and/or to better staffing in the private sector, and/or different organisational structure of the hospitals.
Our finding of a shortage of nursing and clinical staff has been reported in other ICU settings in SA.[10,11] According to de Beer et al., [12] only 25% of nurses working in ICUs in SA are adequately trained. In ICUs, staff shortages and inadequately trained staff can result in poor patient outcomes as these patients require ongoing care and monitoring.[13,14] Furthermore, a staff shortage places an additional burden on the staff who are available which can lead to physical and psychological problems for the healthcare workers. Only one of the ICUs had a full complement of nurses with critical care training. The use of agency nurses to alleviate a staff shortage introduced new challenges to ICUs. Nurse managers felt that, because agency nurses were not part of the permanent staff pool, they did not adhere to infection control policies in ICUs. It has also been reported that agency staff do not display the same commitment as permanent staff, and that their patient care is sub-standard.[12] These challenges can impact negatively on infection control practices and patient care in the ICU and warrant further investigation, particularly if the problem is linked to the use of agency staff.
Although the infection control manager was seen as the link between ICU and hospital management, some managers felt that hospital management was not supportive. Hospital executive managers should endeavour to meet with staff regularly to improve staff morale and facilitate a work environment where unit managers feel supported in their duties. Hospital managers have a moral and ethical obligation to ensure a high quality of patient care and are in a prime position to mandate policies, procedures and organisational climates.[15] It is therefore important that hospital management is seen to be actively involved in infection control and not merely delegating the responsibility to an infection control manager, in keeping with Duerden's recommendation that compliance with infection control should be seen from 'board to ward'.[16]
The challenges around infrastructure and equipment are important factors in resource-constrained healthcare settings. Sufficient equipment to support ventilated patients, adequate spacing and isolation rooms are integral to reducing the risk of HAI to patients in ICUs. The mix of patients infected with easily transmissible drug-resistant organisms with immunocompromised patients is not permitted, and isolation rooms should be available in all ICUs.[5]
The discrepancy in infection control knowledge and practice, and attribution of specific infection control responsibilities to certain cadres of healthcare workers, has been reported in other health settings.[17,18-Nurse managers, particularly in the private sector, perceived difficulty in communicating with doctors regarding infection control. This challenge may be ascribed to the difference in the way ICUs are managed in public and private sectors. In the public sector, ICUs are closed units managed by physicians with specialist training in intensive care medicine, whereas private sector ICUs are open units and any doctor can admit and manage a patient in the unit. In the public sector, clinical and nurse managers have good working relationships and are able to discuss inter-professional issues. The hierarchy of leadership and lines of communication need to be better explained and enforced in the private sector, particularly for doctors. The lack of training on infection control in the undergraduate and postgraduate medical curriculum was highlighted and warrants further investigation and action.
Study limitations
One of the limitations of this research was that it is was conducted in one health district in KwaZulu-Natal and may not reflect the challenges faced by ICU managers in other districts. However, given the similar general challenges facing the health sector in SA, it is likely that many of these challenges will apply. Some participants viewed the interview process as an outlet for the issues they felt were not being addressed by hospital management and might have expressed these issues more vociferously.
Conclusion
This research has identified modifiable challenges to infection control practices within ICUs. Ongoing and regular in-service training on infection control for all cadres of healthcare workers is one of the interventions that can be applied to improve infection control practices in the ICU. The issues of staff shortages and inadequately trained staff must be addressed at a provincial and national level. It is imperative that hospital managers work with their staff to develop strategies to overcome the challenges in implementing and maintaining good infection practices in the ICU, and throughout health facilities. Further research into how the challenges identified affect patient care should be explored.
Acknowledgements. We would like to thank all managers for taking the time to participate in this study. We would also like to acknowledge Professor P Moodley, Professor AW Sturm, and Dr SE Knight for their intellectual contribution to the research.Author contributions. SM conceptualised the study design, collected data and drafted the manuscript. SM and JdB contributed to data analysis and interpretation and critically revising all versions of the article.Funding. This research was supported by the College of Health Sciences at the University of KwaZulu-Natal.Conflicts of interest. None.
Acknowledgements. We would like to thank all managers for taking the time to participate in this study. We would also like to acknowledge Professor P Moodley, Professor AW Sturm, and Dr SE Knight for their intellectual contribution to the research.
Author contributions. SM conceptualised the study design, collected data and drafted the manuscript. SM and JdB contributed to data analysis and interpretation and critically revising all versions of the article.
Funding. This research was supported by the College of Health Sciences at the University of KwaZulu-Natal.
Conflicts of interest. None.
References
1. Medina E, Pieper DH. Tackling threats and future problems of multidrug-resistant bacteria. In: Stadler M, Dersch P, eds. How to Overcome the Antibiotic Crisis: Facts, Challenges, Technologies and Future Perspectives. Cham: Springer International Publishing, 2016:3-33. [ Links ]
2. Gandra S, Ellison RT. Modern trends in infection control practices in intensive care units. J Intensive Care Med 2014;29(6):311-326. [ Links ]
3. Osman MF, Askari R. Infection control in the intensive care unit. Surg Clin North Am 2014;94(6):1175-1194. https://doi.org/10.1016/j.suc.2014.08.011 [ Links ]
4. Fraise AP, Bradley C. Ayliffe's Control of Healthcare-associated Infection. 5th ed. London: Hodder Arnold, 2009. [ Links ]
5. Valentin A, Ferdinande P. Recommendations on basic requirements for intensive care units: Structural and organizational aspects. Intensive Care Med 2011;37(10):1575-1587. https://doi.org/10.1007/s00134-011-2300-7 [ Links ]
6. Pillay-van Wyk V, Msemburi W, Laubscher R, et al. Mortality trends and differentials in South Africa from 1997 to 2012: Second national burden of disease study. Lancet Glob Health 2016;4(9):e642-e653. https://doi.org/10.1016/s2214-109x(16)30113-9 [ Links ]
7. Cimiotti JP, Aiken LH, Sloane DM, Wu ES. Nurse staffing, burnout, and healthcare-associated infection. Am J Infect Control 2012;40(6):486-490. https://doi.org/10.1016/j.ajic.2012.02.029 [ Links ]
8. Srivastava P, Hopwood N. A practical iterative framework for qualitative data analysis. Int J Qual Methods 2009;8(1):76-84. https://doi.org/10.1177/160940690900800107 [ Links ]
9. Lincoln YS, Guba EG, Pilotta JJ. Naturalistic Inquiry. Beverly Hills: SAGE Publications, 1985. [ Links ]
10. Matlakala MC, Bezuidenhout MC, Botha AD. Challenges encountered by critical care unit managers in the large intensive care units. Curationis 2014;37(1):1146. https://doi.org/10.4102/curationis.v37i1.1146 [ Links ]
11. Naidoo K, Singh J, Lalloo U. A critical analysis of ICU/HC beds in South Africa: 2008 - 2009. S Afr Med J 2013;103(10):751-753. https://doi.org/10.7196/samj.6415 [ Links ]
12. De Beer J BP, Bhengu BR. Intensive care nursing in South Africa. S Afr J Crit Care Care 2011;27(1):6-10. [ Links ]
13. West E, Barron DN, Harrison D, Rafferty AM, Rowan K, Sanderson C. Nurse staffing, medical staffing and mortality in intensive care: An observational study. Int J Nurs Stud 2014;51(5):781-794. https://doi.org/10.1016/j.ijnurstu.2014.02.007 [ Links ]
14. Lee A, Cheung YSL, Joynt GM, Leung CCH, Wong WT, Gomersall CD. Are high nurse workload/ staffing ratios associated with decreased survival in critically ill patients? A cohort study. Ann Intensive Care 2017;7(1):46. https://doi.org/10.1186/s13613-017-0269-2 [ Links ]
15. Parand A, Dopson S, Renz A, Vincent C. The role of hospital managers in quality and patient safety: A systematic review. BMJ Open 2014;4(9):e005055. https://doi.org/10.1136/bmjopen-2014-005055 [ Links ]
16. Duerden BI. Responsibility for managing healthcare-associated infections: Where does the buck stop? J Hosp Infect 2009;73(4):414-417. https://doi.org/10.1016/j.jhin.2009.06.027 [ Links ]
17. Stein AD, Makarawo TP, Ahmad MFR. A survey of doctors' and nurses' knowledge, attitudes and compliance with infection control guidelines in Birmingham teaching hospitals. J Hosp Infect 2003;54(1):68-73. https://doi.org/10.1016/s0195-6701(03)00074-4 [ Links ]
18. Shah N, Castro-Sánchez E, Charani E, Drumright LN, Holmes AH. Towards changing healthcare workers' behaviour: A qualitative study exploring non-compliance through appraisals of infection prevention and control practices. J Hosp Infect 2015;90(2):126-134. https://doi.org/10.1016/j.jhin.2015.01.023 [ Links ]
 Correspondence:
Correspondence:
S Mahomed
mahomeds@ukzn.ac.za
Accepted 23 February 2018


{kind=link}