










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Journal of Information Management
versão On-line ISSN 1560-683X
versão impressa ISSN 2078-1865
SAJIM (Online) vol.25 no.1 Cape Town 2023
http://dx.doi.org/10.4102/sajim.v25i1.1622
ORIGINAL RESEARCH
Success factors for evidence-based healthcare practice adoption
Lovemore Motsi; Bester Chimbo
School of Computing, College of Science, Engineering and Technology, University of South Africa, Pretoria, South Africa
ABSTRACT
BACKGROUND: Evidence-based health policies are widely acknowledged as being essential for attaining ongoing improvements in health outcomes. This study represents a theoretical model to test and identify to identify the key drivers for adopting evidence-based healthcare practice (EBHP
OBJECTIVES: The goal of this study was to investigate the critical success factors for the adoption of evidence-based healthcare at a South African public hospital
METHODS: Medical healthcare professionals were surveyed using a questionnaire developed by the researcher. The results were analysed with SPSS 23 and AMOS. A hypothetical model based on updated (D&M) IS Success Model, Technology, Organization and Environment framework (TOE) as well as Technology Acceptance Model (TAM) was developed and analysed using structural equation modelling (SEM
RESULTS: The findings of this study indicate that EHR is crucial and the main construct influencing the adoption of EBHP. The findings of this study indicated a positive relationship between the construct electronic health records (EHR) with medical error reduction (MER), information quality (IQ) and knowledge quality (KQ), all showed a strong positive correlation towards the adoption of EBHP
CONCLUSIONS: Better coordination of patient care (BCP) typically results in lower health care costs. The results also show that using EBHP improves the accuracy of disease diagnosis and treatment, which lowers the burden of disease
CONTRIBUTION: The developed framework will help healthcare systems that are strapped for money, particularly in developing countries
Keywords: medical healthcare professionals; evidence-based healthcare practice (EBHP); better coordination of patient care (BCP); diagnosis and treatment of diseases; medical error reduction; information quality; knowledge quality.
Introduction
The most recent technology, the Internet of Things (IoT), is essential to the digitalisation of the healthcare sector (Boyes et al. 2018). Furthermore, the adoption of connected healthcare is accelerating globally over the past two decades as healthcare IoT cases gain momentum (Shah & Chircu 2018). The impact of leveraging digitalisation across various levels of processes, products and services demonstrates that the healthcare industry is one of the significantly revolutionised sectors (Kumar, Verma & Bharti 2020; Moro Visconti & Morea 2020). Furthermore, the electronic medical record (EMR) represents a change from the antiquated practice of keeping paper records to computerised electronic data management. It is now acknowledged as a contemporary productivity, efficiency and effectiveness in medical care facilitation (Adeleke et al. 2014; Sockolow et al. 2014). In addition, it is supported by systems for Internet networks, providing flexibility in the ability to transfer information, bring about change in the field of healthcare and enhancing patient health outcomes. Nene (2015) claims that a patient at South Africa's King Edward VIII Hospital had to wait more than eight hours before receiving treatment for diarrhoea because staff members needed to find his medical file in the file room. Medical records can occasionally be difficult to locate in the filing department as a result of, among other things, records being lost or misfiled (Nene 2015). These records are occasionally simply misplaced by healthcare providers and later discovered at their offices. In addition, the duplicate record would exist because the original record would have been changed by the time the replacement record was found.
In another study by Marutha (2011), doctors were prevented from operating on a patient at Nkhesani Hospital in Limpopo province, South Africa, because the patient's medical records were missing. The patient's left leg was partially paralysed as a result of a car accident in 2005. According to the report, the doctors needed the missing file, which contained information about the patient's accident, health problems and illness, in order to trace the history of the injuries before the patient could have surgery. Unfortunately, the patient's diabetes records were the only part of the medical history that could be accessed. According to the Limpopo Department of Health and Social Development, which intervened and provided clarification in this case, the hospital had a minor file mix-up. It is evident from the aforementioned cases that when patient health records in paper format are missing, patients face significant challenges and risk their lives, which may result in death. The medical institution could also be harmed by this. Duplicate data is regarded as poor and untrustworthy patient data and is a concern for many organisations and systems, according to Bardach, Real and Bardach (2017). Another disadvantage of paper-based medical records is that data cannot be shared by many users because the physical document is often only read in one place (Dowding, Turley & Garrido 2015).
Clinical decision-making is thought to be improved by the integration of various information tools into EMR, such as test ordering, electronic prescriptions, decision support systems, digital imaging and telemedicine. Furthermore, integrating such information into standard clinical practice might encourage the use of a secure and effective healthcare system (Sockolow, Bowles & Adelsberger 2014). Access to patients' vital health information from various providers, which greatly enhances care coordination and healthcare practice efficiency, is one of the main advantages of EMR that is stated (Jawhari, Keenan & Zakus 2016). Several of these advantages have been supported by earlier studies (Kruse, Mileski & Alaytsev 2015). In the end, the push for electronic health records (EHR) may make it possible for patients to access and possibly transfer their own medical data, giving them more control over their own care and management of their medical data (Chao et al. 2013; King et al. 2014). Furthermore, because of the complexity of healthcare delivery, conventional decision-making methods for implementing new technologies based on trustworthy and predictable systems are inappropriate (Kuziemsky 2016). This study's aim was to investigate the critical success factors that influence the adoption of evidence-based healthcare practice (EBHP) in a South African public hospital. A theoretical framework based on a model based on the updated Information Systems (IS) Success Model (D&M) model, the Technology-Organisation-Environment (TOE) framework and Technological Acceptance Model (TAM) was developed to assist in identifying the critical success factors. Structural equation modelling (SEM) was used to test and validate the conceptual framework using survey data gathered at Dr George Mukhari Academic hospital.
The next section will discuss in greater detail on the theories that were used to develop the conceptual framework, the constructs and the formulation of the hypothesis based on the framework.
Conceptual framework and formulation of hypothesis
This study suggests a hybrid model for the adoption of EBHP. The hybrid model is based on updated versions of Davis, Bagozzi and Warshaw (1989), the TAM and the TOE, as well as DeLone and McLean's IS Success Model (DeLone & McLean 2003; Tornatzky & Fleischer 1990). Technology Acceptance Model was chosen for this study because it concentrates on how individual users perceive technology and assesses how those perceptions might affect their behavioural intention. The goal of this study is to develop a framework for EBHP at a South African public hospital. For this purpose, the factors that contribute to the adoption of EBHP will be analysed using an integration of two theories namely the TAM and TOE into D&M IS Success Model, which is the main underpinning theory in this study.
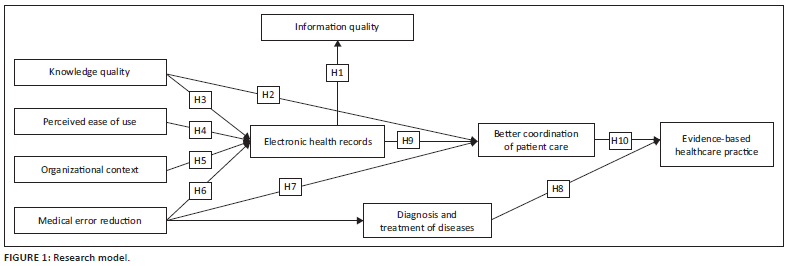
The D&M IS Success Model assisted in finding the individual level acceptance of the new technology like EHR system, whereas the TOE model was a logical extension of D&M IS Success Model from an individual perspective to organisational factors. While D&M IS Success Model and TOE frameworks helped to understand the decision method for technology adoption and some aspects of implementation, TAM theory provided the usability factor from the individual user perspective. For this study, the EBHP construct was used in place of the Net-benefits construct from the D&M IS Success Model. This construct is a dependent variable in the proposed research paradigm (see Figure 1), while the independent variables are medical error reduction (MER), information quality (IQ), knowledge quality (KQ), perceived ease of use and organisational context.
The influence of EHR on medical mistake reduction, IQ, KQ, improved patient coordination, disease diagnosis and treatment, perceived usability, technological context and organisational context were all examined in this study. The findings highlight the importance of improving patient responsiveness and orientation to expat demands in South Africa's healthcare system.
In the section that follows, we will discuss in greater detail how the constructs from TAM and TOE that were incorporated into the D&M IS Success Model as well as how they relate to each other. These relationships are shown in Figure 1: hypothesis research model.
Electronic health records construct
To incorporate evidence-based knowledge into patient treatment, the proper information must be made available at the appropriate time (Mitchell 2019). The optimal time to make a diagnosis may be when attending to a patient at their bedside or during any other step of the examination and treatment process. Doctors who are already under pressure to treat more patients in less time are less likely to hunt for evidence to back their decisions when a search disturbs their workflow (Grumbach & Bodenheimer 2004). One answer to this issue is the use of EHR. The ability to share and store digital information has grown because of EHR technology, making it possible to save all patient and history data on servers. According to contemporary medical practitioners, improved interoperability and a shift in the information-sharing paradigm are both required to improve patient access to and the management of health data (Essén et al. 2018). Based on the convincing literature, the researcher chose to replace system quality in the D&M IS Success Model with EHR as a construct. The following hypothesis is offered to investigate this relationship:
H1: There is a significant positive relationship between EHR and information quality (IQ).
Information quality construct
Beyond the needs and standards for upgrading information, information that has been arranged and processed to give meaning and enhance decision-making (Romney & Steinbart 2014). Information systems are essential to the practice of evidence-based medicine because they give healthcare professionals access to clinical evidence and data about their patients' health as they develop patient-care initiatives (Del Fiol, Workman & Gorman 2014). There is some evidence that EHR can improve patient care standards and patient safety (Cea Soriano, Zong & García Rodríguez 2019; Naidoo & Wills 2016). The IQ was adopted for this study based on the literature without modifying the construct. The following hypothesis is offered to investigate this relationship:
H2: There is a significant positive relationship between KQ and better coordination of patient care (BCP).
Knowledge quality construct
According to Lee (2017), hospitals are knowledge-intensive settings that experience constant change because of improvements in medical technology. Prior research in industrialised nations has shown that installing a knowledge management system (KM) in hospitals can improve treatment protocols, boost knowledge sharing among medical specialists, lower healthcare costs and raise patient care standards (Koushazade, Omidianpoor & Zohurian 2015). Clinical knowledge is created through tacit knowledge (experiences or professional practices of caregivers), which is then transformed into explicit or documented forms such as clinical procedure guides, clinical workflows and EHRs (Chang et al. 2012). Clinical practice guidelines (CPGs), which are knowledge-rich clinical processes, are created and archived by an EHR system, improving their quality through prudent clinical judgements and increased clinician task productivity (Salleh, Abdullah & Zakaria 2017; Giguère et al. 2020). Consequently, knowledge quality for completion should be included in an IS quality review (Chang et al. 2012). The studies of DeLone and McLean did not include a construct: KQ. However, based on the literature, this researcher decided to adopt knowledge quality as a new construct in this study. The following hypothesis is offered to investigate this relationship:
H3: There is a significant positive relationship between EHR and KQ.
Perceived usefulness and perceived ease of use constructs
This study used TAM as a reference to investigate the implications of perceived EHR usability and usability. The basic objective of TAM is to explain why people utilise technology and how various factors influence this behaviour. The underlying premise of the TAM is that a person's use of technology is mediated by their acceptance of it, which is in turn impacted by two cognitive factors, namely perceived usefulness (PU) and perceived ease-of-use (PEU) (Jones & Kauppi 2018). For the purposes of this study, perceived ease of use will be defined as the opinion held by healthcare professionals that using an EHR to get patient medical history is essentially effortless. Numerous researchers have found a strong relationship between behavioural intention to use and perceived usefulness (Joo, Park & Lim 2018). The extent to which EMRs improve work performance and produce perceived benefits is what is meant by perceived usefulness in relation to EMRs (Asan et al. 2017). Perceived ease of use in connection to EMRs is concerned with the extent to which EMRs enhance work performance and bring about perceived benefits (Asan et al. 2017). Based on the literature review, these two constructs were adopted for this study. The following hypothesis is offered to investigate this relationship:
H4: There is a significant positive relationship between perceived usefulness and the adoption EHR at a South African public hospital.
Organisational context construct
Indeed, the TOE framework offers greater strength than more conventional models like the technology acceptance model and the united theory of acceptance and use of technology because it incorporates both human and non-human determinants into a single framework (Awa, Ojiabo & Orokor 2017). The two organisational context constructs are top management support and organisational readiness. The organisational context, which places a strong emphasis on management support for system adoption capability, also affects the adoption of EHR (Mtebe & Nakaka 2018). Top management support can relate to the level of top management support for implementing EHR to improve performance (Abdekhoda, Dehnad & Zarei 2015). Hence, the focus will be on top management support as a construct item of organisational context. The following hypothesis is offered to investigate this relationship:
H5: The adoption of EHR is influenced positively by top management support.
Medical error reduction construct
Medication errors are one of the most frequent causes of unintended harm to patients (Creed 2017). Furthermore, pharmaceutical mistakes can have disastrous effects and have even resulted in the deaths of certain patients (Creed 2017). Preventable prescription errors affect more than 7 million individuals in the United States of America (USA), costing the healthcare system as a whole roughly $21 billion annually (Da Silva & Krishnamurthy 2016). The entire cost of prescription errors is significantly higher when you factor in lost wages, disabilities, lost productivity and the cost of maintaining health. This is a significant issue that has to be resolved. The study postulates that MER directly influences disease diagnosis and treatment, with EHR serving as a catalyst for achieving that result. Based on the literature review, the researcher made the decision to add MER as a new construct to the (D&M) IS Success Model. The following hypothesis is offered to investigate this relationship:
H6: There is a significant positive relationship between EHR and MER.
Better coordination of patient care construct
Electronic health record systems are increasingly understood to be a vital tool for improving the quality, effectiveness and safety of healthcare (Graber, Byrne & Johnston 2017; Schopf et al. 2019). To simply put, implementing such technologies enables medical professionals to provide better care by enhancing record keeping, decision making and patient monitoring. The moderating construct intention to use was adopted from the D&M IS Success Model. The construct was modified to read BCP to accurately represent the study's goal. In proposal framework, BCP has a significant influence on EBHP. The fundamental premise of this study is that BCP is critically important in this context. Medical records are the main source of clinic materials and health data because they are succinct, precise and contain information about a patient's health history, ailments and medical occurrences from a medical perspective (Lungile & Trywell 2017). The following hypothesis is offered to investigate this relationship:
H7: There is a significant positive relationship between MER and BCP.
Diagnosis and treatment of diseases construct
One of the main goals of any health research is to increase the quality of care; as a result, it is critical to identify, share, work with and widen the knowledge of clinicians in order to learn and develop new information and, consequently, improve the quality of treatment. According to a study, using knowledge management techniques can improve care (Betelehem 2017; Mitiku, Jimma & Diriba 2016). Inaccurate diagnoses, improper therapies, medication errors, hazardous hospital practices and a lack of competent, sufficient medical training or understanding affect every country on the earth today (Kuziemsky 2016). The construct user satisfaction was changed in the (D&M) IS Success Model to DTD, and it occupied the position of a mediating variable in the conceptual framework. The following hypothesis is offered to investigate this relationship:
H8: There is a significant positive relationship between DTD and EBHP.
H9: There is a significant positive relationship between EHR and BCP.
Evidence-based healthcare practice construct
Evidence-based practice is the use of the most recent data in clinical decision-making (Melnyk et al. 2012). According to Anoushiravani et al. (2016), the integration of patient records might drastically minimise needless duplication of services and care as well as have a positive significant effect on the country's healthcare budget. Considering that the goal of this study is to explore factors that could influence medical healthcare professionals' decision to adopt EBHP. The net-benefits construct from the D&M IS Success Model was changed to EBHP for this study. In the suggested study framework (see Figure 1), this construct is a dependent variable, and the independent variables are MER, IQ, KQ, PU, diagnosis of diseases and treatments (DTD), technical context (TC) and Organization context (OC). While in this study, EHR and BCP served as mediating factors. The following hypothesis is offered to investigate this relationship:
H10: There is a significant positive relationship between BCP and EBHP.
Research and methods
Instrument development
This research employed a self-administrated questionnaire as a data collection method for the following reasons: the correspondence has a better chance to seek clarity while the questionnaire is be administered (Sekaran & Bougie 2016). A pre-test of the questionnaire with expert in the fields and a pilot study with potential participants were conducted. From the feedback received, the questionnaire was then modified and finalised the instrument based on their feedback. All of the items were measured using a 5-point Likert scale, where 1 = strongly disagree and 5 = strongly agree.
Participation and data collection
The study was conducted at one purposively selected public hospital, which was Dr George Mukhari Academic hospital, which lies close to Sefako Makgatho Health Science University (SMU), was the site of the study. Numerous departments are located within the hospital, including those for family medicine, dermatology, cardiology, neurology, haematology, renal or nephrology and intensive care unit (ICU), general surgery, neuro-surgery, cardiothoracic, ophthalmology, ENT, plastic surgery, urology, maxillofacial surgery, transplant unit, paediatrics, paediatric surgery, neonatal unit, KMC, orthopaedics and gynecology. SMU and other nursing schools in Pretoria train their students at this hospital. Data were gathered between June and October of 2021. It was impossible to get permission from other hospitals to carry out this study because of coronavirus disease 2019 (COVID-19) restrictions. The researcher chose to conduct this study in that specific hospital as DGMAH had already given the researcher permission to do so before the COVID-19 outbreak. The study population was medical healthcare professionals (doctors, nurses, radiographers). A total of 450 questionnaires were self-administered by the researcher, and from the questionnaires received, 150 were discarded because of incomplete data, resulting in a total of 300 responses.
Data analyses
The following section describes the process undertaken to analyse the data collected from the questionnaire. The first step was to undertake basic descriptive tests for 300 participants using SPSS Version 23, followed by exploratory factor analysis (EFA) to determine whether items loaded on their respective constructs as anticipated (Gaskin et al. 2014; Hair et al. 2010). Cronbach's alpha was performed to check the internal consistency of the items for reliability (Bagozzi & Yi 1998), followed by confirmatory factor analysis (CFA) to determine the convergent and discriminant validity of the measurement model (Gaskin et al. 2014; Holmes-Smith 2010). Lastly, SEM in the form of path analysis was used to test the hypotheses (Holmes-Smith 2010). The results of the data analysis are discussed in Section 7.
Descriptive statistics on the respondents
In terms of demographic profile of the surveyed respondents. The sample set is composed of 29.6% males and 70.40% females. Approximately 34.0% of the respondents were between the ages of 31 and 40, with 26 (8.6%) under the age of 25. 98 (32.6%) were between the ages of 21 and 50, while 57 (19.0%) were between the ages of 41 and 50 and 17 (5.6%) were above 50 years old. Medical doctors made up 16 (5.3%), while nurses were the majority 243 (81.0%). 147 (49.0%) had 6-10 years of experience, 68 (27.6%) had 2-5 years of experience, 76 (25.3%) had more than 10 years of experience and 19 (0.6%) had less than one year of experience.
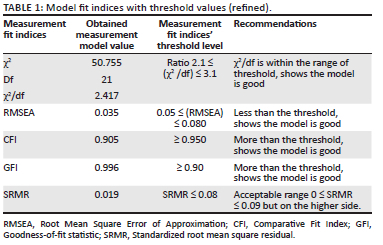
Measuring the model fitness
The results of the measurements of the fit indices, as extracted from AMOS, are listed in Table 1. In addition, the results reveal that the model fit was good according to two fit indices (χ2/df and SRMR). The new results were calculated using 50.755 chi-square statistics with 21 degrees of freedom (χ2/df = 50.755/21 = 2.4169). The conclusion of the results indicated that the model was well-fitting, with Root Mean Square Error of Approximation (RMSEA) = 0.035, Comparative Fit Index (CFI) = 0.905, Goodness-of-fit statistic (GFI) = 0.9996 and Standardized root mean square residual (SRMR) = 0.019. Analysis of Moment Structures (AMOS), on the other hand, proposed no more changes, implying that this was the model's best match. Given the complexity of SEM as an analytical technique, using two or more fit indices to achieve model fit is acceptable (Hooper, Coughlan & Mullen 2008; Kline 2011).
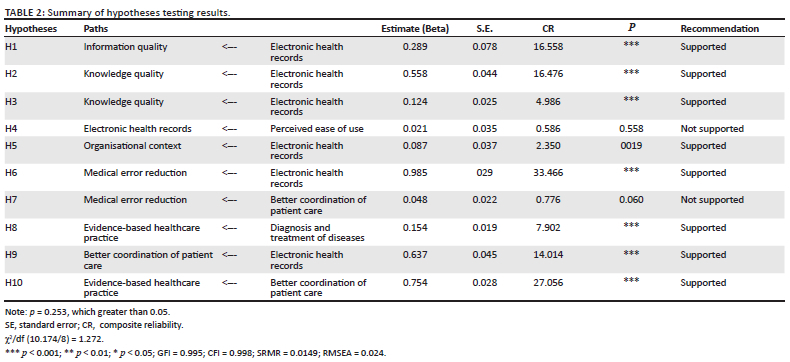
Results of hypotheses
The results of the hypotheses are presented in Table 2. All hypotheses, H1-H5, are supported. The first four hypotheses, H1-H4, are supported with a statistical significance level of 0.001 (p < 0.001), while hypothesis H5 is supported with a statistical significance level of 0.01 (p < 0.01).
Discussion
To develop an integrated model for EBHP, this study used the updated (D&M) IS Success Model, TOE and TAM. Structural equation was then used to analyse data. In addition, to evaluate how well the model fit the data from the EFA, CFA was also used. The results of study confirmed that between EHRs have a positive significant influence on IQ (β = 0.154; p < 0.05). For this reason, H1 was supported. The findings of this study corroborate those of Meeks et al. (2014), who found that the adoption of EHR may have a considerable effect on patient quality and safety.
As predicated in the research model, knowledge quality has a positive significant effect on better patient coordination of patient care (β = 0.985; p < 0.05). However, this H2 was supported. This finding is in line with previous research on the adoption of technological innovation (Shaltoni 2017). Findings of the study reaffirm a positive association between higher knowledge quality and better patient coordination, resolving the issue of contradictory findings in the literature. The results of H3 confirmed that EHRs have a positive significant influence on knowledge quality (β = 0.558; p < 0.05). This hypothesis was also supported. These findings are supported by Zayyad and Toycan's (2018) who claim that EHR facilitates timely communication among all healthcare providers as well as that access to patient medical records and related information. The study did not confirm that EHRs have a positive significant effect on perceived ease-of-use (β = 0.021; p > 0.05). For this reason, H4 was not supported. This finding is in contradiction with that of Hwang, Dutta and Chang (2019), who discovered a significant correlation between attitude and perceived ease of use in the context of physician acceptance of EHR.
The results of the study, however, did confirm that top management's support has a positive significant influence towards the use of EHRs (β = 0.087; p > 0.05). Therefore, H5 was supported in this study. However, the result is consistent with prior research, which demonstrated that leadership roles influence effective implementations in a variety of situations (Aarons, Ehrhart & Farahnak 2014). In addition, the study confirmed that knowledge quality and better patient coordination of patient care are positively and significantly related (β = 0.985; p < 0.05). For this reason, H6 was supported. This result is consistent with Berghout, Fabbricotti and Buljac (2017) assertion that doctors are highly knowledgeable professionals and that, as the largest group employed by hospitals, their decisions are typically based on their knowledge and experience. Furthermore, this study's results did not support BCP has a negative insignificant impact in the reduction of medical errors (β = 0.048; p > 0.05). According to Mitchell (2019), the adoption of an EHR will increase patient outcomes by enhancing the ability to diagnose illnesses and reducing or even preventing medical errors. These findings contradict with those of Mitchell. For this reason, H7 was not supported.
The results of this study confirmed that EBHP has positive significant influence on DTD (β = 0.154; p < 0.05). H8 was supported as a result. These results are consistent with Pyrene's (2015) claim that access to medical records is important as it is practically difficult for medical professionals to offer the best diagnosis or treatment without it. In addition, the study also confirmed that better patient coordination of patient care is positively influenced by the use of EHRs (β = 0.64; p < 0.05). This is also predicated in the research model and hypothesis H9 was supported. These results concur with those of Meeks et al. (2014), who claimed that the use of EHRs improves decision-making, record-keeping and patient care monitoring, allowing medical practitioners to offer better care. Furthermore, the results of H10 confirmed that EBHP has a direct positive influence on better patient coordination of patient care (β = 0.75; p < 0.05). Therefore, H10 was supported in this study. The outcomes of these findings support the claims made by Krist et al. (2014) that implementing an EHR system can facilitate health information exchange by catalysing the sharing of clinical information and patient care coordination among healthcare providers, potentially leading to higher-quality patient care. Since the model was tested and matches the data, the updated (D&M) IS Success Model, TOE and TAM frameworks can be used in the study to investigate the crucial successful factors for the adoption of EBHP in hospitals. This theoretical framework was developed to assist in determining the critical factors required for the adoption of EBHPs at a public hospital in South Africa.
Conclusion
This study contained a cross-sectional survey to understand which critical factors influence EBHP adoption at a public hospital in South Africa. With 300 valid responses, the results showed that the proposed model was acceptable with high significant of statistics for model fit indices. Nurses made up the majority of the participants (225 in total). The updated D&M IS Success Model, TAM and TOE formed the theoretical foundation. Seven dependent variables, EBHP and five independent variables: IQ, EHR, KQ, MER, BCP and DTD, were adopted from the updated and modified D&M IS Success Model. Perceived ease of the variable adopted for TAM while from TOE, organizational context was adopted and these variables were independent variables. The findings of this study reveal that the adoption of EBHP is strongly influenced by EHR, which is a crucial construct. In addition, the findings of this study also showed a strong positive significant relationship between the adoption of EBHP and the constructs of EHRs, MER, IQ and KQ. One of the key findings of this study was that the model used here for the adoption of EBHPs by the medical healthcare professionals at a public hospital in South Africa fit the data well and could be used to steer future research.
Implications
The current study extended and justified the existing D&M IS Success Model by adding KQ and reduction of medical errors as new constructs. BCP was also added to replace the moderating construct 'intention to use' and the construct user satisfaction was modified to read DTD. Net-benefits construct, the dependent variable in D&M IS Success Model was changed to read EBHP. With the adoption of the developed EBHP framework in public hospitals, healthcare professionals will be able to shift from a culture of providing care based on tradition, intuition, and authority to a situation where decisions will be guided and supported by the best available medical evidence.
Limitations and future research
This study contributes to advancing knowledge about the adoption of EBHP in the context of developing countries like South Africa, which may provide a fruitful avenue for future research. A sample population from one academic hospital in Gauteng province was used for the current investigation. Therefore, it is possible that the results do not accurately reflect the critical success factors that have a bearing on the adoption of EBHP in South African public hospitals. Future study is therefore required with a larger sample size, more varied sampling locations and a variety of sampling strategies.
In addition, the insignificant relationship between perceived ease of use and EHR H4 needs to further be investigated in a different hospital setting in other provinces. Furthermore, research should be conducted to determine the critical success factors that influence the adoption of EBHP in South African public hospitals, with additional data collection strategies such as interviews and focus groups being used to determine which is the most viable. Furthermore, the model of the current research can be modified and be applied to the adoption of other types of e-health services, such as telemedicine and mHealth (mobile Health), in South Africa or other developing countries.
Acknowledgements
This article is partially based on the author's thesis of a doctoral degree in Information Systems (IS) degree at the University of South, under the supervision of Prof B. Chimbo.
Without the assistance of the healthcare professionals at Dr George Mukhari Academic Hospital, the author would not have been able to complete this research work. I therefore would like to thank all the healthcare professionals who participated in this study.
Competing interests
The authors declare that they have no financial or personal relationships that may have inappropriately influenced them in writing this article.
Authors' contributions
Both authors, L.M and B.C both from (University of South Africa) School of Computing contributed equally to the research and the writing of this article.
Ethical considerations
Ethical clearance to conduct this study was obtained from the University of South Africa-CAES Health Research Ethics Committee (no. 2019/CAES/075).
Funding information
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Data availability
The datasets generated during and/or analysed during the current study are available in the Dataset repository [https://mylifeunisaac-my.sharepoint.com/:x:/g/personal/motsil_unisa_ac_za1/ERY4CbJ6F-NIvitS2AwPZuoBlq006bMRXy9P75MBBGVg-A?rtime=Mp7cJo-q2kg].
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of any affiliated agency of the authors.
References
Aarons, G.A., Ehrhart, M.G. & Farahnak, L.R., 2014, 'The implementation leadership scale (ILS): Development of a brief measure of unit level implementation leadership', Implementation Science 9(1), 45. https://doi.org/10.1186/1748-5908-9-45 [ Links ]
Abdekhoda, M., Dehnad, A. & Zarei, J., 2019, 'Determinant factors in applying electronic medical records in healthcare', Eastern Mediterranean Health Journal 25(1), 24-33. https://doi.org/10.26719/emhj.18.007 [ Links ]
Abera, G., Bekuma, T.T. & Tolossa, T., 2021, 'Modern contraceptives use by client choice and associated factors in public health facilities of Nekemte town, Western Ethiopia', International Journal of Africa Nursing Sciences 15(10), 100-330. [ Links ]
Adeleke, I.T., Lawal, A.H., Adio, R.A. & Adebisi, A.A., 2014, 'Information technology skills and training needs of health information management professionals in Nigeria: A nationwide study', Health Information Management Journal 44(1), 1-9. https://doi.org/10.12826/18333575.2014.0002 [ Links ]
Anoushiravani, A.A, Patton, J., Sayeed, Z., El-Othmani, M.M. & Saleh, K.J., 2016, 'Big data, big research: Implementing population health-based research models and integrating care to reduce cost and improve outcomes', Orthopedic Clinics 47(4), 717-724. [ Links ]
Asan, O., Flynn, K.E., Azam, L. & Scanlon, M.C., 2017, 'Nurses perceptions of a novel health information technology: A qualitative study in the pediatric intensive care unit', International Journal of Human-Computer Interaction 33(4), 258-264. [ Links ]
Awa, H., Ojiabo, U. & Orokor, L., 2017, 'Integrated technology-organization-environment (T-O-E) taxonomies for technology adoption', Journal of Enterprise Information Management 30(6), 893-921. [ Links ]
Bagozzi, R.P., Yi, Y. & Nassen, K.D., 1998, 'Representation of measurement error in marketing variables: Review of approaches and extension to three-facet designs', Journal of Econometrics 89(1-2), 393-421. [ Links ]
Berghout, M.A., Fabbricotti, I.N., Buljac-Samardžić, M. & Hilders, C.G.J.M., 2017, 'Medical leaders or masters? A systematic review of medical leadership in hospital settings', PLoS One 12(9), e0184522. [ Links ]
Betelehem, L., 2017, 'A framework to support knowledge sharing practice among health care professionals at Yekatit 12 Hospital Medical College', Msc thesis, Addis Ababa University, Addis Ababa, Ethiopia.
Boyes, H., Hallaq, B., Cunningham, J. & Watson, T., 2018, 'The industrial internet of things (IIoT): An analysis framework', Computers in Industry 101, 1-12. https://doi.org/10.1016/j.compind.2018.04.015 [ Links ]
Capık, C., 2014, 'Use of confirmatory factor analysis in validity and reliability studies', Journal of Anatolia Nursing and Health Sciences 17, 196-205. [ Links ]
Cea Soriano, L., Zong, J. & García Rodríguez, L.A., 2019, 'Feasibility and validity of The Health Improvement Network database of primary care electronic health records to identify and characterize patients with small cell lung cancer in The United Kingdom', BMC Cancer 19(1), 1-9. https://doi.org/10.1186/s12885-019-5305-1 [ Links ]
Chao, W.C., Hu, H., Ung, C.O.L., Cai, Y., 2013, 'Benefits and challenges of electronic health record system on stakeholders: A qualitative study of outpatient physicians', Jouranl of Medical Systems 37, 1-6. https://doi.org/10.1007/s10916-013-9960-5 [ Links ]
Chang, I.C., Li, Y.C., Wu, T.Y. & Yen, D.C., 2012, 'Electronic medical record quality and its impact on user satisfaction - healthcare providers' point of view', Government Information Quarterly 29(2), 235-242. https://doi.org/10.1016/j.giq.2011.07.006 [ Links ]
Creed, S., 2017, 'Avoiding medication errors in general practice', Practice Nurse 47(2), 24-26. [ Links ]
Da Silva, B. & Krishnamurthy, M., 2016, 'The alarming reality of medication error: A patient case and review of Pennsylvania and national data', Journal of Community Hospital Internal Medicine Perspectives 6(4), 1-6. [ Links ]
Davis, F.D., Bagozzi, R.P. & Warshaw, P.R., 1989, 'User acceptance of computer technology: A comparison of two theoretical models', Management Science 35(8), 982-1003. [ Links ]
Del Fiol, G., Workman, E. & Gorman, G., 2014, 'Clinical questions raised by clinicians at the point of care: A systematic review', JAMA Internal Medicine 174(5), 710-718. [ Links ]
Delone, W.H. & McLean, E.R., 2003, 'The Delone and Mclean model of information systems success: A ten-year update', Journal of Management Information Systems 19(4), 9-30. [ Links ]
Dowding, D.W., Turley, M. & Garrido, T., 2015, 'Nurses' use of an integrated electronic health record: Results of a case site analysis', Informatics for Health & Social Care 40, 345-361. [ Links ]
Fitrios, R., 2016, 'Factors that influence accounting information system implementation and accounting information quality', International Journal of Scientific & Technology Research 5(4), 192-198. [ Links ]
Gaskin, J.E., Berente, N., Lyytinen, K. & Yoo, Y., 2014, 'Toward generalizable sociomaterial inquiry: A computational approach for zooming in and out of sociomaterial routines', MIS Quarterly 3(38), 849-871. [ Links ]
Giguère, A., Zomahoun, H.T.V., Carmichael, P.H., Uwizeye, C.B., Légaré, F., Grimshaw, J.M. et al., 2020, 'Printed educational materials: effects on professional practice and healthcare outcomes', Cochrane Database of Systematic Reviews 8. [ Links ]
Graber, M.L., Byrne, C. & Johnston, D., 2017, 'The impact of electronic health records on diagnosis', Diagnosis 4(4), 211-223. [ Links ]
Grumbach, K. & Bodenheimer, T., 2004, 'Can health care teams improve primary care practice', Journal of American Medical Association 291(10), 1246-1251. https://doi.org/10.1001/jama.291.10.1246 [ Links ]
Hair, J.F., Black, W.C., Babin, B.J. & Anderson, R.E., 2010, Multivariate data analysis, 7th edn., Prentice Hall, Upper Saddle River, NJ.
Holmes-Smith, P., 2010, Structural equation modeling: From the fundamentals to advanced topics, SREAMS (School Research Evaluation and Measurement Services), Melbourne.
Hooper, D., Coughlan, J. & Mullen, M.R., 2008, 'Structural equation modelling: Guidelines for determining model fit', The Electronic Journal of Business Research Methods 6(1), 53-60. [ Links ]
Hwang, H.G., Dutta, B. & Chang, H.C., 2019, 'The Differing Effect of Gender and Clinical Specialty on Physicians' Intention to Use Electronic Medical Record', Methods of Information in Medicine 58(S 02), e58-e71. [ Links ]
Jones, A.B. & Kauppi, K., 2018, 'Examining the antecedents of the technology acceptance model within e-procurement', International Journal of Operations and Production Management 38(1), 22-42. https://doi.org/10.1108/IJOPM-06-2015-0346 [ Links ]
Joo, Y.J., Park, S. & Lim, E., 2018, 'Factors influencing preservice teachers' intention to use technology: TPACK, teacher self-efficacy, and technology acceptance model', Journal of Educational Technology & Society 21(3), 48-59. [ Links ]
Karch, A.M., 2015, 'Preventing medication errors by empowering patients', American Nurse Today 10(9), 18-23. [ Links ]
King, J., Patel, V., Jamoom, E.W. & Furukawa, M.F., 2014, 'Clinical benefits of electronic health record use: National findings', Health Services Research 49(1 PART 2), 392-404. [ Links ]
Kline, R.B., 2011, Principles and practice of Structural Equation Modelling, 3rd edn., The Guilford Press, New York, NY.
Koushazade, S.A., Omidianpoor, S. & Zohurian, M., 2015, 'The impact of organizational factors on the effectiveness of knowledge management among nurses', International Journal of Hospital Research 4(3), 129-135. [ Links ]
Krist, A.H., Beasley, J.W., Crosson, J.C., Kibbe, D.C., Klinkman, M.S., Lehmann, C.U. et al., 2014, 'Electronic health record functionality needed to better support primary care', Journal of the American Medical Informatics Association 21, 764-771. https://doi.org/10.1136/amiajnl-2013-002229 [ Links ]
Kruse, C.S., Mileski, M. & Alaytsev, V., 2015, 'Adoption factors associated with electronic health record among long-term care facilities: A systematic review', BMJ Open 5, e006615. [ Links ]
Kumar, A., Verma, A.K. & Bharti, D.J., 2020, Aspects of digitalization of healthcare in India, International Journal of Research and Analytical Reviews (IJRAR), p. 5.
Kuziemsky, C., 2016, 'Decision-making in healthcare as a complex adaptive system', Healthcare Management Forum 29(1), 4-7. https://doi.org/10.1177/0840470415614842 [ Links ]
Lee, H.S., 2017, 'Knowledge management enablers and process in hospital organizations', Osong Public Health and Research Perspectives 8(1), 26-33. [ Links ]
Loehlin, J.C., 2004, Latent variables models: An introduction to factor, path and structural equation analysis, 4th edn., Lawrence Erlbaum Associates, Inc., Mahwah, NJ.
Lungile, P.L. & Trywell, K., 2017, 'The management of medical records in the context of service delivery in the public sector in KwaZulu-Natal, South Africa: The case of Ngwelezana hospital', Journal of Library and Information Sciences 83(2), 1-11. [ Links ]
Marutha, S., 2011, 'Records management in support of service delivery in the Public Health Sector of The Limpopo Province in South Africa', Doctoral dissertation, University of South Africa. [ Links ]
Meeks, D.W., Smith, M.W., Taylor, L., Sittig, D.F., Scott, J.M. & Singh, H., 2014, 'An analysis of electronic health record-related patient safety concerns', Journal of American Medicl Information Association 21, 1053-1059. https://doi.org/10.1136/amiajnl-2013-002578 [ Links ]
Melnyk, B.M., Fineout-Overholt, E., Gallagher-Ford, L. & Kaplan, L., 2012, 'The state of evidence-based practice in US nurses: Critical implications for nurse leaders and educators', Journal of Nursing Administration 42(9), 410-417. [ Links ]
Mitchell, J., 2019, History of electronic health records, viewed 08 September 2022, from http://study.com/academy/lesson/history-of-electronic-health-records.html.
Mitiku, H., Jimma, W. & Diriba, C., 2016, 'Managing indigenous knowledge for corrective and preventive cares: The case of Horro Guduru Wollega Zone, Oromia, Ethiopia', Universal Journal of Public Health 4(4), 212-217. [ Links ]
Moro Visconti, R. & Morea, D., 2020, 'Healthcare digitalization and pay-for-performance incentives in smart hospital project financing', International Journal of Environmental Research and Public Health 17(7), 2318. [ Links ]
Mtebe, J.S. & Nakaka, R., 2018, 'Assessing electronic medical record system implementation at Kilimanjaro Christian Medical Center, Tanzania', Journal of Health Informatics in Developing Countries 12(2). [ Links ]
Naidoo, J. & Wills, J., 2016, Foundations for health promotion, Elsevier Health Science.
Nene, N., 2015, Find your file, sick man told, IOL News, viewed 01 July 2022, from http://www.iol.co.za/dailynews/news/find-your-file-sick-man-told1.1812123#.Vd8KGKguDIU.
Nwankwo, B. & Sambo, M.N., 2018, 'Can training of health care workers improve data management practice in health management information systems: A case study of primary health care facilities in Kaduna State, Nigeria', The Pan African Medical Journal 30, 289. [ Links ]
Pyrene, M.B., 2015, 'The management of records for healthcare service delivery at the Victoria Public hospital in the Eastern Cape Province in South Africa', Master's thesis, University of Fort Hare. [ Links ]
Raut, A., Yarbrough, C., Singh, V., Gauchan, B., Citrin, D., Verma, V. et al., 2018, 'Design and implementation of an affordable, public sector electronic medical record in rural Nepal', Journal of Innovation in Health Informatics 24(2), 862. [ Links ]
Schopf, T.R., Nedrebø, B., Hufthammer, K.O., Daphu, I.K. & Lærum, H., 2019, 'How well is the electronic health record supporting the clinical tasks of hospital physicians? A survey of physicians at three Norwegian hospitals', BMC Health Services Research 19(1), 1-9. [ Links ]
Schoenfeld, E.M., Goff, S.L., Downs, G., Wenger, R.J., Lindenauer, P.K., Science, P. et al., 2018, 'A qualitative analysis of patients' perceptions of shared decision-making in the emergency department: "Let me know I have a choice"', Academic Emergency Medicine 25(7), 716-727. https://doi.org/10.1111/acem.13416. [ Links ]
Sekaran, U. & Bougie, R., 2016, Research methods for business: A skill-building approach, 7th edn., John Wiley & Sons, Haddington.
Shah, R. & Chircu, A., 2018, 'IoT and AI in healthcare: A systematic literature review', Issues in Information Systems 9(3), 33-41. https://doi.org/10.48009/3_iis_2018_33-41 [ Links ]
Shaltoni, A.M., 2017, 'From websites to social media: Exploring the adoption of internet marketing in emerging industrial markets', Journal of Business & Industrial Marketing 32(7), 1009-1019. https://doi.org/10.1108/jbim-06-2016-0122 [ Links ]
Sockolow, P.S., Bowles, K.H., Adelsberger, M.C., Chittams, J.L. & Liao, C., 2014, 'Impact of homecare electronic health record on timeliness of clinical documentation, reimbursement, and patient outcomes', Applied Clinical Informatics 5(2), 445-462. [ Links ]
Tornatzky, L.G. & Fleischer, M., 1990, The process of technological innovation, Lexington Books, New York, NY.
Zayyad, M.A. & Toycan, M., 2018, 'Factors affecting sustainable adoption of e-health technology in developing countries: An exploratory survey of Nigerian hospitals from the perspective of healthcare professionals, PeerJ 6, e4436. https://doi.org/10.7717/peerj.4436 [ Links ]
 Correspondence:
Correspondence:
Lovemore Motsi
motsil@unisa.ac.za
Received: 04 Oct. 2022
Accepted: 23 Feb. 2023
Published: 14 July 2023


{kind=link}
{kind=link}