










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Information Management
On-line version ISSN 1560-683X
Print version ISSN 2078-1865
SAJIM (Online) vol.25 n.1 Cape Town 2023
http://dx.doi.org/10.4102/sajim.v25i1.1613
ORIGINAL RESEARCH
Critical success factors of smart card technology in South African public hospitals
Lario Malungana; Lovemore Motsi
School of Computing, College of Science, Engineering and Technology, University of South Africa, Pretoria, South Africa
ABSTRACT
BACKGROUND: Even though the government has set several admirable targets for raising the standard of healthcare, as highlighted by communities and media reports, public health institutions' services continue to fall short of patients' expectations and basic standards of care. For this reason, the general public has lost faith in the healthcare system. The public healthcare system in South Africa is completely dysfunctional and urgently needs to be transformed to serve the majority of those who use public hospitals.
OBJECTIVES: The study aimed to improve healthcare for the majority of South Africans by investigating the critical success factors (CSFs) that influence the adoption of smart card technology (SCT) in South African public hospitals.
METHODS: A thorough review of peer-reviewed literature was conducted to determine potential barriers to adopting SCT. Furthermore, a hybrid model that combines the Health Unified Technology of Acceptance Theory (HUTAUT) model, DeLone and McLean IS success model (D&M) and the diffusion of innovation (DOI) theory will be developed, validated and tested to identify the CSFs adoption of SCT in public hospitals in South Africa
RESULTS: The validated research model has been developed to be adopted by nurses at public hospitals.
CONCLUSION: This research will contribute to the development of a new framework that identifies the CSFs for SCT adoption in South African public hospitals.
CONTRIBUTION: The study's results will make a special contribution to the body of knowledge in the fields of health informatics, particularly e-health.
Keywords: adoption; public healthcare; healthcare professionals; technology; e-health.
Introduction
The World Health Organization (WHO) defined e-health as the use of information communication technologies (ICTs) for healthcare. Much attention has been drawn to the efficient use of medical information management systems by academics. Alberts et al. (2014) state that e-health technologies are used to treat patients, conduct medical research, educate the health workforce, track diseases and monitor public health. Lau and Kuziemsky (2016) added that e-health is an evolving field in the interaction of medical informatics, public health, and business, health services and information delivered or enhanced through the Internet and related technologies. The last decade has seen the emergence of smart card technology (SCT), which has various potential applications in the manufacturing, banking, logistics, agriculture, retail sectors and the healthcare sector. The continuous nature of health services, which must be delivered with high quality and effectiveness around the clock, presents the healthcare business with numerous obstacles (Aboelmaged & Hashem 2018). Prior studies have shown that the adoption of new technology is seen as the new critical success for healthcare services in South Africa. Although SCT is customised according to the sectoral needs, it consists of a single memory chip with no other functions, an embedded integrated circuit, a secure microcontroller, or any device with comparable intelligence and internal memory.
The electronic health card, for example, was adopted in Germany as the foundation of its e-health infrastructure (Wirtz, Mory & Ullrich 2012). Barbosa, Takako and Sadok (2020) found that there were challenges in interfacing with human users and other systems. However, the lack of data support and confidentiality leads to authenticity control of devices on the network. Furusa and Coleman (2018) pointed out that for e-health to be implemented in Zimbabwe, doctors would have to demonstrate their capacity to use the technology. For this reason, doctors have been required to learn how to use e-health technologies in public hospitals, which require hardware and software that cannot be avoided during treatment. This study seeks to address challenges facing South African hospitals regarding administration, medical assistance, the provision of healthcare services and many others by using critical factors for the adoption of SCT. The findings will guide nurses, management, clinicians and pharmacists in adopting SCT for delivering healthcare services at hospitals to patients.
Theoretical gaps
Healthcare Unified Theory of Acceptance of User Technology (HUTAUT) aimed to understand why users accept or reject a technology and how healthcare technology design can improve user adoption. The HUTAUT was developed by Maeko and Van Der Haar (2018) for allowing acceptance and user influence in public healthcare (Maeko & Van Der Haar 2018). The HUTAUT model was only tested as a new model in healthcare and has added value in understanding the many phases of technology implementation in healthcare. However, the framework relied much on good skills and user interaction to achieve a successful technology deployment, which is a barrier to implementation in hospitals. Therefore, can only be effectively adopted as an adoption process in South African public hospitals.
Quantitative researchers have widely used DeLone and McLean (D&M) models to assess the effectiveness of information systems (IS) (DeLone & McLean 1992, 2003). This evaluation framework has typically been used to determine how various success factors might benefit people and organisations. However, the D&M model appears to be common. As a result, more evaluations are needed to find additional potential elements that might have a favourable impact on how well healthcare professionals use the SCT in public hospitals. Smart card technology can be used to share information, promote technological expertise and improve uses across several systems. Hence, knowledge quality for completion should be included in an IS quality review (Jeyaraj 2020). As healthcare systems are familiar with the D&M model, the D&M model is considered as being irrelevant because of the mandatory use of other e-health systems (Petter, Delone & McLean 2013). Therefore, the D&M model must be revised with an improved measure for IS user performance when it is compulsory. In measuring the success of IS, the D&M models delineate user satisfaction. However, there is a strong correlation between system quality, information quality and the subjective measure of user satisfaction construct (Aquino et al. 2018), thus the low explanatory capability because of recurring measures (Srur & Drew 2012).
Although diffusion of innovation theory (DOI) has been used in most qualitative studies, DOI has been applied in academics and other institutions to adopt the technology. The DOI is defined as a theory that examines how innovation, communication channels, time and social systems interact for the adoption of a new idea, concept or technology in a given adopter market (Mollaoglu et al. 2016). However, most organisations have long realised that adopting or rejecting information technology (IT) leads to the success or failure of business objectives. As a result, the ability to communicate new technology and the user's acceptance of it has become crucial to IS research and practice (Iyamu 2021). Therefore, it has been observed that public healthcare may not have the opportunity to recognise the consequences or feedback from healthcare professionals.
Research model
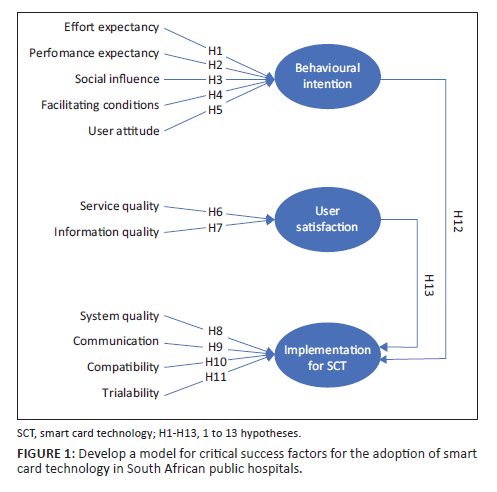
Sets of relationships among exogenous, mediating and endogenous constructs of the proposed study model are illustrated in Figure 1. Each path possesses a positive hypothesised effect. For the benefit of this study, the HUTAUT model (Maeko & Van der Haar 2018), the Delone and McLean IS success model (2003) and the DOI theory (Rogers 2003) were identified as the underpinning theoretical frameworks. In the context of this study, the independent variables in this study were expected to be sustained factors that lead to positive user behavioural intention. Constructs such as behavioural intention and user satisfaction were used as mediating factors. A schematic view of this model is shown in Figure 1.
Methodology
Study design
In this study, HUTAUT, D&M models and DOI are based on prior quantitative instruments connected to the research variables and the local context of South African public hospitals adoption was used to build the important factors for the SCT user survey that was conducted. A 5-point Likert scale was used to collect responses, with 1 representing 'strongly disagree' and 5 representing 'strongly agree'. According to what is implied by this scale, the respondents have a lot of selection flexibility (Hung, Tsai & Chuang 2014). After analysis, a survey questionnaire should be included for increased reliability and validity (Odhiambo 2015). The study further reviewed the questionnaires before data collection by distributing them to nurses.
For the new questionnaire, a pilot test was carried out for 50 nurses at Steve Biko Academic Hospital (six emergency nurses, 13 midwives, 14 paediatric nurses, 15 neonatal surgical nurses, and 2 other nurses from different departments). The result was further analysed by principal component analysis (PCA) using the Statistical Package for the Social Sciences (SPSS), specifically, for all measured constructs.
The Kaiser-Meyer-Olkin (KMO) and Bartlett's tests were the second result of the PCA factor analysis. The KMO statistic ranges from 0 to 1. For factor analysis to be effective, the value of KMO should be close to 1 rather than 0. A value close to 1 indicates that correlation patterns are relatively compact, implying that factor analysis should yield distinct and reliable factors. Accepting values greater than 0.5 is recommended by Kaiser (1974). Furthermore, values between 0.5 and 0.7 are considered mediocre, values between 0.7 and 0.8 are considered good, values between 0.8 and 0.9 are good and values greater than 0.9 are considered superb. Therefore, the KMO statistic value for the data used in this study was found to be 0.918.
Data collection
A purposive sampling technique was employed to collect the data due from nurses from different wards. This study used the cross-sectional data collection method based on structured questionnaires. Structured questionnaires were provided to healthcare personnel at Kalafong Tertiary Hospital, Steve Biko Academic Hospital, Tshwane District Hospital and Pretoria West District Hospital. These hospitals were chosen based on a few characteristics, including their location in Gauteng and the communities or areas they serve. Furthermore, each hospital is classified as academic, tertiary or district-based hospital. Data were collected over 9 months because of the coronavirus disease 2019 (COVID-19) pandemic. A total of 486 survey questionnaires were distributed; however, the responses were 406 in total. Steve Biko Academic exhibited the highest usable responses (60%) followed by Kalafong Tertiary hospital (15%), Tshwane District hospital (10%) and Pretoria West hospital (5%).
Data analysis technique
Quantitative analysis is used to determine the strength of correlations between various components in the context of an event. The predictions of a theory are used in this procedure to see whether the hypothesis is viable. The greatest strength of quantitative analysis lies in providing repeatable evidence that supports the theoretical prediction. Furthermore, quantitative analysis can detect minor associations, which would be undetected by human data analysis. The questionnaire data were collected, analysed and validated with SPSS (v26). The variables were then defined and labelled. In addition, before using SPSS, data were imported into Microsoft Excel to check for errors (Esewe 2017). For complex statistical data analysis, a multitude of academics utilise SPSS. The SPSS software package was created for the management and statistical analysis of social science data. Respondents from the listed hospitals in the Tshwane district completed all questions. The study adopted variables and relationships for statistical techniques using SPSS software. For the benefit of data analysis, exploratory factor analysis (EFA), confirmatory factor analysis (CFA) and structural equation modelling (SEM) were applied for a hybrid of factor analysis and path analysis (Maguraushe 2021).
Ethical considerations
Ethical clearance to conduct this study was obtained from the University of South Africa CAES Health Research Ethics Committee (reference no. 2020/CAES_HREC/081).
Results
Descriptive analysis
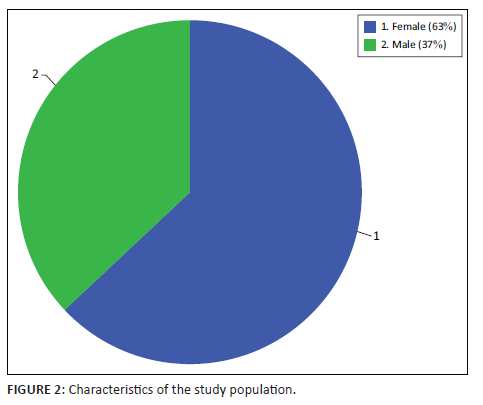
Using descriptive statistics, we investigated and analysed summary information on the distribution and central tendency of continuous variables. Mean, minimum, maximum and skewedness values were used to analyse and comprehend the distribution of the collected data. The mean value represents the midpoint of the available range. Skewness is a measure of asymmetry in a set of statistical data from the normal distribution (Pallant 2020). Skewedness is classified into two types: negative and positive (Pallant 2020). The females had the highest representation of 63%, while their male counterparts were 37% of the total sample. Generally, it was difficult to have an equal representation of both gender; therefore, these statistics are acceptable so that the conclusions drawn from this study can be generalised across gender.
A total of 406 usable responses from the total distributed 486 surveys, representing a 74% response rate, were subjected to descriptive analysis in SPSS. Figure 2 depicts the profile of the respondents. The sample exhibited unequal representation of female (63%) and male (37%) nurses because of a larger percentage of female nurses in the surveyed hospitals. There was an unbalanced number of respondents because of COVID-19-related illnesses among these nurses affected the response rate.
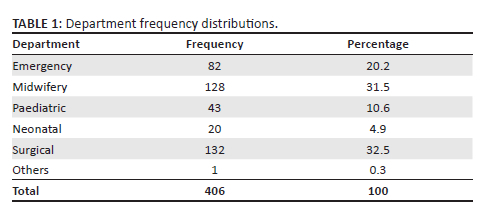
Respondents were asked to specify the department they work in. The results as summarised in Table 1 indicated that 32.5% of the respondents work in the surgical department, which is the most represented. The midwifery department followed this with a total of 31.5% of the sample. Emergency and paediatric departments represent 20.2% and 10.6%, respectively. The least represented departments are the neonatal and other departments that were not explicitly mentioned in the questionnaire, each with 4.9% and 0.2%, respectively.
Results from the structural equation modelling
In this study, the outcome of the structural equation model highlighted the relationship between the investigated constructs. The summary was extracted from Analysis of a Moment Structures output of the standardised significance levels obtained after running the hypotheses in Table 2. The levels of the hypothesised relationships between latent variables compromised the underlying causal structure of the SCT implementation. The hypothesised relationship was established according to a ratio of 1.96. This simply means that hypotheses are significant or supported, and if their constructs should be greater than 1.96, then it is rejected.
Final research model
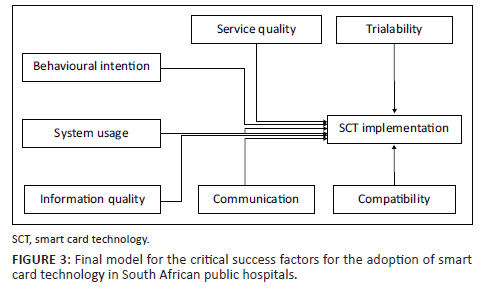
Only the hypotheses included in the final research model, depicted in Figure 3, were accepted. The model also depicts the relationship between organisational factors, technological acceptance factors and IS success variables that led to the adoption of SCT in observable ways. The accepted hypotheses H5, H8, H9, H10, H11, H12 and H13 make up the critical success factors (CSF) that conceptualise the adoption of SCT.
Discussion
This study aimed to investigate the CSF of SCT in South African public hospitals with the relationship between behavioral intention (BI), system quality (SQ), system usage (SU), information quality (IQ), communication (C), Compatibility (CP) and trialability (TR) have the influence of these variables on SCT. The results in Table 2 show that the first hypothesis effort expectancy (H1) was not supported. This suggests that effort expectancy does not significantly impact the implementation of SCT (β = −0.575, p = 0.862, R2 = 0.75). The findings of this study corroborate Steininger et al. (2014) that some of the variables have a significant impact on the implementation of IT systems. Although some of the variables were found to be having a positive impact on the adoption of the SCT, such as hypothesis 5, BI having a significant impact on the adoption of SCT was supported (β = −0.209, p < 0.001, R2 = 0.75) suggesting an inverse relationship between the two variables.
However, the performance expectancy (H2) hypothesis was dropped because of low reliability. On the other hand, hypotheses 6 and 7 (user attitude and user satisfaction effect on adoption of SCT) were not supported (β = 0.480, p = 0.741, R2 = 0.75 and β = −0.317, p = 937, R2 = 0.75, respectively). This finding resonates with the previous research in a study conducted on the understanding of the barriers and the levels of adoption for physicians in the United States of America (USA) (El-Yafouri & Klieb 2014). Therefore, the findings in this study support that the hypotheses from 8 to 13 were supported. It was found that system use (β = 0.209, p < 0.001, R2 = 0.75), information quality (β = 0.557, p < 0.001, R2 = 0.75), service quality (β = 0.562, p < 0.001, R2 = 0.75), communication (β = 0.211, p < 0.001, R2 = 0.75), compatibility (β = 0.419, p < 0.001, R2 = 0.75) and trialability (β = −0.020, p < 0.001, R2 = 0.75) variables had a significant impact on the adoption of SCT in South African public hospitals.
Conclusion
This study examined the CSF that South African public hospitals needed to adopt SCT. This study identified four CSF for the adoption of SCT: The cost of adopting SCT, management strategies and technology, data management of the smart card by healthcare professionals, and privacy and security of data management in healthcare. Three underlying theories were used in this study as a lens to analyse the CSF for the adoption of SCT. The HUTAUT model, the DeLone and McLean IS success model (D&M) (2003) and the DOI were all integrated into the framework that was developed. This framework was tested and validated to identify the CSF for the adoption of SCT. The findings indicate that the primary stakeholders influencing the origination's implementation strategy are the government, top management, shareholders and employees. However, the results show that the implementation strategy of any system within an organisation is influenced by how the organisation perceives its workers. The data collection process for this study may have some limitations. This study included 406 participants and information was collected from them at Steve Biko Academic Hospital, Tshwane District Hospital, Kalafong Tertiary Hospital, and Pretoria West Hospitals. As a result, because this study was limited to a single province's small scale, it might not be adequate. For this reason, it is advised that studies be carried out in the future that concentrate on other public hospitals that are included in the study.
Implications
Policy implications
The study's findings showed that the effectiveness of information and service had a major influence on the adoption of SCT in healthcare. The study's findings also imply that strict policies must be adopted to ensure the effective and efficient use of SCT in public healthcare. This study's findings confirmed that regardless of whether a service is provided by internal agencies or by outside contractors, policies and procedures must guide the service provider. According to Hsu, Yen and Chung (2015), service quality makes it possible to assess the caliber of ICT services offered by healthcare professionals. As a result, it has been made clear how important service quality is when applying SCT in public healthcare, especially when dealing with patients' vital health information. In order to maximise the use of smart card technologies, adequate regulations are needed to control the operational requirements and service quality of healthcare providers.
The researchers draw the conclusion that the absolute quality of the information in the system is necessary for the adoption of smart cards in public healthcare to be successful. According to Kilsdonk, Peute and Jaspers (2017), the idea of information quality is the integration of various elements, such as human, organisational and technical variables that provide a variety of information in the system. Furthermore, the Department of Health needs to create a clear policy guide based on the study's background which would make it easier for the public and private sectors to use computer technology in their different settings while maintaining high data quality.
An environmental management system is a set of management principles, operational procedures and performance standards for improving a business's environmental performance (Angeles 2014). Infrastructure, privacy and security issues must be addressed while making wise decisions to maintain healthcare performance. Without first educating healthcare professionals about the technology, the Department of Health would not be able to decide on the adoption of SCT. Furthermore, of the people in their environment, healthcare professionals are socially conditioned to respond in a variety of ways (Howell et al. 2016). The extensive use of performance construct adopted in HUTAUT, which directly impacts implementation, is said to be directly impacted by technology.
Theoretical implication
The research's findings were thoroughly investigated and it was found that BI, communication, compatibility and trialability positively impact the adoption of SCT. According to the studies of the following theories, it can be inferred that these findings have direct theoretical implications:
-
Maeko's Unified Theory of User Technology Acceptance of User Technology in Healthcare (HUTAUT) is supported by BI (Maeko & Van der Haar 2018).
-
The DeLone and McLean IS success model (2003) is supported by system use.
-
Rogers' (2003) DOI theory is supported by factors such as communication, compatibility and trialability.
Maeko's (Maeko & Van der Haar 2018) HUTAUT model shows that BI affects how people use technology. The mediating construct that is significant for the adoption of SCT is the BI construct as used in the UTAUT model (as HUTAUT is derived from UTAUT theory). In addition, BI is the primary indicator of SCT's actual use and demonstrates the healthcare professional's willingness to use it. Intriguingly, the study discovered that BI significantly affects SCT in public healthcare and that it is a valid construct in the HUTAUT model with a significant value of 0.01. As a result, there are higher standards for SCT adoption, including behavioural intent and commitment to using technology to improve the adoption environment for SCT.
System use is a crucial aspect of adopting SCT in public healthcare and has been extensively used in studies by the Delone and McLean IS success model (1992, 2003). Because system use makes healthcare operational processes simpler, it is believed to significantly impact SCT in public healthcare. In addition, it has sophisticated search features, multiple access points and the capacity to digitally combine data from numerous databases worldwide (Acquah-Swanzy 2015). In line with technological adoption and usage, the findings highlight communication, compatibility and trialability as essential elements of Rogers' (2003) DOI theory. For SCT to be adopted in public hospitals, communication, compatibility and trialability are all crucial components with important values (p = 0.01). This statement backs up Rogers' DOI model's theoretical stance. According to the DOI theory, communication is the primary means by which news about innovations such as the SCT is disseminated through contemporary media. Rogers (2003) asserts that the degree of confidence that is dependable on existing principles and the anticipated user requirements determine compatibility. The results of this study corroborate Rogers' findings from 2003, who discovered that compatibility can accommodate individual preferences using SCT systems, making innovation more adaptable in public healthcare institutions.
The concept and theory that encourages healthcare professionals to adopt novel approaches and adopt goals and values that are compatible with their current work practices are strengthened by this study. As a result, advantages such as data protection, storage capacity, data consistency, access authorisation, data ownership, device usability and privacy concerns become apparent early on in the adoption process (Cripps, Standing & Prijatelj 2012). The results of this study also support Rogers' (2003) DOI theory, according to which compatibility is a key factor in the introduction of new products such as the SCT in public healthcare facilities.
In addition, according to Rogers (2003), trialability - or a system's ability to be tested or trialled before making firm decisions - is a crucial element for technology implementation. According to the study's findings, trialability significantly affects SCT implementation, which is consistent with Rogers' (2003) research. This study addressed the importance of trialability in SCT adoption and confirms the work of Dos Santos Brito (2014). It was found that trialability in DOI addresses the adoption of technology in healthcare from data inputs, data storage and data processes on portable devices and servers to maintain personal data for smart health. The findings of this study are also consistent with those of Tsai and Chang (2016), who discovered that a system's adoption is the only factor that determines whether it succeeds or fails. This covers the creation and administration of policies as well as software planning and development.
Acknowledgements
Competing interests
The author(s) declare that they have no financial or personal relationship(s) that may have inappropriately influenced them in writing this article.
Authors' contributions
Lovemore Motsi contributed to the research, methodology, data collection and data analysis of the article. Lario Malungana contributed to the introduction, discussion and conclusion of the article. Both authors consented to the final draft of the article for submission.
Funding information
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Data availability
The data that support the findings of this study are available on request from the corresponding author.
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of any affiliated agency of the authors.
References
Aboelmaged, M. & Hashem, G., 2018, 'RFID application in patient and medical asset operations management: A technology, organizational and environmental (TOE) perspective into key enablers and impediments', International Journal of Medical Informatics 118(July), 58-64. https://doi.org/10.1016/j.ijmedinf.2018.07.009 [ Links ]
Acquah-Swanzy, M., 2015. Evaluating electronic health record systems in Ghana: the case of Effia Nkwanta regional hospital (Master's thesis, UiT Norges arktiske universitet). [ Links ]
Alberts, B., Kirschner, M.W., Tilghman, S. & Varmus, H., 2014, 'Rescuing US biomedical research from its systemic flaws', Proceedings of the National Academy of Sciences 111(16), 5773-5777. [ Links ]
Angeles, R., 2014, 'Using the technology-organization-environment framework for analyzing Nike's Considered Index green initiative, a decision support system-driven system', Journal of Management and Sustainability 4(1), 96-113. [ Links ]
Aquino, R.P., Barile, S., Grasso, A. & Saviano, M., 2018, 'Envisioning smart and sustainable healthcare: 3D Printing technologies for personalized medication', Futures 103, 35-50. https://doi.org/10.1016/j.futures.2018.03.002 [ Links ]
Barbosa, G., Takako, P. & Sadok, D., 2020, 'An internet of things security system based on grouping of smart cards managed by field programmable gate array R', Computers and Electrical Engineering 74(2019), 331-348. https://doi.org/10.1016/j.compeleceng.2019.02.013 [ Links ]
Cripps, H., Standing, C. & Prijatelj, V., 2012, 'Smart health care cards: Are they applicable in the Australian context?', In 25th Bled eConference eDependability, Slovenia, 17 June, p. 5.
DeLone, W.H. & McLean, E.R., 1992, 'Information systems success: The quest for the dependent variable', Information Systems Research 3(1), 60-95. [ Links ]
DeLone, W.H. & McLean, E.R., 2003, 'The DeLone and McLean model of information systems success: A ten-year update', Journal of Management Information Systems 19(4), 9-30. [ Links ]
dos Santos Brito, K., da Silva Costa, M.A., Garcia, V.C. & de Lemos Meira, S.R., 2014, 'Brazilian government open data: implementation, challenges, and potential opportunities', In Proceedings of the 15th annual international conference on digital government research, Aguascalientes, Mexico, June 18-21, 2014, pp. 11-16.
Esewe, R.E., 2017, 'Nigeria developing strategies to enhance implementation of early Kangaroo Mother Care (KMC)', Doctoral dissertation, University of Western Cape. [ Links ]
El-Yafouri, R. & Klieb, L., 2014, 'Electronic medical records adoption and use: Understanding the barriers and the levels of adoption for physicians in the USA', In 2014 IEEE 16th International Conference on e-Health Networking, Applications and Services (Healthcom), IEEE, pp. 506-512. https://doi.org/10.1109/healthcom.2014.7001894
Furusa, S.S. & Coleman, A., 2018, 'Factors influencing e-health implementation by medical doctors in public hospitals in Zimbabwe', South African Journal of Information Management 20(1), 1-9. https://doi.org/10.4102/sajim.v20i1.928 [ Links ]
Howell, P., Sharman, R., Das, S. & Abdelhamid, M., 2016, 'Patient Adoption of Smart Cards', In Twenty-second Americas Conference on Information Systems, San Diego, 2016.
Hsu, P.F., Yen, H.R. & Chung, J.C., 2015, 'Assessing ERP post-implementation success at the individual level: Revisiting the role of service quality', Information and Management 52(8), 925-942. [ Links ]
Hung, S.Y., Tsai, J.C.A. & Chuang, C.C., 2014, 'Investigating primary health care nurses' intention to use information technology: An empirical study in Taiwan', Decision Support Systems 57(1), 331-342. https://doi.org/10.1016/j.dss.2013.09.016 [ Links ]
Iyamu, T., 2021, Applying theories for information systems research, Routledge, Milton Park.
Jeyaraj, A., 2020, 'DeLone & McLean models of information system success: Critical meta-review and research directions', International Journal of Information Management 54(November 2019), 102139. https://doi.org/10.1016/j.ijinfomgt.2020.102139 [ Links ]
Kaiser, H.F., 1974, 'An index of factorial simplicity', Psychometrika 39(1), 31-36. [ Links ]
Kilsdonk, E., Peute, L.W. & Jaspers, M.W., 2017, 'Factors influencing implementation success of guideline-based clinical decision support systems: a systematic review and gaps analysis', International Journal of Medical Informatics 98, 56-64. [ Links ]
Kiwanuka, A., 2015, 'Acceptance process : The missing link between UTAUT and diffusion of innovation theory', American Journal of Information Systems 3(2), 40-44. https://doi.org/10.12691/ajis-3-2-3 [ Links ]
Lau, F. & Kuziemsky, C., 2016, 'Handbook of eHealth evaluation: an evidence-based approach', Chapter 9, University of Victoria, Victoria, BC, Canada.
Maguraushe, K., 2021, 'Development of a diagnostic instrument and privacy model for student personal information privacy perceptions at a Zimbabwean university', Doctoral dissertation.
Maeko, M.E. & Van Der Haar, D.T., 2018, 'A Framework for User Awareness and Acceptance of Smart Card and Fingerprint-Based Access Control to Medical Information Systems in South Africa', In 2018 IST-Africa Week Conference (IST-Africa), May 9-11, 2018, p. 1.
Mollaoglu, S., Chergia, C., Ergen, E. & Syal, M., 2016, 'Diffusion of green building guidelines as innovation in developing countries', Construction Innovation 16(1), 1-29. https://doi.org/10.1108/CI-09-2014-0045 [ Links ]
Odhiambo, M.E., 2015, 'A framework for implementation of e-health in Kenya public hospitals', Doctoral dissertation, Strathmore University. [ Links ]
Pallant, J., 2020, SPSS survival manual: A step by step guide to data analysis using IBM SPSS, 7th edn., McGraw-hill education, Routledge, UK, March 3, p. 378.
Petter, S., Delone, W. & McLean, E.R., 2013, 'Information systems success: The quest for the independent variables', Journal of Management Information Systems 29(4), 7-62. https://doi.org/10.2753/MIS0742-1222290401 [ Links ]
Rogers, E.M., Singhal, A. & Quinlan, M.M., 2014, 'Diffusion of innovations', In An integrated approach to communication theory and research, pp. 432-448, Routledge, New York.
Srur, B.L. & Drew, S., 2012, 'Challenges in designing a successful e-health system for Australia', In 2012 International Symposium on Information Technologies in Medicine and Education, IEEE, Griffith University, Australia, Vol. 1, pp. 480-484.
Steininger, K., Stiglbauer, B., Baumgartner, B. & Engleder, B., 2014, 'Factors explaining physicians' acceptance of electronic health records', In 2014 47th Hawaii international conference on system sciences, IEEE, pp. 2768-2777. https://doi.org/10.1007/s12553-018-0277-8
Tsai, C.L. & Chang, H.C., 2016, 'Evaluation of critical factors for the regional innovation system within the HsinChu science-based park', Kybernetes 45(4), 699-716. https://doi.org/10.1108/K-02-2015-0059 [ Links ]
 Correspondence:
Correspondence:
Lovemore Motsi
Motsil@Unisa.ac.za
Received: 13 Sept. 2022
Accepted: 25 Jan. 2023
Published: 31 Mar. 2023


{kind=link}