










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkJournal of Energy in Southern Africa
On-line version ISSN 2413-3051
Print version ISSN 1021-447X
J. energy South. Afr. vol.31 n.4 Cape Town Nov. 2020
http://dx.doi.org/10.17159/2413-3051/2020/v31i4a8362
ARTICLES
Sustainable electricity for sustainable health? A case study in North-Western Zambia
Lizzie CaperonI, *; Lina Brand-CorreaII
IBradford Institute for Health Research, Bradford Royal Infirmary, Bradford, UK, BD9 6RJ. ORCID: https://orcid.org/0000-0001-5204-170X
IIUniversity of Leeds, Leeds, LS2 9JR, UK. ORCID: https://orcid.org/0000-0003-3142-8766
ABSTRACT
This study explores the under-researched link between clean energy and public health outcomes, and offers new insights into the link between wider access to clean energy and progress towards health outcomes, in particular the prevention and treatment of non-communicable diseases such as diabetes. This is the first study to consider the impact of a run-of-river hydropower plant (RORHP) in a remote rural community in Zambia in relation to health outcomes. Exploring this relationship establishes how the health benefits which renewable energy can bring can be capitalised upon to meet the health-related objectives of the United Nations sustainable development goals. Workshops and semi-structured interviews were conducted with a range of stakeholders including community members, health workers, business owners, and key people involved with the plant, to establish health and social impacts of the introduction of electricity in the community of Ikelenge. Findings are used to establish both synergies and trade-offs of the RORHP on the health of the community, and recommendations are made for the continued improvement of health following the introduction of the RORHP, to achieve further progress towards meeting SDG targets.
Keywords: renewable energy; sustainability; rural settings; non-communicable diseases, diabetes, well-being, community health, diet, clean energy
1. Introduction
The sustainable development goals (SDGs) are a collection of 17 global goals adopted by the United Nations member states in 2015. Goal 3 aims to ensure healthy lives and promote well-being for all at all ages (United Nations, 2019a), and is thus the most closely related to public health outcomes. Simultaneously, ensuring access to affordable, reliable, sustainable and modern energy for all is the focus of Goal 7 (United Nations, 2019b). Previous research on the link between clean energy and health outcomes (on the synergies between SDGs 3 and 7) has focused mainly on respiratory diseases caused by indoor air pollution from dirty cooking fuels (World Health Organisation, 2018a; Jung & Huxham, 2019; Naz et al., 2017). However, the link between clean energy and public health outcomes is still underexplored.
This study offers new insights into the link between wider access to clean energy and progress towards health outcomes, in particular the prevention and treatment of non-communicable diseases (NCDs) such as diabetes - one of the targets of SDG 3 is to tackle the growth in NCDs. Using a qualitative approach, access was gained to an under-researched population in a remote community in rural north-western Zambia, focusing on the community of Ikelenge. This is the first study to consider the impact of a run-of-river hydropower plant (RORHP) in such a community in relation to health outcomes. Through exploring this relationship, the study sought to establish how the health benefits which renewable energy can bring can be capitalised upon to meet the health-related objectives of the SDGs. The paper adds empirical support and new insights to the existing literature on synergies and trade-offs between energy and the SDGs (Fuso Nerini et al., 2018; Roy et al., 2018).
Workshops (n=2) and semi-structured interviews (n=16) were conducted with a range of stakeholders including householders (n=8), health workers (n=3), business owners (n=2) and key people involved with the RORHP (named Zengamina) (n=3). The findings help to reveal both positive and negative impacts on the health of the community and local health system. Recommendations are then made for the continued improvement of health following the introduction of the RORHP, to achieve further progress towards meeting SDG targets.
2. Case study context, methods and data
2.1 Case study context: diet, health care and energy
The case study was carried out in Zambia's North-Western Province, in the district of Ikelenge, which borders on the Democratic Republic of Congo (DRC) and Angola. Staple crops in the region are cassava and maize, and subsidy crops include pumpkins, sweet potatoes and yams, leafy vegetables, tomatoes and cabbage (Pesa, 2014). Over the twentieth century, cassava was promoted by the government and is now the preferred staple for people in the north-west of Zambia (Pesa, 2014). In Ikelenge, these foods are mainly obtained from subsistence agriculture, with 70% of households reporting farming as their main economic activity (Zambia Statistics Agency, 2015). Other avenues for food provisioning included hunting and animal husbandry. However, because of high competition in markets, the commercial rearing of stock failed to be successful in the region (Pesa, 2014). Thus, the diet in Ikelenge district is mainly vegetables (97% of households have vegetables more than five times per week), while meat and fish are rare in people's diet (93% of households have meat and fish three times per month or less) (Zambia Statistics Agency, 2015). In addition to vegetables, pineapple production has been sporadically successful in the region over time, becoming a significant part of people's diet as well as a source of income, with several pineapple-processing factories being opened over the last half century. However, the Ikelenge's most important export has been hampered by problems exporting the fruit, including problems in transporting produce beyond the region (Malama, 2014). The Ikelenge district is so closely associated with pineapple production that is it referred to as 'pineapple country' in the rest of Zambia.
The region's traditional diet of cassava and pineapples, both high in sugar, has contributed to reportedly disproportionately high levels of diabetes and high blood glucose there. NCDs are estimated to account for 29% of deaths in Zambia, with risk of premature death at between 30-70 years at 18% in 2016 (World Health Organisation, 2018b). The Zambian government has developed an NCD strategic plan based on the WHO Global Action Plan for NCDs 2013-2030 (World Health Organisation, 2015), though there is criticism that the plan does not cover all NCDs adequately (Mukanu et al., 2017). There is a 3.4% prevalence of reported diabetes in Zambia, with rates increasing year on year (International Diabetes Federation, 2020).
Research took place in various locations around the town of Ikelenge itself, including community halls, homes of residents, and the Kalene Hill hospital - a missionary hospital set up in 1905, with the present hospital built in the 1950s (Kalusa, 2014). It serves the Ikelenge district area of approximately 32,919 people (City Population, 2010), and patients who travel from neighbouring Angola and DRC, whose borders are approximately 15 miles away. Estimates state that the hospital caters for 44,000 people (Kalene Mission Hospital Online, 2017), though health workers at the hospital say that this is an underestimate, calculating double this number, owing to many people travelling long distances to access the hospital. The hospital has four wards (split into male/female and children's wards), each holding around forty patients, as well as a maternity unity (30 patient capacity) and an outpatient's unit run by a team of six nurses who process up to 200 patients per day (Kalene Mission Hospital Online, 2017). Surgery is conducted in two operating theatres, one used for major and one for minor surgery. The hospital is home to a nursing school, which takes students from the local area.
Zambia in general has a very low access rate to electricity (31%), meaning the majority of its population lives with no electricity. In rural areas, such as Ikelenge, the rate is between 4% and 11% (Sustainable Energy for All, 2020). The Zengamina RORHP is an infrastructure initiative that clearly contributes to SDG 7, developed through the independent North West Zambia Development Trust (NWZDT) (North West Zambia Development Trust, 2013). It was inaugurated in July 2007 with a generating capacity of 750kW, and currently has a 35km transmission line that supplies electricity to the community Hospital, local schools, and around 1000 villagers from Ikelenge (North West Zambia Development Trust, 2013).
2.2 Methods
Qualitative methods were used, specifically participatory workshops and semi-structured interviews (SSIs), aimed at producing socially useful knowledge using a pragmatic approach (Feilzer, 2010). The goal was to understand the changes which had occurred to health systems and outcomes as a result of the introduction of electricity in the region. The fieldwork, carried out in October 2018, was part of a broader project analysing the role of energy in human wellbeing. The workshops followed the Human Scale Energy Services (HuSES) framework (Brand-Correa et al., 2018). Participatory workshops have been shown to stimulate discussion between participants who have commonality and to encourage discussion and consensus (Skovdal & Cornish, 2015). Dialogues which can emerge from workshops stem from listening to narratives and can be seen as the basis of praxis - the unity of theory and action (Freire, 1970) . These dialogues can offer an important insight as a tool of democratic communication and can form the basis of transformational change (Ledwith & Springett, 2010). Workshops are a well-tested participatory technique for eliciting authentic research contributions (Green & Thorogood, 2009; Breuer et al., 2014; Carr et al., 2003; Cote-Arsenault & Morrison-Beedy, 2005; Kitzinger, 1995; Tausch & Menold, 2016; Chambers, 2012).
An iterative approach was taken when developing the SSI guides, which consisted of 20 open questions structured around the concepts of human needs (Max-Neef et al., 1992; Doyal & Gough, 1991) and energy services (Cullen & Allwood, 2010; Grubler et al., 2012), derived from literature reviews of previous research. For the purposes of this paper, the questions on the needs of 'subsistence' and 'protection' were particularly relevant. Two community member interviews were undertaken as pilots. The research team (LC, LBC) reflected on the pilot interviews and revised and improved the interview guides, adding probes on the use of the hospital and opinions about dietary behaviour change in the community.
2.3 Data collection
Two workshops were conducted in community centres that were well known to community members and easily accessible. The advice of our local research assistants was to conduct separate workshops for men and women, in the belief that each group would speak more freely if separated. There were 16 men and 13 women in the workshops. The workshops were facilitated by the two lead researchers (LC and LBC), and undertaken in the local language, Lunda, with the help of a local community member who provided simultaneous translation.
Interviews were undertaken in the houses of the community members (n=8), workplaces of the community members (n=3) and a hospital (n=4). A total of 15 interviews were conducted, the maximum pragmatic number, given the time and budget constraints of the project. All locations provided privacy and a quiet space to allow participants the opportunity to speak calmly and openly. Interviews were conducted by the two lead researchers either in English or through a translator who was a local facilitator and member of the community. Reflective field notes were made by researchers straight after the interviews, in English, to inform subsequent interviews. All interviews and workshops in the local language were transcribed from audio recordings into English, based on the simultaneous translation done by the local facilitator. All interviews in English were transcribed from the audio recordings in English.
The interviews were of purposively-selected community members (n=8), health workers (n=4) and decision makers (n=3). Health workers were from the only hospital in the region, and the decision-makers were native to the region, involved in the building process and managed the hydroelectric power plant. Participants were approached by a local facilitator known to the community in their home or place of work and asked if they would like to participate in the study. If they agreed, one of the lead researchers returned to their home/place of work at a later date and interviews were conducted with the local facilitator present.
Both workshops and interviews purposively included people from a range of ages and professions and both genders, to demonstrate important shared patterns that cut across the cases (Palinkas et al., 2015). Tables 1 and 2 summarise interview and workshop participants.

In line with established ethical requirements, both information sheets and consent forms were provided to all participants in the workshops and interviews. The study received ethical approval from the Research Ethics Committee, University of Leeds (Leeds, LS2 9LJ, United Kingdom).
2.4 Data analysis
Like the sampling and data collection process, the data analysis took an iterative form. Data was constantly analysed and refined as it was collected, with the majority of the in-depth data analysis conducted at the end of the study. Data was analysed using the framework approach (Gale, Heath, Cameron, Rashid, & Redwood, 2013). This approach was selected to allow themes to emerge inductively from the data, and also to allow pre-determined objectives to lead to deductive analysis (Feilzer, 2010). Two members of the research team (LC, LBC) independently analysed a sample of three interviews and then through discussion reached a consensus on a framework for the themes, including a priori and emergent ones. LC then analysed the other interviews, discussing any amendments to the analysis framework with LBC. The themes in the framework analysis were generated from the majority of the respondent responses. Each theme had been referred to by at least one group of respondents we interviewed, and in many cases by multiple groups interviewed. Theme 1 (Electricity leads to changes in dietary consumption due to refrigeration) was discussed by all community members, business owners and in both workshops. Theme 2 (Electricity leads to changes in the health workforce) was referred to by all health workers interviewed. Theme 3 (Electricity leads to a change in hospital functionality) was discussed by all health workers interviewed, some community members, two of three decision makers, and was discussed in both workshops. Theme 4 (Electricity contributes to an increase in diagnosis of NCDs such as diabetes) was discussed by health workers, community members and in both workshops. Such repeated discussion of the main themes by different groups of respondents allowed the analysis to be structured with these key themes, confidently and with supporting statements from respondents.
3. Results: Key themes
Using the analytical approach discussed, the four key themes mentioned above emerged from the data. These themes were generated from the majority of our respondent responses, and there was agreement within and across different respondent groups about their significance.
3.1 Theme 1: Electricity leads to changes in dietary consumption due to refrigeration
Since the construction and coming into operation of the RORHP, several households which had adequate access to disposable income had bought refrigerators for their homes to store food. Those householders who had bought refrigerators (both of the business owners and three of the community members, including additional community members referred to in both workshops) stated that doing so meant they had increased the amount of refrigerated food they consumed. This was apparent in the school head teacher's home:
When I moved here I bought the fridge. With the fridge here we can keep food like meat, fish and vegetables for longer. But sometimes the power goes off and the food goes off.
Community member 1
These householders were able to store a wider range of foods than they consumed before they had access to electricity. Newly consumed food and drink included meat and fish products, and fizzy drinks stored to be drunk chilled. However, as mentioned by the head teacher, the lack of stability of the electricity supply meant that sometimes, when the power supply was stopped, food stored in fridges would need to be eaten immediately or it would go off.
Refrigerators were also shared by many community members, with those able to purchase them sharing with their families who had no access, or with other disadvantaged members of the community, such as widows who had very limited resources. Participants in the female workshop discussed the process of sharing fridge space with other women in the community:
We let her [ayoung mother of the community] bring some items to put in our fridge because she has no access to one in her home.
Female workshop participant
Sharing space in fridges meant that even the poorest in the community occasionally ate fish or meat, which they had not been able to do before the RORHP was introduced.
We can eat fish and meat now that we can save it in the fridges. Before we only ate cassava and vegetables some days.
Community member 3
Refrigeration also opened up economic opportunities for some enterprising members of the community, and existing shop owners, including the two business owners interviewed, who began importing products such as fizzy drinks and salted fish to sell:
I have had this shop for 17 years.... Things are changing now I have electricity... people come here to charge their phones and I can store drinks in the fridge to sell. The electricity is good for my business.
Business owner 1
This enterprising spirit shows that refrigeration widened the potential for the community to expand their diets, and most participants stated that the introduction of fish and meat in their diet was a positive and aspirational addition. They discussed how fish and meat could be consumed regularly, as well as for special occasions. However, the new food and drink they consumed can have mixed health benefits, with householders excited about the new possibilities to consume, without expressing an understanding of the consequences to their health, particularly of sugary beverages sold by shop owners.
Furthermore, all householders interviewed who owned refrigerators, and both business owners, expressed frustration at power outages and load shedding which often led to a loss of their perishable goods, particularly meat. (Load shedding is a common occurrence in Zambia, even in the big urban centres and the capital city of Lusaka. Frustration with power outages shows how quickly high expectations on security of supply arise, despite the situation likely being equal or even worse in the rest of the country.) The power outages were unpredictable, often resulting from changes in local weather events, such as storms, high winds or uncharacteristically long rainy/dry seasons (which will only get more frequent and more severe as climate change worsens). This reinforces the importance of reliable access to electricity (Harvey, 2014), otherwise the consumption of 'new food' becomes sporadic.
3.2 Theme 2: Electricity leads to changes in the health workforce
All health workers interviewed at the Kalene hospital stated that, since the introduction of electricity, students who train there are more willing to stay to work there, attributing this to the advantages brought by electricity. One said that since the introduction of electricity to the hospital, which replaced the diesel generator (now used as a backup option only), more health workers had been willing to come to this remote area from urban areas such as Lusaka, where she had come from. She told us that other remote areas in Zambia placed health workers in hospitals that often did not have electricity, and therefore they had tougher working environments and fewer comforts outside of work hours:
It is good here now there is electricity, we can watch TV, listen to music, charge our phones. We are lucky compared with other places [health centres] where they do not have these things. More people want to come here to work now because it is better.
Health worker 3
However, despite the benefits stated which have come from the introduction of electricity to the hospital, there remain drawbacks, such as a lack of connectivity due to a lack of internet or mobile connection at the hospital. This can cause social problems amongst the health workers:
Being away from family is not a problem for me, but communication is a problem. Communication is very important to maintain relationships. Some of us have had to break up with our partners. I had to break up with my boyfriend because we could not communicate properly. It is very hard not having the network [mobile phone network connection] here.
Health worker 3
Though the health workers raised the issue of lack of access to mobile networks from the hospital, which had impacts on their relationships with family and friends outside Kalene, they were able to get a mobile signal in places at walking distance from the hospital grounds, such as the nearby airstrip. Furthermore, the owner of the RORHP told us of plans to install a new communication mast next to the hospital. Overall, we found that newly employed health workers wanted to work at Kalene hospital and the workforce was more easily retained than it had been previously when there was no, or limited, access to electricity. This marked a change from the limited staffing (one health worker reported they were working at only 40% workforce capacity) prior to the introduction of the RORHP. However, despite recent placements of workers from urban areas such as Lusaka, the hospital remains understaffed, with only two doctors employed, which raises wider questions about resourcing of rural hospitals in Zambia. Several nurses interviewed spoke about their desire to undertake medical training to become doctors, but stated that financial barriers had prevented them from doing so:
I want to do medical training but I need sponsorship because I cannot afford it. I would be a doctor here because doctors are desperately needed.
Health worker 1
As this health worker states, a lack of affordable doctor training opportunities limits the potential for improving the workforce in such remote rural areas as Ikelenge. Also, further medical training opportunities for staff at Kalene in education institutions elsewhere would not guarantee retention of the workforce in the local health system. Overall, despite an increase in the health workforce due to the benefits brought by the introduction of electricity by RORHP, there remain issues with capacity, capability and training of the workforce, which cannot be addressed by the introduction of electricity alone.
3.3 Theme 3: Electricity leads to a change in hospital functionality
Electricity had increased the hospital's functional - ity, allowing improved healthcare after dark, with health professionals, who had previously not been able to care easily for patients on wards without light, now having access to 24-hour light. This could ensure round-the-clock care for patients. Furthermore, since the RORHP was built, the Zambia government built an electricity-powered mortuary at Kalene hospital, which can accommodate six bodies. Health workers discussed the introduction of the mortuary as highly beneficial, stating it marked an improvement in the functioning of the hospital and the services it can offer. They said that it also helped to limit the spread of disease from bodies which cannot be buried immediately. Health workers also told us that improved facilities and staffing had led to increased numbers of people attending the hospital. One health worker described how one patient had come from the DRC:
One patient walked here for two weeks from DRC. She had heard that the hospital had good facilities and could treat her.
Health worker 2
Patients were travelling great distances to the hospital, which now has improved facilities. Health workers stated that the reputation of the hospital had increased due to these improved facilities. Participants in both workshops corroborated this by stating that they were more likely to visit the hospital now they had heard that the equipment and facilities had improved since the introduction of electricity. There are still many limitations to the facilities available in the hospital, particularly in providing adequate healthcare to the immense catchment population, but, the introduction of electricity has clearly increased the hospital's reputation and ability to provide improved care to patients.
3.4 Theme 4: Electricity contributes to an increase in diagnosis of NCDs
Diagnosis of NCDs such as diabetes had also improved with the introduction of glucometers and lighting in the laboratory, which could function outside daylight hours following the introduction of electricity. Lighting in the laboratory allowed for quicker test results. Since the introduction of RORHP, health workers stated that Kalene hospital had diagnosed an increased number of cases of diabetes with glucometers and blood sugar tests.
Furthermore, due to this remote hospital having electricity, unlike other remote hospitals, a nutritionist had been encouraged to accept a full-time placement (see theme 2), providing much needed nutritional counselling to those with high blood glucose levels, diabetes, high blood pressure and other NCDs. Health workers at Kalene hospital stated that there had always been a high number of diabetes cases at the hospital, likely to be related to the cultivation consumption of staples cassava and pineapples:
We have a lot of diabetes here. The local foods are high in starch and sugar. It is not surprising.
Health worker 2
Although the nutritionist can now counsel recently diagnosed patients, health workers said that the nutritionist is rarely able to make a difference to patients' behaviour, due to a combination of reluctance to go against cultural norms and lack of access to alternative food, particularly for those patients without access to refrigeration. Participants in both workshops did not show an awareness of NCDs such as diabetes, and had not received any nutritional education about the consumption of, for example, chilled sugary drinks and how this could increase blood sugar levels. Whilst rates of diagnosis of diabetes are increasing in the community, awareness of the environmental factors leading to diabetes, including the increase in refrigeration of unhealthy foods, were not understood.
4. Discussion
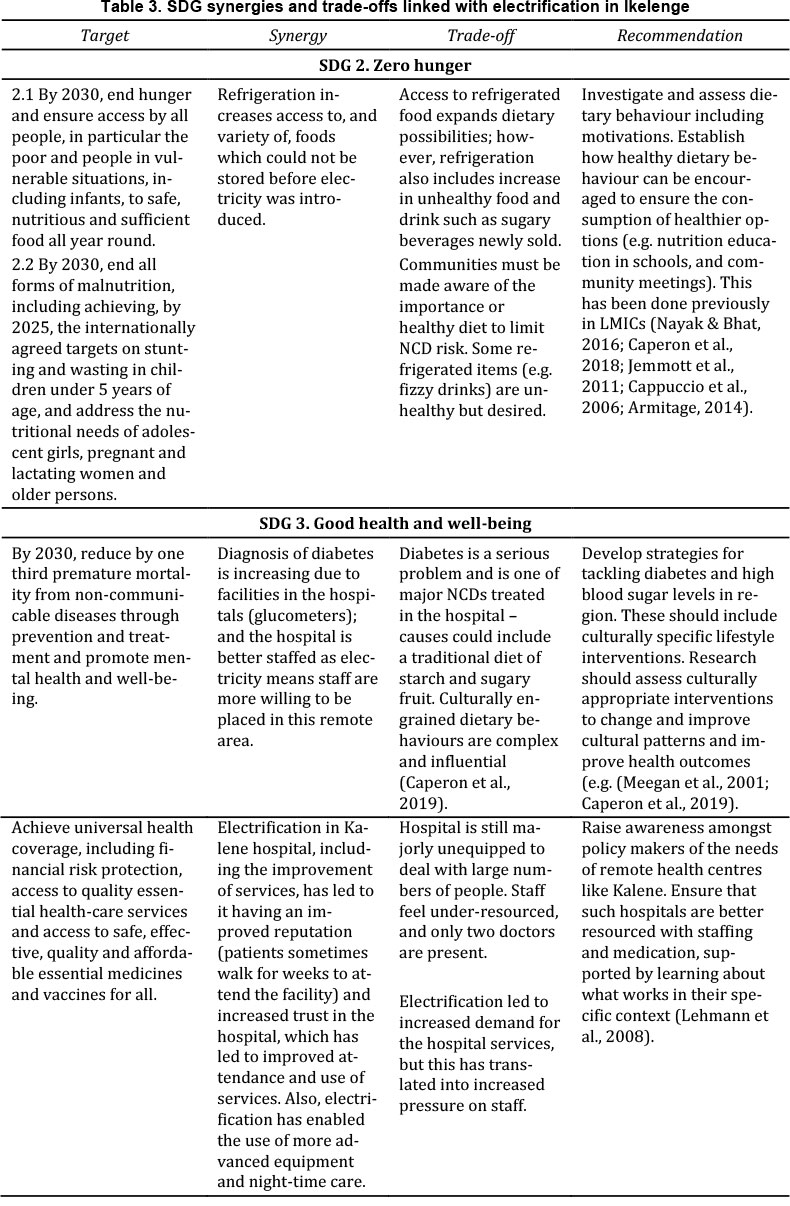
The study's findings shed light on the relationship between the introduction of electricity in the rural area of Ikelenge, and health- and social-related outcomes for the local population. The findings are unique in exploring such a relationship and, to the best of our knowledge, no literature documents such a relationship. The findings relate to SDGs 2 (Zero hunger) and 3 (Good health and well-being) (see Table 3), through the implementation of a project that contributes to SDG 7 (Sustainable energy for all).
Evidently, refrigeration has had an impact on the diets of those who have access to electricity, adding more variety to traditional diets based on cassava and pineapples, by introducing the possibility of storing and consuming food such as meat and salted fish. Many participants viewed these as positive changes to their health and lifestyles. Despite this, refrigeration led to greater consumption of sugary bottled drinks, as a result of local business owners starting to sell them. Little research has explored the relationship between refrigeration and dietary change in low-income country contexts. However, the benefits of refrigeration to extend food freshness are widely acknowledged (Earley, 2014; The Borgen Project, 2018). Nutrition transition has been observed in low-income countries, including dietary change such as that found in Ike-lenge (Popkin et al., 2012). Links have been firmly established between the consumption of sugary drinks and an increase risk in NCDs (Te Morenga et al., 2013; World Health Organisation, 2019), and links between sugary drinks and diabetes in particular have been well established (Malik et al., 2010).
This link with diabetes is particularly relevant in the context of Ikelenge where the traditional diet of cassava and pineapples has likely contributed to the high rates of diabetes reported at Kalene hospital. Culturally defined dietary behaviours like this have been shown to be complex and influential in low-income settings similar to Ikelenge (Caperon et al., 2019). An approach to tackle these engrained behaviours could be to develop strategies for tackling diabetes which could include behavioural-change strategies which incorporate cultural understanding (Meegan et al., 2001). Such culturally appropriate interventions should aim to contribute to SDG 3 (Good health and well-being) including reducing by one third premature mortality from NCDs (United Nations, 2019a).
The second SDG, on zero hunger, states that all people should have access to nutritious and sufficient food all year round (United Nations, 2019b). The introduction of refrigeration in Ikelenge has led to the potential to allow for different food types to be stored and consumed and increase the variety of food available. However, it is apparent that the introduction of refrigeration is a double-edged sword as discussed in the paragraph above. Therefore, such dietary changes need to be accompanied by nutrition education and behavioural measures to ensure that unhealthy food and drink is consumed in moderation. Such measures have been introduced in other low-income country settings (Caperon et al., 2018; Jemmott et al., 2011; Armi-tage, 2014; Cappuccio et al., 2006), though none have been introduced in response to electrification. This presents a gap in the research and an opportunity for developing healthy living interventions to accompany new clean energy projects which change lifestyle habits in low-income settings such as Ikelenge.
Within SDG 3 is the objective to achieve universal health coverage, including access to essential healthcare services. According to our participants, access to Kalene hospital remains problematic, with one patient walking for two weeks to attend. Our study found that the hospital remains under-equipped to deal with the huge numbers of people it serves. However, since the introduction of electricity, there has been an increase in the ability of the hospital to treat patients using improved methods and equipment. Despite new facilities such as 24-hour lighting on wards and in the laboratory, the health workers still felt under-resourced and only two doctors were employed. Solutions to address these ongoing challenges could include raising awareness amongst policymakers of the needs of remote health centres like Kalene. This is been seen as a priority by the WHO and is advocated by other research from similar low-income settings (World Health Organisation, 2010; Lehmann et al., 2008).
Such studies advocate learning about what works best in specific rural contexts, such as Ikelenge, considering wider political, economic and policy contexts, to meet the challenges of improved resourcing. These improvements are needed to improve the functioning, adaptability and strength of remote, local health systems in low-income settings.
Closely connected to the need for improved resourcing in health settings like Kalene hospital, SDG 3 also advocates for the development, training and retention of the health workforce in low-income countries, especially in the least-developed countries, like Zambia. Our data showed that movement has occurred towards this goal since the introduction of electricity to Kalene hospital, which is consistent with findings for Sierra Leon (Wurie et al., 2016) and Kenya (Ojakaa et al., 2014). More staff were willing to be placed at Kalene due to the modern comforts expected from electricity, such as television. Mobile phone coverage was still patchy and health workers stated that there was a lack the funding for them to receive further training. Therefore, there is a need to raise awareness amongst policymakers of the need to upskill medical professionals to ensure hospitals are adequately staffed and resourced, as others also advocate (Bangdiwala et al., 2010; Anyangwe & Mtonga, 2007).
Table 3 shows the targets outlined by the SDGs in relation to improved health outcomes, states the synergies made by the RORHP introduction of clean energy, as well as the emerging or persisting tradeoffs associated with this change, and our recommendations for further improvements aligned with the SDG aims.
5. Conclusion
This research has found that first-time access to electricity can lead to improvements in health and social outcomes, but also challenges. We found that the Zengamina hydroelectric power generation plant project in rural north-west Zambia brought about improvements to health care delivery, diagnosis of NCDs (particularly diabetes), retention of health workers and changes in dietary behaviour due to increased ability to refrigerate edible goods. There are, however, challenges arising from the changes brought about by the introduction of electricity, such as increased consumption of refrigerated sugary beverages. We have proposed how these challenges can be met with strategies to, for example, improve dietary behaviour within cultural boundaries. These measures aim to reduce the risk factors for non-communicable diseases, which are on the rise globally and especially in low-income countries. Overall, electrification holds great potential in low-income countries if it is carefully implemented. If such electrification is from clean energy sources, as it was in this case, it further supports the synergies between sustainable development goals and builds long-term environmental sustainability.
Acknowledgements
This work was undertaken as part of the Leverhulme Trust's Research Leadership Award 'Living well within limits' (RL2016-048) project awarded to Prof Julia K. Steinberger.
Author contributions
The authors jointly designed the study, undertook field-work and collected the data, and wrote the paper. Lizzie Caperon performed the data analysis and Lina Brand-Correa reviewed the analysis process.
References
Anyangwe, S. & Mtonga, C. 2007. Inequities in the Global Health Workforce: The Greatest Impediment to Health in Sub-Saharan Africa. International Journal of Environmental Research and Public Health, 4(2): 93-100. http://www.mdpi.com/1660-4601/4/2/93 17 January 2020. [ Links ]
Armitage, C.J. 2014. Evidence That Self-Incentives Increase Fruit Consumption: A Randomized Exploratory Trial Among High-Risk Romanian Adolescents. Prevention Science, 15(2): 186-193. http://link.springer.com/10.1007/s11121-012-0346-6 17 January 2020. [ Links ]
Bangdiwala, S.I., Fonn, S., Okoye, O. & Tollman, S. 2010. Workforce Resources for Health in Developing Countries. Public Health Reviews, 32(1): 296-318. https://doi.org/10.1007/BF03391604. [ Links ]
Brand-Correa, L.I., Martin-Ortega, J. & Steinberger, J.K. 2018. Human Scale Energy Services: Untangling a 'golden= thread'. Energy Research and Social Science, 38(January): 178-187. [ Links ]
Breuer, E., De Silva, M.J., Fekadu, A., Luitel, N.P., Murhar, V., Nakku, J., Petersen, I. & Lund, C. 2014. Using Workshops to Develop Theories of Change in Five Low and Middle Income Countries: Lessons from the Programme for Improving Mental Health cCare (PRIME). International Journal of Mental Health Systems, 8: 15. [ Links ]
Caperon, L., Arjyal, A., K. C., P., Kuikel, J., Newell, J., Peters, R., Prestwich, A. & King, R. 2019. Developing a socio-ecological model of dietary behaviour for people living with diabetes or high blood glucose levels in urban Nepal: A qualitative investigation. PLOS ONE, 14(3): e0214142. https://doi.org/10.1371/journal.pone.0214142. [ Links ]
Caperon, L., Sykes-Muskett, B., Clancy, F., Newell, J., King, R. & Prestwich, A. 2018. How effective are interventions in improving dietary behaviour in low- and middle-income countries? A systematic review and meta-analysis. Health Psychology Review, 12(3): 312-331. https://www.tandfonline.com/doi/full/10.1080/17437199.2018.1481763 5 July 2019. [ Links ]
Cappuccio, F.P., Kerry, S.M., Micah, F.B., Plange-Rhule, J. & Eastwood, J.B. 2006. A Community Programme to Reduce Salt Intake and Blood Pressure in Ghana. BMC Public Health, 6(1): 13. https://doi.org/10.1186/1471-2458-6-13. [ Links ]
Carr, A., Hewlett, S., Hughes, R., Mitchell, H., Ryan, S., Carr, M. & Kirwan, J. 2003. Rheumatology Outcomes: the Patient's Perspective. The Journal of Rheumatology, 30(4): 880-883. [ Links ]
Chambers, R. 2012. Participatory Workshops: A Sourcebook of 21 Sets of Ideas and Activities. London: Earthscan. City Population. 2010. Ikelenge (District, Zambia) - Population Statistics, Charts, Map and Location. https://www.citypopulation.de/php/zambia-admin.php?adm2id=0802 14 January 2020. [ Links ]
Cote-Arsenault, D. & Morrison-Beedy, D. 2005. Maintaining Your Focus in Focus Groups: Avoiding Common Mistakes. Research in Nursing & Health, 28(2): 172-179. [ Links ]
Cullen, J.M. & Allwood, J.M. 2010. The efficient use of energy: Tracing the global flow of energy from fuel to service. Energy Policy, 38(1): 75-81. [ Links ]
Doyal, L. & Gough, I. 1991. A Theory of Human Need. London: The Macmillan Press. [ Links ]
Earley, K. 2014. Tech Can Prevent Huge Food Waste Problems in Developing Countries. The Guardian. https://www.theguardian.com/sustainable-business/2014/dec/18/technology-prevent-waste-food-developing-countries 6 April 2020. [ Links ]
Feilzer, M.Y. 2010. Doing Mixed Methods Research Pragmatically: Implications for the Rediscovery of Pragmatism as a Research Paradigm. Journal of Mixed Methods Research, 4(1): 6-16. http://mmr.sagepub.com/content/4/1/6.abstract. [ Links ]
Freire, P. 1970. Pedagogy of the Oppressed. New York: Herder and Herder. [ Links ]
Fuso Nerini, F., Tomei, J., To, L.S., Bisaga, I., Parikh, P., Black, M., Borrion, A., Spataru, C., Castán Broto, V., Anandarajah, G., Milligan, B. & Mulugetta, Y. 2018. Mapping synergies and trade-offs between energy and the Sustainable Development Goals. Nature Energy, 3(1): 10-15. [ Links ]
Green, J. & Thorogood, N. 2009. Qualitative Methods for Health Research. London: Sage. [ Links ]
Grubler, A., Johansson, T.B., Mundaca, L., Nakicenovic, N., Pachauri, S., Riahi, K., Rogner, H.-H. & Strupeit, L. 2012. Energy Primer. In Global Energy Assessment - Toward a Sustainable Future. Cambridge, UK; New York, NY, USA and Laxenburg, Austria: Cambridge University Press and International Institute for Applied Systems Analysis: 99-150. [ Links ]
Harvey, F. 2014. The Energy "TRilemma": How Did We Get Here? The Guardian. [ Links ]
International Diabetes Federation. 2020. Diabetes in Zambia. IDF Africa Members,. https://idf.org/our-network/regions-members/africa/members/30-zambia.html 6 April 2020. [ Links ]
Jemmott, J.B., Jemmott, L.S., O'Leary, A., Ngwane, Z., Icard, L., Bellamy, S., Jones, S., Landis, J.R., Heeren, G.A., Tyler, J.C. & Makiwane, M.B. 2011. Cognitive-behavioural Health-promotion intervention Increases Fruit and VegetableConsumption and Physical Activity Among South African adolescents: A Cluster-Randomised Controlled Trial. Psychology and Health, 26(2): 167-185. [ Links ]
Jung, J. & Huxham, M. 2019. Firewood Usage and Indoor Air Pollution from Traditional Cooking Fires in Gazi Bay, Kenya. Bioscience Horizons: The International Journal of Student Research, 11. https://doi.org/10.1093/biohorizons/hzy014. [ Links ]
Kalene Mission Hospital Online. 2017. Kalene Mission Hospital. https://web.archive.org/web/20171009193242/http:/www.kalenehospital.com/ 6 April 2020. [ Links ]
Kalusa, W.T. 2014. Missionaries, African Patients, and Negotiating Missionary Medicine at Kalene Hospital, Zambia, 1906-1935. Journal of Southern African Studies, 40(2): 283-294. [ Links ]
Kitzinger, J. 1995. Qualitative Research: Introducing focus groups. BMJ, 311(7000): 299 LP - 302. http://www.bmj.com/content/311/7000/299.abstract. [ Links ]
Ledwith, M. & Springett, J. 2010. Participatory Practice: Community-Based Action for Transformative Chang. Bristol: Policy Press. [ Links ]
Lehmann, U., Dieleman, M. & Martineau, T. 2008. Staffing Remote Rural Areas in Middle- and Low-income Countries: A Literature Review of Attraction and Retention. BMC Health Services Research, 8(1): 19. https://doi.org/10.1186/1472-6963-8-19. [ Links ]
Malama, B. 2014. Ikelenge Cries for Factory. Zambia Daily Mail Limited,. http://www.daily-mail.co.zm/ikelenge-cries-for-factory-roads/ 6 April 2020. [ Links ]
Malik, V.S., Popkin, B.M., Bray, G.A., Després, J.-P., Willett, W.C. & Hu, F.B. 2010. Sugar-Sweetened Beverages and Risk of Metabolic Syndrome and Type 2 Diabetes. Diabetes Care, 33(11): 2477-2483. http://care.diabetesjournals.org/content/33/11/2477.abstract. [ Links ]
Max-Neef, M. a., Hopenhayn, M. & Hamrell, S. 1992. Human Scale Development: Conception, Application and Further Reflections, Volume 1. Apex Press. http://www.area-net.org/fileadmin/user_upload/papers/Max-neef_Human_Scale_development.pdf 6 April 2020. [ Links ]
Meegan, M.E., Conroy, R.M., Lengeny, S.O., Renhault, K. & Nyangole, J. 2001. Effect on Neonatal Tetanus Mortality After a Culturally-based Health Promotion Programme. Lancet, 358(9282): 640-641. [ Links ]
Te Morenga, L., Mallard, S. & Mann, J. 2013. Dietary Sugars and Body Weight: Systematic Review and Meta-analyses of Randomised Controlled Trials and Cohort Studies. BMJ: British Medical Journal, 346: e7492.http://www.bmj.com/content/346/bmj.e7492.abstract. [ Links ]
Mukanu, M.M., Zulu, J.M., Mweemba, C. & Mutale, W. 2017. Responding to Non-communicable Diseases in Zambia: a Policy Analysis. Health Research Policy and Systems, 15(1): 34. http://health-policy-systems.biomedcentral.com/articles/10.1186/s12961-017-0195-7 15 January 2020. [ Links ]
Nayak, B.S. & Bhat, V.H. 2016. School Based Multicomponent Intervention for Obese Children in Udupi District, South India - A Randomized Controlled Trial. Journal of Clinical and Diagnositic Research, 10(12): SC24. [ Links ]
Naz, S., Page, A. & Agho, K.E. 2017. Household Air Pollution from Use of Cooking Fuel and Under-five Mortality: The Role of Breastfeeding Status and Kitchen Location in Pakistan. PLOS ONE, 12(3): e0173256. https://doi.org/10.1371/journal.pone.0173256. [ Links ]
North West Zambia Development Trust. 2013. Zengamina Hydro Project. http://www.nwzdt.org/?page_id=22 14 January 2020. [ Links ]
Ojakaa, D., Olango, S. & Jarvis, J. 2014. Factors Affecting Motivation and Retention of Primary Health Care Workers in Three Disparate Regions in Kenya. Human Resourcesfor Health, 12(1): 1-13. [ Links ]
Pesa, I. 2014. Moving Along the Roadside: A Social History of Mwinilunga District, 1870s-1970s. Leiden University. https://openaccess.leidenuniv.nl/handle/1887/28744 14 January 2020. [ Links ]
Popkin, B.M., Adair, L.S. & Ng, S.W. 2012. Global Nutrition Transition and the Pandemic of Obesity in Developing Countries. Nutrition Reviews, 70(1): 3-21. [ Links ]
Roy, J., Tschakert, P., Waisman, H., Halim, S.A., Antwi-Agyei, P., Dasgupta, P., Hayward, B., Kanninen, M., Liverman, D., Okereke, C., Pinho, P.F., Riahi, K. & Suarez Rodriguez, A.G. 2018. Sustainable Development, Poverty Eradication and Reducing Inequalities. In V. Masson-Delmotte, P. Zhai, H.-O. Pörtner, D. Roberts, J. Skea, P. R. Shukla, A. Pirani, W. Moufouma-Okia, C. Péan, R. Pidcock, S. Connors, J. B. R. Matthews, Y. Chen, X. Zhou, M. I. Gomis, E. Lonnoy, T. Maycock, M. Tignor, & T. Waterfield, eds. Global Warming of1.5°C. An IPCC Special Report on the Impacts of Global Warming of 1.5°CAbove Pre-industrial Levels and Related Global Greenhouse Gas Emission Pathways, in the Context of Strengthening the Global Response to the Threat of Climate Change,. Cambridge, U.K.: Cambridge University Pres: 445-538. [ Links ]
Skovdal, M. & Cornish, F. 2015. Qualitative Research for Development. A Guide for Practitioners. Rugby, UK: Practical Action Publishing. [ Links ]
Sustainable Energy for All. 2020. Zambia - SEforALL Africa Hub. https://www.se4all-africa.org/seforall-in-africa/country-data/zambia/ 14 January 2020. [ Links ]
Tausch, A.P. & Menold, N. 2016. Methodological Aspects of Focus Groups in Health Research: Results of Qualitative Interviews With Focus Group Moderators. Global Qualitative Nursing Research, 3: 2333393616630466. [ Links ]
The Borgen Project. 2018. Cooling in Developing Countries. https://borgenproject.org/cooling-in-developing-countries/ 6 April 2020. [ Links ]
United Nations. 2019a. Goal 3: Sustainable Development Knowledge Platform. https://sustainabledevelopment.un.org/sdg3 14 January 2020. [ Links ]
United Nations. 2019b. Goal 7: Sustainable Development Knowledge Platform. https://sustainabledevelopment.un.org/sdg7 14 January 2020. [ Links ]
World Health Organisation. 2015. Global Action Plan for the Prevention and Control of NCDs 2013-2020. World Health Organization. [ Links ]
World Health Organisation. 2018a. Household Air Pollution and Health. https://www.who.int/news-room/fact-sheets/detail/household-air-pollution-and-health 17 January 2020. [ Links ]
World Health Organisation. 2010. Increasing Access to Health Workers in Remote and Rural Areas Through Improved Retention: Global Policy Recommendations. https://apps.who.int/iris/handle/10665/44369. [ Links ]
World Health Organisation. 2019. Reducing Free Sugars Intake in Adults to Reduce the Risk of Noncommunicable Diseases. World Health Organization. https://www.bmj.com/content/346/bmj.e7492?view=long&pmid=23321486 16 January 2020. [ Links ]
World Health Organisation. 2018b. Zambia Non Communicable Disease Profile. https://www.who.int/nmh/countries/zmb_en.pdf 15 January 2020. [ Links ]
Wurie, H.R., Samai, M. & Witter, S. 2016. Retention of Health Workers in Rural Sierra Leone: Findings from Life Histories. Human Resources for Health, 14(1): 1-15. [ Links ]
Zambia Statistics Agency. 2015. Zambian LCMS 2015 Household Survey. Zambia Statistics Agency Online. https://www.zamstats.gov.zm/ 6 April 2020. [ Links ]
* Corresponding author: Tel.: +44 (0)1274383943 email: e.l.v.caperon@leeds.ac.uk


{kind=link}