










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkJournal of the South African Veterinary Association
versión On-line ISSN 2224-9435
versión impresa ISSN 1019-9128
J. S. Afr. Vet. Assoc. vol.95 no.1 Pretoria 2024
http://dx.doi.org/10.36303/JSAVA.586
ORIGINAL RESEARCH
Comparison of exposure of the radius afforded by the craniomedial and craniolateral open surgical approaches in dog cadavers
SK Crowdis; DD Lewis
Department of Small Animal Clinical Sciences, College of Veterinary Medicine, University of Florida, United States of America
ABSTRACT
Management of antebrachial fractures in dogs typically involves open reduction and bone plate stabilisation of the radius performed using either a craniomedial approach (CMA) or craniolateral approach (CLA). The aim of this cadaveric study was to compare radial exposure afforded via the craniomedial and craniolateral approaches, without and with releasing the abductor digiti I longus (ADIL) muscle. The CMA and CLA were performed on alternate paired cadaver forelimbs with the subsequent release (CMA) or elevation (CLA) of the ADIL muscle (n = 12). The percent area of exposure was calculated in defined longitudinal radial segments (LRSs) and hemi-circumferential radial segments (HRSs) using digitally uploaded images. A non-parametric rank sum test was used for statistical analysis (p < 0.05).
While both the CMA and CLA provided sufficient exposure for radial cranial plate placement in the mid-to-distal diaphyseal region (50-80% LRSs), the CMA afforded greater exposure to the distal metaphysis (80-90% LRS). The CLA was advantageous in exposing the proximal diaphysis (20-50% LRSs) and distal epiphysis (90-100% LRS). Exposure of the distal diaphyseal, metaphyseal, and epiphyseal regions (80-100% LRSs) was impeded by the ADIL muscle. A tenotomy of the tendon of insertion of the ADIL muscle increased exposure afforded by the CMA in the distal metaphyseal and epiphyseal regions. The exposure afforded by the CLA in the distal diaphyseal and metaphyseal regions was significantly improved by elevating the origin of the ADIL muscle. The results of this study provide useful clinical information when surgeons are deciding which approach to use for cranial radial plating.
Keywords: canine, radius, plating, approach, fracture
Introduction
Management of antebrachial fractures in dogs typically involves open reduction and stabilisation with a plate applied to the cranial surface of the radius (Ramírez & Macías 2016). Craniomedial and craniolateral approaches to the radius have been described (Piermattei & Johnson 2004) with each approach having advantageous attributes (Ramírez & Macías 2016; De Arburn Parent et al. 2017).
Selecting which surgical approach to use when plating a dog's antebrachial fracture is influenced by the location and configuration of the fracture, available implants, associated soft tissue trauma, and the training and experience of the surgeon (Brinker et al. 1998; Fox 2012). Antebrachial fractures often involve the middle-to-distal two-thirds of the radial diaphysis with a concurrent ulnar fracture (Fox 2012). Adequate exposure of the major fracture segments in this region for open plate application can be limited by the proximity of surrounding myotendinous and neurovascular structures (Larsen et al. 1999). The craniomedial approach (CMA) is reportedly advantageous because less soft tissue dissection is required as the craniomedial surface of the radius is more superficially located in the mid-to- distal radius, thereby mitigating the risk of haemorrhage or injuring the superficial branches of the radial nerve (Piermattei & Johnson 2004). The craniolateral approach (CLA) is advocated because this approach allows simultaneous exposure to the radius and ulna through the same skin incision (Lipowitz et al. 1993; Brinker et al. 1998) and is more advantageous when stabilising very distal radial fractures (Piermattei & Johnson 2004). Exposure of the distal radius can reportedly be improved by releasing the abductor digiti I longus (ADIL) muscle at its origin when performing the CLA or by transecting the tendon of insertion as this structure courses obliquely over the distal radius when performing a CMA (Piermattei & Johnson 2004; Lipowitz et al. 1993).
The objective of this cadaveric study was to quantitively compare the exposure of the radius obtained using either the CMA or CLA to the radius, without and with transection of the tendon of insertion (CMA) or release of the origin (CLA) of the ADIL muscle. We were specifically interested in defining longitudinal and hemi-circumferential segments of the radius that were sufficiently exposed via each approach to allow for cranial plate application. We hypothesised that the CLA would provide greater proximal diaphyseal and distal epiphyseal exposure, and the CMA would offer greater distal diaphyseal and metaphyseal exposure. We also hypothesised that release of the ADIL muscle would improve the exposure of the distal diaphyseal, metaphyseal, and epiphyseal region for both approaches. The results of this study should provide surgeons, particularly less experienced surgeons, with objective information to base decisions regarding which approach might be more advantageous when addressing radial fractures at specific locations.
Materials and methods
This study was performed using dog cadavers obtained from shelters where the dogs were scanned for microchips in an attempt to identify an owner. Dogs were only euthanised and donated if the animal had not been claimed by an owner or was not adopted after a prolonged period of time. Animal Care and Use Committee oversight is not required for use of dog cadavers at our institution. Twelve dog (six females, six males) cadavers of various ages were used in the study weighing approximately 16.0-37.2 (mean 26.3 ±8.0) kg. The limbs did not have gross evidence of prior fractures or deformity. Cadavers with visible or palpable antebrachial musculoskeletal abnormalities were excluded from the study population. The cadavers' forelimbs were disarticulated at the scapulohumeral joint and frozen at -20 °C for later use. Freezing of the disarticulated limbs was carried out with the limbs in slight suspension to imitate the standing position and to prevent pressure deformities or retraction of muscles. The limbs were thawed and similarly prepared 48 hours prior to dissection. The approach used was alternated between forelimbs in individual dogs. Forelimbs were assigned to approach groups using a randomising application (random. org/coin) such that six left forelimbs and six right forelimbs were assigned to the CMA group and the other six left forelimbs and six right forelimbs were assigned to the CLA group (n = 12).
Limb Preparation
The skin was removed from the brachium to the level of the proximal manus. The limbs were positioned with the caudal aspect of the antebrachium dependent. A Kern bone holding forceps was applied to the brachium to maintain the proximal limb segment in a vertical position. A 22-gauge needle was placed in the radiocarpal joint to visualise the distal border of the radius.
Craniomedial Approach (CMA)
The deep antebrachial fascia was incised proximally between the extensor carpi radialis and pronator muscles. The median nerve and brachial artery and vein were identified, and care was taken to protect these structures during dissection. A Freer elevator was used to bluntly elevate the musculature, and a Hohmann retractor was placed to maintain exposure of the radius and provide light retraction. The degree of retraction was assessed by a board-certified surgeon (DDL) so that the exposure obtained was reflective of what would be expected intraoperatively in a clinical case.
Grey (Grease Lightening Sally Hansen Insta-Dri®) nail polish was applied to delineate the region of radius exposed with this surgical approach. The nail polish was allowed to dry for six hours at ambient temperature, before the ADIL muscle's tendon of insertion was transected as this structure passed into the medial sulcus of the radius. Red (ASAP Apple Sally Hansen Insta-Dri®) nail polish was applied to delineate the additional area of the radius exposed following the tendonotomy. The nail polish was allowed to dry for six hours before the radius and ulna were disarticulated at the elbow and antebrachiocarpal joints. The antebrachial musculature was dissected from the radius and ulna until the bones were free of the attached muscles.
Craniolateral Approach (CLA)
The deep antebrachial fascia was incised over the diaphysis of the radius between the extensor carpi radialis muscle and the more laterally located common digital extensor muscle. The common and lateral digital extensor muscles were retracted caudolaterally, and the extensor carpi radialis was retracted craniomedially to expose the lateral diaphysis of the radius. A Freer elevator was used to elevate the musculature, and a Hohmann retractor was placed to maintain exposure of the radius and provide light retraction. The degree of retraction was assessed by a board-certified surgeon (DDL) so that the exposure obtained was reflective of what would be expected intraoperatively in a clinical case. Blue (Jet Setter Sally Hansen Insta-Dri®) nail polish was applied to delineate the region of radius exposed with this surgical approach. The nail polish was allowed to dry for six hours at ambient temperature before the ADIL muscle was elevated from its origin near the interosseous crest of the lateral radius. Purple (Go Garnet Sally Hansen Insta-Dri® nail polish was used to delineate the additional area of exposure of the radius exposed following this. The nail polish was allowed to dry for six hours before the radius and ulna were disarticulated at the elbow and antebrachiocarpal joints. The antebrachial musculature was dissected from the radius and ulna until the bones were free of the attached muscles.
Image Intake and Analysis
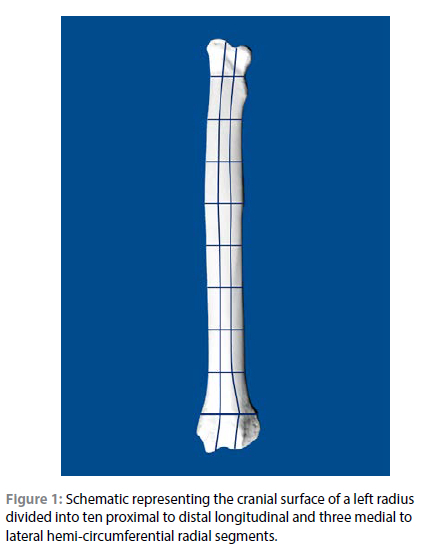
Images of the cranial aspect of the radius were obtained using a cellphone (iPhone 13 ProMax) positioned with a tripod and at a consistent focal length of 20 cm. A marker was placed adjacent to the radius to ensure appropriate digital calibration. The camera was centred and positioned parallel to the mid-radius. The images were digitally uploaded (sketchandcalc.com) for analysis. The digital length of the bone was measured along the frontal plane mechanical axis and the radius was divided into ten proximal-to-distal longitudinal radial segments (LRSs) and transversely into three hemi-circumferential radial segments (HRSs) (Figures 1 and 2).
The total surface area for the defined radial segments was calculated prior to calculating the total surface area painted with nail polish for each defined HRS and LRS. The surface area of radius painted with nail polish in each of the defined radial segments was divided by the total surface area of that defined radial segment to calculate the percent exposed for each of the four approaches. In applicable defined radial segments, the increase in the percent surface area exposure afforded by releasing the ADIL muscle was calculated separately. Mean ± SD percent exposure was calculated for each defined radial segment for both the CMA and CLA without and with release of the ADIL muscle. A nonparametric rank sum test was performed for statistical analysis. A p < 0.05 was used for statistical significance.
Results
The percent exposure of defined LRSs and HRSs afforded via the CMA and CLA without releasing the ADIL muscle is listed in Table I.
The proximal epiphyseal and metaphyseal regions of the radius (0-20% LRSs) were not exposed through either approach. Exposure of the cortical surface of the radius in these regions would have required elevation of the pronator and supinator muscles. Exposure of the proximal diaphyseal region (20-30% LRS) was limited via the CMA, but the CLA afforded greater exposure in the cranial and lateral HRSs. The exposure of the lateral proximal radial diaphysis (30-50% LRSs) was greater with the CLA than with the CMA. There were no differences in exposure afforded by the CMA and CLA in the remainder of the diaphyseal region with both approaches yielding similar exposure of the radius in this region. While the exposure of the lateral, and to a lesser extent the cranial HRS in the distal metaphyseal region (80-90% LRS) was limited via both approaches, the CMA afforded greater exposure to the medial distal radial metaphysis than the CLA. Exposure of the medial distal radial epiphysis (90-100% LRS) was limited via both approaches, but greater exposure of the cranial and lateral HRSs in the distal radial epiphysis was obtained by using the CLA compared to the CMA.
The percent exposure of defined LRSs and HRSs via the CMA and CLA following release of the tendon of insertion or elevation of the origin of the ADIL muscle, respectively, is listed in Table II, and the increase in percent exposure of defined LRSs and HRSs via the respective release of the tendon of insertion (CMA) or elevation of the origin (CLA) of the ADIL muscle is summarised in Table III.
Exposure was not increased from the proximal epiphysis through diaphysis (0-50% LRSs) with transecting the ADIL muscle. Release or elevation of the ADIL muscle primarily afforded an increase in exposure in the distal diaphyseal, metaphyseal, and epiphyseal regions. Elevation of the origin of the ADIL muscle afforded an increase in exposure most notably within the distal diaphysis (70-80% LRS) and lateral metaphysis and epiphysis (80-100% LRSs). The greatest increase in exposure following release of the tendon of insertion of the ADIL muscle was seen within the medial and cranial distal metaphysis and epiphysis (80-100% LRSs). Greater exposure was obtained within the medial distal metaphysis and epiphysis (80-100% LRSs) with the combined CMA and release of the tendon of insertion of the ADIL muscle. Exposure of the lateral HRS from the proximal diaphysis to the distal epiphysis (20-100% LRSs) was more greatly afforded by the CLA and elevation of the origin of the ADIL muscle.
Discussion
Our results provide objective guidance for surgeons when selecting an approach for cranial radial plate application (Figure 3). We partially accept our hypothesis as the CLA provided greater exposure to the proximal diaphysis and distal epiphysis. Although the CMA did provide greater metaphyseal exposure in the medial HRS, there was no statistical difference seen between the two approaches in the distal diaphysis.
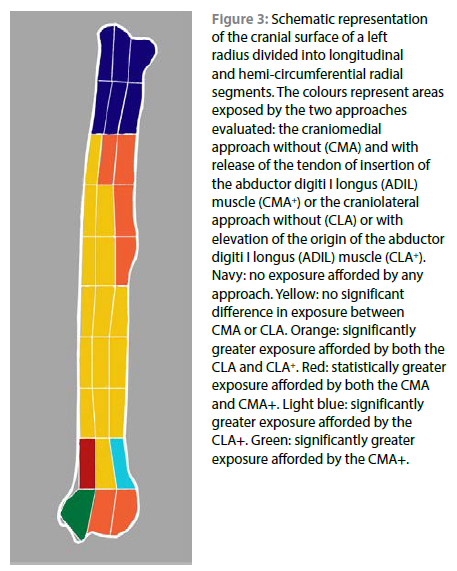
A similar study has been performed using human cadaver specimens to objectively delineate surface area exposure of the radius afforded by different open surgical approaches (Cross et al. 2011). In our study, the CLA affords greater exposure to the proximal lateral diaphysis (20-50% LRSs) and distal lateral and cranial epiphysis (90-100% LRS). There was no significant difference in exposure afforded the CMA and CLA identified in the mid-to-distal diaphyseal region (50-80% LRSs). Most antebrachial fractures in dogs involve the distal radial diaphysis (Ramírez & Macías 2016). Based on our results, both approaches provide sufficient exposure for cranial plate placement in this region and either approach can be used based on the surgeon's preference and case requirements. Plate placement in the distal radial metaphyseal region (80-90% LRS) can be more readily accomplished using the CMA particularly in the medial HRS, without release of the tendon of insertion of the ADIL muscle. Lakshmi, et al. (2007) has advocated using the CMA when performing open plating of distal metaphyseal radial fractures.
Distal exposure (80-100% LRSs) can be effectively improved using either approach by transecting the tendon of insertion (CMA) or by releasing the origin (CLA) of the ADIL muscle. Sardinas and Montavon (1997) describe improving exposure by manipulating the ADIL muscle when performing medial bone plate placement when stabilising distal radius and ulna fractures, but retraction can also inhibit obtaining and maintaining reduction and alignment. Our findings suggest that releasing the ADIL muscle improves exposure of the distal radius, for both the craniomedial or craniolateral approaches, and should be considered when attempting distal cranial radial plate placement.
This study had several limitations. Although there was variation in size and musculature of individual cadavers, an attempt was made to acquire cadavers of relatively uniform body size, conformation, and muscular development. Even though this study used advanced digital imaging software, the area of exposure afforded by the approaches may be slightly underestimated as we utilised two-dimensional image analysis to delineate three-dimensional osseous morphology. In addition, the exposure obtained in cadaver limbs, which had the skin excised could have been different than the exposure that would be obtained in live dogs undergoing open radial fracture stabilisation. We were, however, cognisant to this issue and attempted to ensure the degree of muscle retraction employed during the dissection reflected what would be done during a standard surgical procedure. The force of retraction, unfortunately, was not measured.
Conclusion
The proximal lateral diaphysis and distal lateral and cranial epiphysis are more easily accessed with the CLA. The CMA provides greater exposure of the distal medial metaphyseal region. While either the craniomedial and craniolateral approaches afford sufficient exposure for cranial plate application in the mid-diaphyseal region, plate placement in the distal diaphyseal, metaphyseal, and epiphyseal regions is impeded by the ADIL muscle. The tendon of insertion of the ADIL muscle limits exposure of the distal metaphyseal and epiphyseal region via CMA, but tenotomy significantly improves exposure. Similarly, exposure of the distal diaphyseal and metaphyseal regions can be significantly improved by elevating the origin of the ADIL muscle. Our results suggest that a quantitative clinical trial evaluating exposure afforded by each of these approaches during open reduction and cranial plating of radial fractures is warranted.
Conflict of interest
The authors declare they have no conflicts of interest that are directly or indirectly related to the research.
Funding source
This work was supported by the Dr Jeff and Jo Godwin Advanced Small Animal Surgical Training and Canine Gait Laboratory.
Ethical approval
The author/s declare that this submission is in accordance with the principles laid down by the Responsible Research Publication Position Statements as developed at the 2nd World Conference on Research Integrity in Singapore, 2010.
This article does not contain any studies with human or animal subjects.
ORCID
SK Crowdis https://orcid.org/0009-0004-5298-0685
DD Lewis https://orcid.org/0000-0001-9675-6408
References
Brinker, W.O., Olmstead, M.L., Sumner-Smith, G., et. al., 1998, Manual of Internal Fixation in Small Animals, 2nd ed, Berlin, Springer, (2), 146. https://doi.org/10.1007/978-3-642-60288-7. [ Links ]
Cross, J.D., White, J.A., Johnson, AE., et al., 2011, Comparison of dorsal and volar approaches to the proximal radius, Orthopedics 34(2):93. https://doi.org/10.3928/01477447-20101221-14. [ Links ]
De Arburn Parent, R., Benamou, J., Gatineau, M., et al., 2017, Open reduction and cranial bone plate fixation of fractures involving the distal aspect of the radius and ulna in miniature- and toy-breed dogs: 102 cases (2008-2015), J Am Vet Med Assoc 250(12), 1419-1426. https://doi.org/10.2460/javma.250.12.1419. [ Links ]
Fox D.J., 2012, Radius and ulna, In: Tobias KM, Johnston SA, eds., Veterinary Surgery Small Animal, St. Louis WB, Saunders, 761-784. [ Links ]
Lakshmi, N.D., Ganesh, T.N., Ayyappan, S., et al., 2007, Management of a distal metaphyseal radial fracture in a dog with a mini-T-plate, Vet Rec 161(23), 791-792. [ Links ]
Larsen, L.J., Roush, J.K., McLaughlin, R.M., 1999, Bone plate fixation of distal radius and ulna fractures in small- and miniature-breed dogs, J Am Anim Hosp Assoc 35(3), 243-250. https://doi.org/10.5326/15473317-35-3-243. [ Links ]
Lipowitz, A.J., Caywood, D.D., Newton, C.D., 1993, Small Animal Orthopedics Illustrated: Surgical Approaches and Procedures. 1st ed. St. Louis: Mosby Inc, 140. [ Links ]
Piermattei, D.L., Johnson, K.A., 2004, The Forelimb. In: An Atlas of Surgical Approaches to the Bones and Joints of the Dog and Cat, 4th ed, Philadelphia: WB Saunders, 246-254. https://doi.org/10.1016/B978-0-7216-8707-0.50008-7. [ Links ]
Ramírez, J.M., Macías, C., 2016, Conventional bone plate fixation of distal radius and ulna fractures in toy breed dogs, Aust Vet J 94(3), 76-80. https://doi.org/10.1111/avj.12408. [ Links ]
Sardinas, J.C., Montavon, P.M., 1997, Use of a medial bone plate for repair of radius and ulna fractures in dogs and cats: a report of 22 cases, Vet Surg 26(2), 108-113. https://doi.org/10.1111/j.1532-950X.1997.tb01472.x. [ Links ]
 Correspondence:
Correspondence:
email: kattcrowdis@ufl.edu


{kind=link}
{kind=link}
{kind=link}
{kind=link}