










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkJournal of the South African Veterinary Association
versão On-line ISSN 2224-9435
versão impressa ISSN 1019-9128
J. S. Afr. Vet. Assoc. vol.94 no.1 Pretoria 2023
http://dx.doi.org/10.36303/JSAVA.540
ORIGINAL ARTICLE
Application of the Alivecor KardiaMobile smartphone modulated ECG device for use in horses
G PikethI; A WilliamsII; EC SchliewertI
IDepartment of Companion Animal Clinical Studies, Faculty of Veterinary Science, University of Pretoria, South Africa
IIHead of Equine and Data, Research and Ai Executive Manager, Vet-Ai Information, United Kingdom
ABSTRACT
Electrocardiography is the method used to monitor the electrical impulses in the heart. These diagnostics are increasingly making use of smartphone-based technologies.
The objective of this research was to determine whether the Alivecor KardiaMobile (ECGAKM) smartphone-modulated electrocardiographic device, a novel ECG device, can be used to obtain reliable electrocardiogram (ECG) readings in horses.
The device was initially tested in 36 Nooitgedacht pony mares to determine the best site of application, method of skin preparation, and ECGAKM device orientation for reliable ECG tracings. Once the most reliable site for ECG acquisition was determined, the device was then applied, in this manner, to 31 Nooitgedacht pony mares and compared with a standard telemetric ECG system (ECGTV).
The ECGAKM device was best applied in the fourth intercostal space on the left hemithorax in a vertical orientation and with the skin dampened with 70% ethanol. Mean values determined for RR and QT intervals between the ECGAKM and ECGTV were not significantly different, however, mean values for the duration of the QRS complexes were significantly different for the two devices. There is acceptable agreement between the ECGTV and ECGAKM devices with regards to the measurement of the PQ; RR and QT intervals but not the QRS duration. The automatically calculated heart rate is not an accurate measure of true heart rate.
The Alivecor KardiaMobile (ECGAKM) device can be considered as a simplified screening ECG device in situations where the more standardised system is either unavailable or impractical, but has some limitations.
Keywords: smartphone, electrocardiography, horse, Alivecor KardiaMobile, intercostal, tracing, waveform, Bland-Altman
Introduction
Electrocardiography is the method used to monitor the genesis, propagation, and conduction of electrical impulses in the heart. This centers on the measurement of an electrical potential difference created by the electrical activity in cardiac musculature. The changes in this electrical activity are recorded and displayed as a "real time" tracing with the depolarisation and repolarisation of the cardiac tissues represented as deflections of the tracing around a baseline (Mitchell 2019; Van Loon & Patteson 2010).
In the digital era, smartphones are increasingly used in medical diagnostics and many of the more recently developed electrocardiographic devices are modulated by smartphone operating systems.
The practicality and the inexpensive nature of these smartphone-based ECG devices lend themselves toward their use in horses, where a significant number of clinical evaluations are conducted in an ambulatory setting (Kraus et al. 2019). The smartphone modulated Alivecor KardiaMobile (Alivecor KardiaMobile Model AC-009, Alivecor Inc., USA) device provides tracings with accurate baseline conduction intervals with a high degree of sensitivity (72.4-94.4%) and specificity (> 94%) in the diagnosis of atrial arrhythmias in human patients (Haberman et al. 2015). Other studies also indicated favourable results for the use of similar, veterinary-specific devices in horses.
Although an AliveCor smartphone-based ECG device has been compared to a standard base-apex ECG in horses in several studies (Alberti et al. 2020; Corradini et al. 2020; Kraus et al. 2019; Vezzosi et al. 2018; Welch-Huston et al. 2020), all of these studies made use of the AliveCor Veterinary Heart Monitor (Alivecor Inc., USA) (ECGvet).
This study aimed to determine whether the Alivecor KardiaMobile (Alivecor Inc., USA) (ECGAKM) smartphone-based ECG device could be successfully applied in horses by determining the best location, orientation, and conditions for ECGAKM device application in the standing horse at rest. Additionally, the study aimed to compare the ECGAKM device recordings to recordings made with a telemetric ECG system considered the gold standard (Televet 100 [Kruuse Televet 100, Rosch and Associates, Frankfurt am Main, Germany]). Unlike the AliveCor Veterinary Heart Monitor, the device used in this study is marketed for use in humans. Due to greater demand, human-orientated diagnostic devices receive wider marketing and distribution, often making them more available than their veterinary related counterparts.
Methods
The study had a cross-sectional study design with specific emphasis on method agreement analysis. The research was conducted in two separate phases with electrocardiographic tracings collected in two separate time periods, namely 11-22 November 2018 and 20-24 May 2019, corresponding with the traditional summer and autumn seasons in the southern hemisphere.
Study population
Clinically healthy, adult, non-pregnant Nooitgedacht pony mares from the Onderstepoort Teaching Animal Unit were included in the study. Mares were considered clinically healthy based on history and clinical examination findings prior to the data collection. Horses with a known history of cardiovascular disease or abnormalities on their clinical examination prior to ECG acquisition were excluded from the study population.
Part 1
Thirty-six pony mares with an age range of 2-25 years and mean body condition of 3/5 (range 2-4/5) were included. Hair coats were generally short and fine with often very sparse coverage in and around the axillary region. Tests were performed in the late spring.
Part 2
Thirty-one pony mares with an age range of 2-25 years and a mean body condition score of 3.5/5 (range 3-4/5) were included. Hair coats were generally longer and coarser than previously because testing was performed in late autumn.
Smartphone ECG acquisition
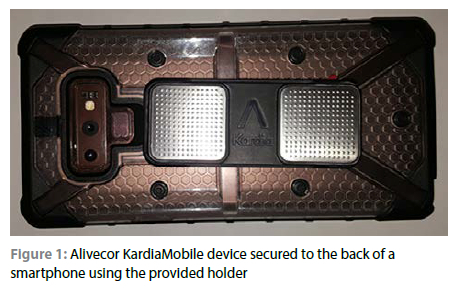
The ECGAKM device was attached to an Android-based smartphone (Samsung Galaxy Note 9, Samsung, South Korea) using the device holder and double-sided tape with the side containing the battery port orientated to the top of the smartphone (Figure 1). The entire phone with attached device was then applied to the study subjects. Once sufficient contact between the patient's skin and the electrodes is achieved, the device synchronises with the Kardia application to enable tracing acquisition. This is achieved via communication with the smartphone's microphone using ultrasound waves, which are then converted into an ECG tracing. Tracings were obtained over a period of 30 seconds with an automatic mains filter applied. Tracings were recorded at a paper speed of 25 mm/s and amplitude of 10 mm/mV.
Standard ECG acquisition
For the second part of the study, the Kruuse Televet 100 Veterinary telemetric ECG (ECGTV) system was used as a gold standard. This device was applied in a modified base apex configuration. Electrodes were attached to the skin using ECG pads held in place using a surcingle. ECG tracings were recorded for a period of 30 seconds at a paper speed of 25 mm/s and amplitude of 10 mm/mV, identical with the settings used in the smartphone device. During acquisition, a 60 hz filter was applied with only a single lead analysed.
Sampling procedure
Part 1
Three body contact locations were used for data collection:
1. The left fourth intercostal space with the lowest end of the ECGAKM device 3-5 cm above the olecranon.
2. The right 4th intercostal space with the lowest end of the ECGAKM device 3-5 cm above the olecranon.
3. The centre of the right triceps muscle mass.
These locations were selected as representative points to determine the best location for tracing acquisition. The locations over the left and right thorax were determined to be the closest locations to the heart tissue with the location over the triceps muscle mass included to assess the influence of increased distance from the heart on the tracing acquisition.
The ECGAKM was applied in three orientations at each site:
1. Vertical orientation with the device perpendicular to the ground.
2. The device horizontal to the ground (rotated clockwise 90 degrees from position 1)
3. At an angle of 45 degrees to the ground (i.e. diagonally across the chest) with the side of the device with the battery compartment orientated caudodorsally.
The device was tested for each of these orientations at the three predetermined sites with each of the following different skin preparations:
1. Without any skin preparation. The hair over the site was left intact and only gross contaminants such as grass or mud were removed.
2. A solution of 70% ethanol was applied to the hair and skin at the recording site. Alcohol was applied using a spray bottle and nozzle with the excess being wiped away using a gloved hand.
3. The site hair was clipped using a portable electric hair clipper and the device applied to dry skin.
The device was applied to the skin using sustained, firm digital pressure from a single operator. The pressure used was sufficient to allow adequate contact of the electrodes with the skin and to prevent slippage of the device.
Part 2
Findings from phase one revealed that application of the ECGAKM device in the left fourth intercostal space, in a vertical orientation and with the skin moistened with 70% alcohol yielded the most repeatable yet complete ECG tracings. As such, this was the method applied for Phase 2 of the study.
Due to the season, the animal's hair coat was comparably longer and thicker. Therefore, the areas of application of the ECGAKM device, as well as areas of electrode attachment for the leads of the ECG™ were clipped and moistened with alcohol. The leads for the ECGTV device were applied in a modified base-apex configuration: The green (left leg) electrode was applied to the sternum, the black (neutral) electrode applied ventral to the withers and spinal column on the left and the red (right arm) electrode applied 10 cm distal to the black lead. The yellow (left arm) electrode was placed at a site corresponding to that of the red lead on the right thorax (Televet 2018). Electrodes were attached to the skin using ECG pads held in place using a surcingle. Once a good quality tracing was obtained with the ECGTV device, a simultaneous ECGAKM tracing was obtained over a period of 30 seconds.
ECG analysis
Part 1
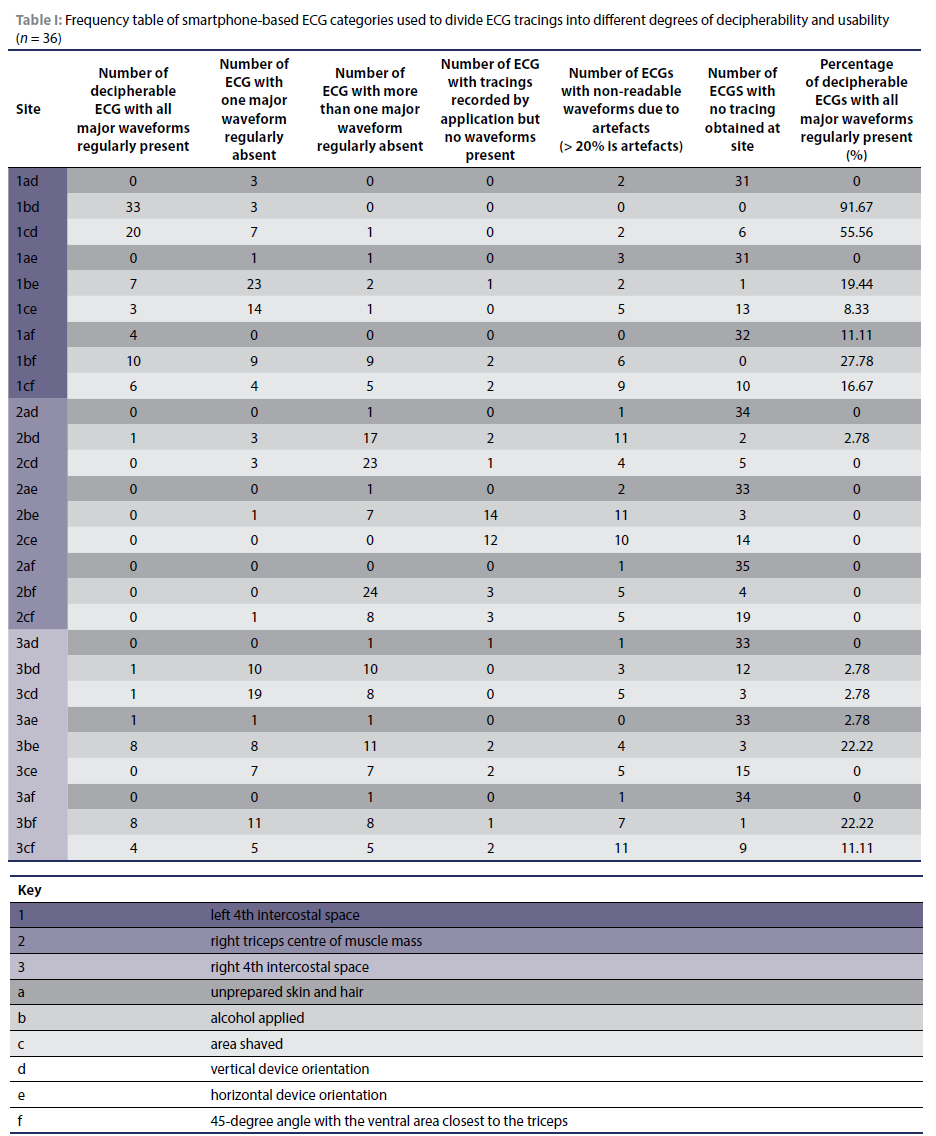
The ECGAKM device was applied at each of the sites mentioned in the experimental methods. The heart rate was obtained and recorded immediately after completion of recordings at each site. All recordings were analysed by the same investigator. For a trace to be considered as diagnostic, baseline artefacts had to be absent for at least 80% of each tracing (Vezzosi et al. 2018). Major waveforms were identified as a P wave, QRS complex (or variation thereof such as rS complex where no Q wave was identified) as well as a T wave. A non-readable tracing was defined as one that had more than 20% of the total tracing obscured by artefacts or where the tracing had one or more waveforms regularly absent but was not consistent with any arrhythmia.
Part 2
Values were recorded from the following dependent variables:
1. PQ interval
2. RR interval
3. QT interval
4. QRS duration
5. Cardiovascular rhythm/rhythmogenesis
The average for each variable was calculated for each tracing including all available complexes. The average value determined for each variable over the entire tracing was then compared between the ECGAKM and ECGTV devices. As such, direct correlation and comparison of individual intervals or complexes between the two devices was not performed.
Data analysis
Data was examined and evaluated using two commercially available software programs namely Microsoft Excel (Microsoft Excel 2013, Microsoft Corporation, USA) and IBM SPSS statistics (IBM SPSS Statistics 2009, IBM, USA) software. Significance was set to 5%.
Part 1
Data was summarised in the form of a frequency table. Heart rate determined by the Kardia app was compared to heart rate determined via auscultation using a Mann-Whitney test and analysed for agreement using graphical representation in the form of a Bland-Altman plot.
Part 2
Data was either summarised in the form of mean (grouped) coupled with standard deviation (if normal distribution) or median and interquartile range (Table I). Agreement between ECGTV and ECGAKM was tested with independent t-test or MannWhitney U test. The level of agreement between quantitative data pairings was determined using a Bland-Altman plot and the bias as well as limits of agreement for each data set were determined (Giavarina 2015).
Results
Part 1
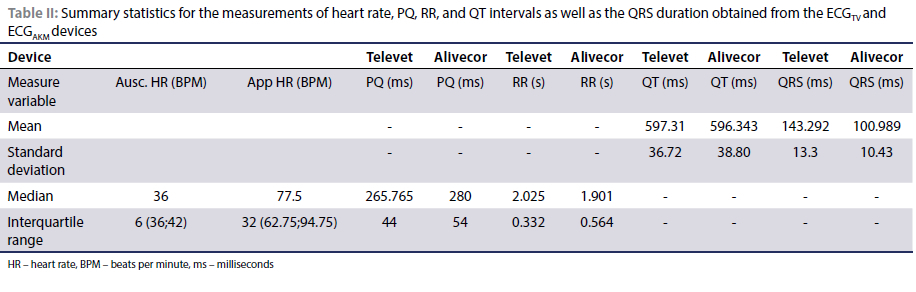
A total of 972 ECG recordings were obtained in Part 1 of the study. Only 11% (107 recordings) of the total recordings were deemed decipherable and of diagnostic value. A total of 91.7% (33/36) of the tracings recorded from the left 4th intercostal space with the device in a vertical orientation and the skin moistened with 70% alcohol were interpretable with all waveforms regularly present. This was the greatest percentage of any of the application methods. Results for the remaining locations, orientations and application methods of the smartphone device can be found in Table I. Heart rate determined using the Kardia app conformed to a normal distribution while the data set for the auscultated heart rate did not. Therefore, the summary statistics are presented as the median and interquartile range in Table II.
Statistical values determined using the Mann-Whitney U test as well as Bland-Altman analysis for comparison of the heart rates determined using the Kardia app and auscultation can be found in Table II. The relationship of the data points in a Bland-Altman plot also indicated that the Kardia app tends to overestimate the actual heart rate value by increasing amounts as the actual heart rates increased.
The Mann-Whitney U test was used to compare the heart rates obtained using the ECGAKM application and on auscultation (the auscultated heart rate data set was not normally distributed). This yielded a U value of 43 and a two-tail significance of 0. Bland-Altman analysis of the heart rate data sets revealed a bias of -39.75 and upper and lower level of agreement of 5.23 and -84.73 respectively. The relationship of the data points in the Bland-Altman plot also indicated that, especially at increased heart rates, the ECGAKM application tends to overestimate the actual value by an increasing amount.
Part 2
Mean QT interval values as well as the mean QRS duration values were determined to follow normal distribution while mean RR and PQ interval values were determined to be non-normally distributed. Table II summarises the data sets accordingly:
Arrhythmias were noted in the same three out of 31 horses (9.67%) in both device tracings when analysed manually. These were consistent with sinoatrial blockades in both the ECGAKM and ECGjv tracings. The Kardia app identified these arrhythmic tracings as unreadable in all three occurrences.
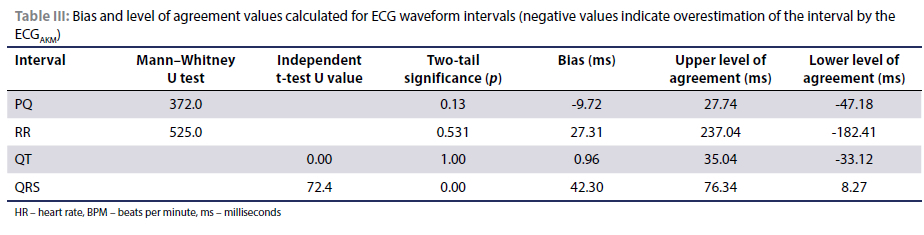
Mean values determined for QT intervals were not significantly different when the two devices were compared. The mean values for the QRS duration were significantly different between the two devices (Table III).
The independent-samples Mann-Whitney U test indicated that the distribution of values of mean PQ and RR interval was the same over the ECGAKM and ECGTV categories. Bland-Altman analysis indicated that ECGAKM on average overestimates the PQ interval by 9.72 milliseconds, underestimates the RR interval by 27.31 milliseconds and underestimated the QT value by a meagre 0.96 milliseconds. Bland-Altman analysis also revealed that the ECGAKM device tends to underestimate the QRS duration by 42.30 milliseconds. The values determined for bias and the levels of agreement based on the Bland-Altman analysis can be found in Table III.
Discussion
Alivecor KardiaMobile device application
Previous studies have evaluated and concluded that the use of a veterinary-specific smartphone-based ECG device (ECGVET) may be applicable in horses (Alberti et al. 2020; Corradini et al. 2020; Kraus et al. 2019; Vezzosi et al. 2018; Welch-Huston et al. 2020). The present study specifically evaluates the ECGAKM device, a device designed and manufactured for human use, in horses. The greater demand for and monetary backing applied to the human medical field means devices like the ECGAKM have several advantages over veterinary-specific devices. These include the fact that they are more commonly available, more regularly refined and updated and cheaper than devices specifically designed for veterinary application. Therefore, supporting the idea of an inexpensive and accessible device for use by the ambulatory veterinarian, one would be amiss if a device designed for humans was not examined.
The ECGAKM device and its associated smartphone application, the Kardia app, are simple to navigate and user friendly. They do not require in-depth technical or medical skills to apply, but further evaluation in equids is required before definitive conclusions can be cemented. The orientation of the device relative to the smartphone affects the polarity of complexes on the ECG recording. The polarity of the deflections can however be adjusted using a setting on the Kardia app.
To our knowledge, this is the first study to not only assess the ECGAKM device in horses but also to examine multiple different methods of device application. In this study, the ECGAKM device is compared to a modified base-apex configuration similar to that used in the study by Welch-Huston et al. (2020). Electrodes in the ECGAKM device are arranged in a linear pattern, similar to the linear arrangement of the modified base-apex lead system to fit underneath a surcingle. This modified base-apex configuration also enhances each of the three leads ability to emphasise different portions of the cardiac cycle (Mitchell 2019). Comparing the two devices in these orientations hypothetically would allow for the best chance of obtaining comparable tracings. The ECGAKM tracings were compared for similarity to the ECGTV device and were not expected to be an exact replica. Corradini et al. (2020) evaluated the Alivecor Veterinary Heart Monitor on both the left and right thorax and concluded that the positioning on the right thorax resulted in improvement in the identification and interpretation of the presence of P wave deflections. In that study, they suggest that the user consider obtaining ECG recordings from both sides of the thorax to improve ECG assessment. This should be further evaluated using the ECGAKM device to determine if it is a relevant approach for the use of this device.
In this study, the most appropriate site of application for the device was confirmed to be the fourth intercostal space on the left thorax. This is not an unexpected finding as there is a short distance from the cardiac musculature to the skin surface with a reduced amount of intervening tissue in this location. Skin contact is another important aspect in the acquisition of a good quality ECG tracing. In this case it is thought that application of 70% alcohol yielded the better tracings than dry, unclipped skin as it served to help flatten the coat thereby reducing the intervening air between the electrode and skin. Application of the device in a vertical orientation yielded the most diagnostically relevant and repeatable ECG tracings. This is thought to be due to the fact that in the vertical orientation, the rigid device achieves more consistent contact when applied in only one intercostal space, as there is no rib contour around which the device has to be conformed.
Considering these results, the suggested method of application of the ECGAKM device is as follows:
1. Apply the device in the left fourth intercostal space.
2. Apply the device in a vertical orientation (Figure 2).
3. Moisten the skin of coat with the addition of alcohol to improve the contact of the electrodes.

Alivecor KardiaMobile usability in horses
Due to the limited number of abnormal rhythms present in the study, the comparative process relied on examination of the individual intervals to determine an objective indication of the similarity between tracings recorded by each device. It must be considered that both the duration, amplitude and interval measurements in the equine ECG are at present less diagnostically relevant than in other species due to differences in the pathway of ventricular depolarisation (Hewetson 2013).
Heart rate determination
There was a significant difference between the heart rate obtained by cardiac auscultation compared to the heart rate measured by the Kardia app. The Kardia app tends to overestimate the heart rate by 39.75 beats per minute. This is likely due to the application's tendency to count larger T waves as QRS complexes. This is similar to the conclusions made in several studies examining this phenomenon using the ECGVET (Alberti et al. 2020; Corradini et al. 2020; Vezzosi et al. 2018). As such, the heart rate determined automatically via the smartphone device should not be relied upon to provide accurate heart rate data.
Identification of arrhythmias
Corradini et al. (2020) concluded that the ECGVET had an inherent value as a stall-side evaluation tool for some of the common equine cardiac arrhythmias. Kraus et al. (2019) identified that the ECGVET was able to confer the correct heart rhythm diagnosis in 97% of instances.
In the present study, an arrhythmia was only observed in three (9.6%) horses. The arrhythmia was identified in all three horses on both the ECGAKM and ECGTV tracings and classified as a sinoatrial blockade. Further investigation into the ECGAKM device's ability to identify common arrhythmias in the horse would be required before a definitive conclusion can be reached.
PQ interval
The PQ interval conformed to the same distribution in both devices. In horses, AV blockade is common and can, in certain instances, be considered as physiological (Reed et al. 2017). For this reason, the PQ interval shows a large degree of variation both between different individuals as well as between different complexes in the same ECG (Reed et al. 2017). Previous research has shown that the PQ interval is dependent on which lead is used for its determination (Paslawska et al. 2012) and that the difference between the longest and shortest PQ interval in resting healthy Anglo-Arabian horses can be 60 ± 50 milliseconds (Paslawska et al. 2012). Taking this and clinical experience into consideration, there is good agreement between the two methods tested when considering the PQ interval and its associated variability. A similar observation was made by Vezzosi et al. (2018) and Alberti et al. (2020) for the use of the ECGVET device.
RR interval
The RR interval is extremely important when analysing ECGs for signs of abnormal rhythmicity. As such, it is one of the most important aspects of the comparison between the two devices in this study. Although the mean values for RR interval were determined to not be significantly different for these two devices, further analysis revealed a total variability of 419.45 milliseconds for the RR interval as determined by the ECGAKM. When performing ECG analysis, Mitchell (2019) used a beat-to-beat RR interval variation of 20% as a threshold cut-off for the resting individual. Considering this, the variation is considered clinically acceptable for horses. As such, the ECGAKM displayed good agreement with the ECGTV device with regards to RR interval determination.
QT interval
The QT interval was also examined for agreement between the two devices. Mean QT values were not significantly different between the two devices. Bland-Altman analysis corroborated this and the variation of the QT interval estimation by the ECGAKM seems to be acceptable enough for the device to be used for a screening purpose. This mirrors the conclusions made by Vezzosi et al. (2018) for the QT measurements made using the ECGVET.
QRS complex
The mean values for QRS duration were significantly different between the two devices. Due to the small dipole created by the ECGAKM device, the QRS complex often appears to be a simplified version of that seen in the ECGTV tracings. This is bound to influence the duration of the complex recorded by the ECGAKM device when compared to the ECGTV recording system. Our findings revealed that the ECGAKM device tends to underestimate the QRS duration by 42.30 milliseconds which is the greatest bias seen over any of the waveforms recorded. As such it can be expected that the ECGAKM device is unlikely to yield the same QRS duration as the ECGTV device at any point, resulting in poor agreement between the two devices. This, however, is not expected to significantly influence the assessment of basic arrhythmias in the horse.
Limiting factors for use of the Alivecor Kardia Mobile device
The study did identify some limiting factors in the use of the device in horses. The battery compartment of the ECGAKM is not waterproof and is prone to alcohol infiltration if large volumes are used to moisten the hair coat which is usually required to improve electrode contact. This is a hindrance when using the device in horses as it can result in poor signal acquisition when the device is applied.
Motion artefacts were a common occurrence in this study. Motion artefacts corresponded to obvious movement of the horses' body. Movements included foot stamping due to flies, panniculus (also often associated with irritation by flies) as well as movement associated with the breathing motion. This may have implications for the usability of the device in warmer climates and in post-exercise or diseased horses where an increased respiratory rate and/or effort may occur. Climatic conditions favouring large insect populations such as flies can notably hinder the successful use of the ECGAKM device. This is particularly relevant for the ambulatory setting, where fly control is more difficult than in the hospital environment.
Additionally, the ECGAKM has a very small dipole with regards to the layout of the electrodes. When applied in human medicine, the ECG is recorded with a finger from each hand placed on one of the electrodes. The electrical potential is then measured across the heart making use of the arms as extensions of the lead system. This achieves some mitigation of the concerns that arise due to the small dipole. When applied in the horse, however, the ECG is recorded on the thoracic wall with a small distance between the areas of electrode contact. This study supports the findings reported by Kraus et al. (2019) in dogs as well as Alberti et al. (2020) in horses, where the small dipole leads to a reduction in the amplitude of smaller waveforms such as the P wave.
Study limitations
The present study has several limitations. The evaluation of the best application method of the ECGAKM device is a simplified experimental design that only serves to provide general guidelines regarding the approach of correct application of the ECGAKM device. The three orientational approaches used in this study are a gross underestimation of the total number of ways in which to orientate the device on the horse's thorax. Additional studies may identify a superior orientation. Several important aspects of the functionality of the device were also not evaluated.
For the purpose of this study, the device was attached directly to the underside of the smartphone, so the range between smartphone and device, at which diagnostic recordings can be obtained, was not assessed. It should also be mentioned that although the device overestimated the heart rate due to incorrectly identifying T waves as QRS complexes, no further evaluation was conducted to determine if different orientations of the ECGAKM device had any influence on this.
The current study does not evaluate the comparability between the ECGAKM and the ECGVET devices with regards to their use in the identification of pathological arrhythmias. Before a definitive statement can be made on the use of the ECGAKM device, further evaluation regarding its ability to identify and record arrhythmic events in the horse is required. Further investigation into factors that may hinder appropriate tracing acquisition is also needed. These include factors such as those affecting electrode contact and ECG quality.
Another limitation is the relatively uniform study population. A more diverse study population could evaluate the applicability of the device in different breeds, hair coat, and body type.
Tracing analysis was performed by a single individual with only tracings deemed to display arrhythmias checked by a second person. As such, it was not possible to determine an inter-observer agreement for this study and thereby the reliability of the data. It may be more beneficial to have several individuals with different levels of training to analyse and evaluate the ECG tracings.
Conclusion
The ECGAKM can record decipherable ECG tracings in horses on a repeatable basis. The device is easy to use and requires limited training to obtain diagnostic ECG recordings. The ECGAKM device does not yield identical tracings to the ECGTV, but the tracings recorded do appear to show sufficient agreement with the ECGTV device to be considered as a simplified screening device in situations where the more standardised system is either unavailable or impractical. As concluded by Kraus et al. (2019) and Vezzosi et al. (2018) with regards to the ECGVET, the ECGAKM is not currently considered to be a suitable substitute for the more standard 6-lead ECG systems and should not be considered for in-depth cardiovascular analysis. Further studies evaluating the ECGAKM device's ability to identify and record arrhythmic events in the horse are warranted.
Conflict of interest
The authors declare no conflict of interest.
Funding source
Funding for this research was partially obtained from the Agricultural Sector Education Training Authority (AgriSeta) in conjunction with Borbely Trading CC (Technopet).
Ethical approval
The study was approved by the Faculty of Veterinary Science Research Committee and the University of Pretoria Institutional Animal Ethics Committee (V087-18).
ORCID
G Piketh https://orcid.org/0000-0002-1556-3418
A Williams https://orcid.org/0000-0003-4351-1946
EC Schliewert https://orcid.org/0000-0003-3763-8203
References
Alberti, E., Stucchi, L., Pesce, V., et al., 2020, Evaluation of a smartphone-based electrocardiogram device accuracy in field and in hospital conditions in horses, Vet Rec Open 7(1), e000441. https://doi.org/10.1136/vetreco-2020-000441. [ Links ]
Corradini, I., Fernández-Ruiz, A., Barba, M., et al., 2020, Stall-side screening potential of a smartphone electrocardiogram recorded over both sides of the thorax in horses, J Vet Intern Med, 34(5), 2101-2108. https://doi.org/10.1111/jvim.15795. [ Links ]
Giavarina, D., 2015, Understanding Bland-Altman analysis, Biochem Med 25, 141-151. https://doi.org/10.11613/BM.2015.015. [ Links ]
Haberman, Z.C., Jahn, R.T., Bose, R., et al. 2015, Wireless smartphone ECG enables large-scale screening in diverse populations, J Cardiovasc Electrophysiol 26(5), 520-526. https://doi.org/10.1111/jce.12634. [ Links ]
Hewetson, M., 2013, Introduction to electrocardiography in the horse and recognition of common abnormalities, Proceedings of the 13th International Congress of the World Equine Veterinary Association, Budapest, Hungary. [ Links ]
Kraus, M.S., Rishniw, M., Divers, T.J., et al., 2019, Utility and accuracy of a smartphone-based electrocardiogram device as compared to a standard base-apex electrocardiogram in the horse, Res Vet Sci 125, 141-147. https://doi.org/10.1016/j.rvsc.2019.05.018. [ Links ]
Mitchell, K.J., 2019, Equine electrocardiography, Vet Clin North Am Equine Pract 35(1), 65-83. https://doi.org/10.1016/j.cveq.2018.12.007. [ Links ]
Paslawska, U., Zysko, D., Noszczyk-Nowak, A., et al., 2012, Short-term and long-term PQ, QT and R-R intervals' variability at the resting condition and after exercise testing in healthy Anglo-Arabian horses, Pol J Vet Sci 15(1), 55-59. https://doi.org/10.2478/v10181-011-0114-8. [ Links ]
Reed, S., Bayly, W., Sellon, D.C., 2017, Equine internal medicine, 4th ed. Saunders. [ Links ]
Televet, 2018, Televet Version 7.0.0 Veterinary telemetric ECG system Documentation, Engel Engineering Services GmbH, Germany, Available from: https://kruuse.com/Files/Files/Pdf/SE/Televet%20II%20291308.pdf. Accessed 23 Jun 2019. [ Links ]
Van Loon, G., Patteson, M., 2010, Chapter 6 - Electrophysiology and arrhythmogenesis, In: Marr, C.M. & Bowen, I.M. (eds), Cardiology of the Horse, 2nd ed, Edinburgh: W.B. Saunders. https://doi.org/10.1016/B978-0-7020-2817-5.00011-0. [ Links ]
Vezzosi, T., Sgorbini, M., Bonelli, F., et al., 2018, Evaluation of a smartphone electrocardiograph in healthy horses: comparison with standard base-apex electrocardiography, J Equine Vet Sci 67, 61-65. https://doi.org/10.1016/j.jevs.2018.03.006. [ Links ]
Welch-Huston, B., Durward-Akhurst, S., Norton, E., et al., 2020, Comparison between smartphone electrocardiography and standard three-lead base apex electrocardiography in healthy horses, Vet Rec 187, e70. https://doi.org/10.1136/vr.105759. [ Links ]
 Correspondence:
Correspondence:
email: graeme.piketh@up.ac.za


{kind=link}
{kind=link}
{kind=link}