










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkJournal of the South African Veterinary Association
versión On-line ISSN 2224-9435
versión impresa ISSN 1019-9128
J. S. Afr. Vet. Assoc. vol.93 no.1 Pretoria 2022
http://dx.doi.org/10.36303/JSAVA.2022.93.1.489
ORIGINAL RESEARCH
Ketamine-medetomidine compared to tiletamine-zolazepam-medetomidine for immobilisation of semi-captive cheetahs (Acinonyx jubatus)
RK BuckI; ASW TordiffeII; GE ZeilerI
IDepartment of Companion Animal Clinical Studies, Faculty of Veterinary Science, University of Pretoria, South Africa
IIDepartment of Paraclinical Sciences, Faculty of Veterinary Science, University of Pretoria, South Africa
ABSTRACT
The immobilisation time and cardiopulmonary effects of ketamine-medetomidine (KM) and tiletamine-zolazepam-medetomidine (TZM) were compared in semi-captive cheetahs (Acinonyxjubatus). Seven healthy adult cheetahs were included in a randomised prospective crossover study. Each cheetah was immobilised on two occasions by remote injection, once with a combination of ketamine (4.93 ± 0.75 mg/kg) and medetomidine (0.038 ± 0.003 mg/kg) (KM) and once with tiletamine-zolazepam (1.16 ± 0.12 mg/kg) and medetomidine (0.039 ± 0.002 mg/kg) (TZM). Time to safe approach, characterised by absent responses to an ear flick and tail tug, was recorded as the immobilisation time. Following immobilisation, cardiopulmonary parameters were recorded, and an arterial blood gas sample analysed. Data is reported as mean ± SD and compared using a general linear mixed model (p < 0.05). Immobilisation times were no different between combinations, 11.4 ± 5.7 minutes for KM and 13.2 ± 4.6 minutes for TZM (p = 0.528). Systolic blood pressure was 218 ± 22 mmHg for KM and 210 ± 28 mmHg for TZM (p = 0.594). There was moderate hypoxaemia with both combinations with arterial oxygen partial pressure of 58.4 ± 6.6 mmHg for KM and 61.3 ± 4.2 mmHg for TZM (p = 0.368). Haematocrit was higher with KM (40.7 ± 2.5) than TZM (35.8 ± 2.8, p = 0.007). There were differences in electrolytes, with TZM resulting in higher serum potassium (4.3 ± 0.2 mmol/L, p < 0.001) and glucose (11.8 ± 2.9 mmol/L, p = 0.039) than KM. Both combinations provided acceptable immobilisation for field use, although severe hypertension was a consistent finding. Supplementation with oxygen is recommended with both combinations.
Keywords: Acinonyx jubatus, cheetah, immobilisation, ketamine, medetomidine, tiletamine-zolazepam.
Introduction
Working with wild animals requires effective restraint to facilitate even simple procedures. For larger wild felids, such as cheetahs, lions or leopards, chemical capture is considered safer than physical restraint for both personnel and animals. Chemical capture, or immobilisation, is the administration of various combinations of sedative or anaesthetic drugs to render an animal sufficiently sedated or anaesthetised to permit physical manipulation (Chinnadurai et al. 2016). The goal of any immobilisation is a calm, predictable and reliable induction of heavy sedation or anaesthesia to ensure an animal is safe to work with, while concurrently maintaining homeostatic cardiopulmonary function (Chinnadurai et al. 2016).
A recent global survey completed by 75 veterinarians proficient with cheetah capture, reported ketamine-medetomidine (KM, 75% of respondents) and tiletamine-zolazepam-ketamine (TZM, 28% of respondents) to be the two most commonly chosen immobilisation protocols used to immobilise cheetahs (Braud et al. 2019).
Ketamine is a dissociative anaesthetic drug that acts primarily as an N-methyl-D-aspartate receptor antagonist. Similarly, tiletamine, provides dissociative anaesthesia through a similar pharmacological manner, though it is comparatively more potent than ketamine (Lin et al. 1993). Tiletamine is only available in proprietary combinations with the sedative benzodiazepine receptor agonist drug zolazepam. Medetomidine is an alpha-2 adrenoceptor agonist sedative drug which is commonly administered in combination with dissociative anaesthetics for its profound anaesthetic sparing effects, reliable sedation and muscle relaxation (Deem et al. 1998; Sinclair 2003; Stegmann & Jago 2006).
The aim of this study was to compare KM with TZM for immobilisation of semi-captive cheetahs, with particular focus on effective immobilisation time, as indicated by the time to safe handling, cardiovascular function and blood gas parameters following immobilisation. We hypothesised that there would be no difference in immobilisation time or physiological parameters between the immobilisation combinations.
Materials and methods
This study was performed with the approval of the University of Pretoria Animal Ethics committee. The study took place at the AfriCat Foundation near Otjiwarongo, in Namibia. The study site was 1 460 m above sea level and the barometric pressure ranged from 621-636 mmHg (82.8-84.8 kPa). This trial formed part of a larger project investigating field-ready immobilisation and anaesthetic drug protocols; only data relevant to this trial are reported here.
Animals and housing
Seven semi-captive cheetahs (two females, five males) from the AfriCat Foundation were included in a randomised, prospective, crossover study, where each animal was immobilised on two separate occasions, with two different combinations, with one year between immobilisations. The cheetahs weighed between 30.8 and 50.6 kg and were between five and 15 years of age at the time of the trial. Cheetahs were housed in large camps (5-20 ha) in small family groups of three to five animals.
Cheetahs were immobilised to facilitate an annual health evaluation that included blood collection, dental procedures, and gastroscopy.
Drug combinations
Two drug combinations for immobilisation were compared at the following target doses: 1.) ketamine (5 mg/kg; Ketamine-Fresenius, Fresenius Kabi, South Africa) and medetomidine (0.04 mg/kg; Medetomidine 10 mg/ml, Kyron Laboratories, South Africa) (treatment KM), and 2.) zolazepam-tiletamine (1.2 mg/kg; Zoletil, Virbac, South Africa) and medetomidine (0.04 mg/kg) (treatment TZM). Body mass used for drug calculations was estimated based on historical records and visual assessment by experienced wildlife veterinarians.
Immobilisation
Food was withheld for 24 hours prior to each immobilisation, although free access to water was allowed until darting. Prior to immobilisation, the preselected cheetah was moved into the small management camp (5 x 5 m; water access point and 2 x 1 m canvas roof for shelter) adjacent to their home camp to facilitate darting.
The immobilisation combination was delivered by a 1.5 ml charged dart (1.5 mm x 25 mm uncollared) delivered by a carbon dioxide powered dart rifle (Dan Inject, Denmark) into the muscles of the shoulder. Timing commenced at the time of rifle discharge, using a dedicated stopwatch. Once recumbent, the cheetah was approached from the rear and the tail was tugged and the ear flick tested. Absence of response to both was used to deem sufficient depth of immobilisation to allow safe handling. The time from darting to safe handling was recorded as the immobilisation time.
Thereafter, a blindfold was applied to reduce exposure to external stimuli and the cheetah was transported to the procedure room by pickup truck (up to 10 minutes' drive).
Physiological monitoring
Upon arrival in the procedure room, the cheetah was weighed using an electronic veterinary scale. An intravenous catheter was placed aseptically into a medial saphenous vein (18G Jelco; Smiths Medical Ltd, South Africa) to enable intravenous access for fluid and drug administration. The cheetah's trachea was intubated via the orotracheal route, using an illuminated laryngoscope (Macintosh-blade 4; Welch Allyn, USA) with a cuffed polyvinyl chloride endotracheal (ET) tube (internal diameter 8.0 to 10.0 mm). Any animal which was inadequately anaesthetised to allow intubation, indicated by head avoidance or chewing on mouth opening, was administered ketamine (0.5 mg/kg IV, bolused to effect). The total amount of ketamine administered was recorded. Following intubation, a dorsal pedal artery was cannulated (20G Jelco; Smiths Medical Ltd, South Africa) to facilitate measurement of arterial blood pressure and arterial blood sampling.
Invasive systolic (SAP), mean (MAP) and diastolic (DAP) blood pressure as well as pulse rate were measured using a multiparameter monitor (CardioCap 5; Datex-Ohmeda, Finland) connected via non-compliant tubing to an electronic strain gauge transducer (DTX Plus Disposable Transducer; BD Medical, South Africa) zeroed to atmospheric air pressure at the level of the right atrium. Heart rate (HR) was taken from lead II of the monitor's electrocardiogram, with leads connected in base-apex configuration. In addition, the end-tidal carbon dioxide and respiratory frequency were measured by the multiparameter monitor through a side stream connector attached to the end of the endotracheal tube.
Peripheral oxyhaemoglobin saturation was measured using a transmittance pulse oximeter probe (Nonin Medical, MN, USA) attached to the tongue. Rectal temperature was measured using a digital thermometer (HI98509 Checktemp 1; Hanna Instruments, South Africa). Any cheetah presenting with a temperature above 40.5 °C which continued to increase was actively cooled by wetting and application of fans.
After instrumentation, an arterial blood sample was anaerobically collected and analysed on site within five minutes of collection using a portable self-calibrating blood gas analyser (EPOC BGEM and smart cards; Epocal, Canada). The blood gas analyser measured arterial partial pressures of oxygen (PaO2) and carbon dioxide (PaCO2), arterial blood pH, blood glucose and electrolytes (Na+, K+, Ca2+) as well as haematocrit and haemoglobin. It also calculated bicarbonate (HCO3-) and base excess (extracellular fluid). The arterial blood samples were interpreted using alphastat algorithms (temperature 37.0 °C). The cardiopulmonary parameters and temperature were recorded at the end of instrumentation (10-15 minutes post time to safe handling), simultaneously with arterial blood collection, for data analysis.
Following collection of arterial blood gas samples and recording of cardiopulmonary parameters, data collection for this trial was considered complete. Anaesthesia was maintained using either volatile anaesthesia or total intravenous anaesthesia with propofol to allow for gastroscopy and dental examination. Supplemental oxygen (2.0 L/minute) was provided to all animals after completion of sample collection. Due to differences in methods of maintaining anaesthesia, recovery times are not reported as part of this trial. However, all cheetahs made a full recovery and returned to their normal daily routine after the annual health evaluations.
Statistical analysis
The alveolar to arterial oxygen partial pressure (P(A-a)O2) was calculated as described by Wagner (2015). The arterial to end-tidal CO2 partial pressure gradient (P(a-E')CO2) was calculated as the difference between the PaCO2 and the PECO2. Distribution of data was assessed for normality by evaluating descriptive statistics, plotting histograms and performing the Anderson-Darling test for normality and found to be parametric. Physiological, electrolyte and blood gas variables were compared between combinations using a paired f-test. Body masses, drug dosages and immobilisation times were also compared using paired f-tests. Additionally, the 95% confidence interval for difference between the means (CI) and Cohen's d (d) were calculated for each variable of comparison to assess the effect size. Time variables were compared using values in seconds and then converted to minutes for reporting. Data were presented as mean ± standard deviation (SD). Where available, known reference ranges for cheetahs were used for interpretation of results (potassium, sodium; Hudson-Lamb et al. 2016) and where reference ranges are unknown, those for lions (glucose, haematocrit; Broughton et al. 2017) or domestic cats (blood pressure Acierno et al. 2018; acid-base Hopper & Haskins 2008) were used. Data were analysed using commercially available software (MiniTab) and results were interpreted with a 5% level of significance (p < 0.05).
Results
All cheetahs successfully completed the trial and had resumed normal behaviour by the day after anaesthesia. The body weight for the cheetahs when receiving KM was 38.9 ± 5.7 kg and not different to when they received TZM at 38.7 ± 7.0 kg (p = 0.948, T-value = 0.07, d = 0.04, CI -7.30; 7.76).
For treatment KM, the dose of ketamine administered was 4.93 ± 0.75 mg/kg and that for medetomidine was 0.038 ± 0.003 mg/kg. For treatment TZM, the dose of zoletil administered was 1.16 ± 0.12 mg/kg and that for medetomidine was 0.039 ± 0.002 mg/kg. There was no difference in the dose of medetomidine administered to cheetah between treatments (p = 0.627, T-value = -0.5, d = 0.27, CI -0.00462; 0.00292).
The immobilisation time for treatment KM was 11.4 ± 5.7 minutes, which was no different to that for treatment TZM, which was 13.2 ± 4.6 minutes (p = 0.528, T-value = -0.65, d = 0.35, CI -411; 255). An additional bolus of ketamine was required to facilitate intubation in five cheetahs during treatment KM (0.9 ± 0.3 mg/kg) and in two cheetahs following treatment TZM (1.2 ± 0.3 mg/kg) (p = 0.103).
There were no differences in the physiological variables between treatments (Table I). A clinically relevant observation was that all cheetahs had elevated arterial blood pressures, with SAP of 218 ± 22 mmHg following treatment KM and 210 ± 28 mmHg following TZM (p = 0.595).
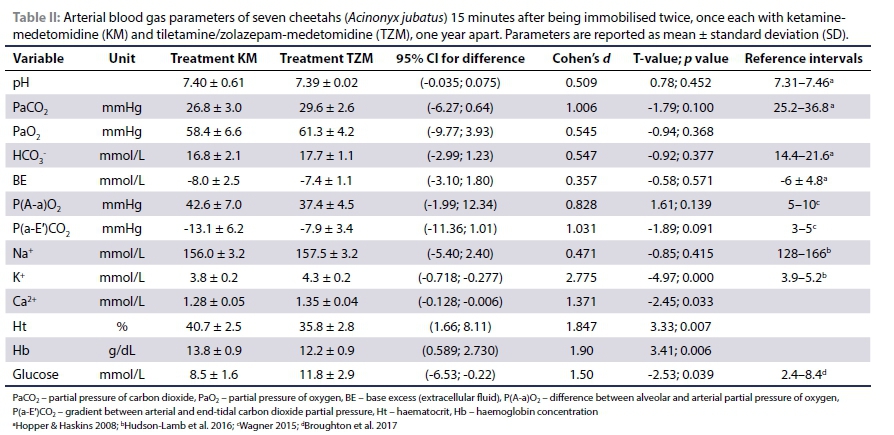
Blood gas, calculated indices and electrolytes are reported in Table II. There were no differences in arterial blood gas variables or calculated oxygenation and ventilation indices between treatments. With both treatments, cheetahs had a PaO2 of less than 80 mmHg and were normocapnic. With both treatments, there was a negative P(a-E')CO2.
There were significant differences in electrolyte concentrations (particularly potassium and calcium) and haematocrit values between treatments, although all values were within expected reference intervals. Both treatments resulted in blood glucose above 8.4 mmol/L, with treatment TZM causing significantly higher serum glucose concentrations than treatment KM.
Discussion
Combinations of ketamine or tiletamine-zolazepam with medetomidine were effective in immobilising cheetahs in a predictable manner with similar cardiopulmonary effects. Both combinations resulted in profound hypertension and moderate hypoxaemia, with notable differences in concentrations of blood potassium and glucose.
The doses of drugs chosen for this study were based on the authors' previous experience of working with semi-captive cheetahs. Others have reported much higher doses of ketamine (6.9 mg/kg) used to immobilise captive cheetahs than those used in this study, combined with a lower dose of medetomidine (0.027 mg/kg) (Stegmann & Jago 2006). In a global survey of veterinarians working with cheetahs, however, commonly used doses of ketamine and medetomidine in combination ranged from 2.37 to 3.25 mg/kg and 0.048 to 0.073 mg/kg, respectively (Braud et al. 2019). This reflects a lower dose of ketamine than the current study, and a higher dose of medetomidine. In the same survey, common dosages of TZ are reported as 1.2 to 1.5 mg/kg, combined with 0.04 to 0.06 mg/kg medetomidine; similar to those used in the present study (Braud et al. 2019). The dosages used in this study were within the normal working range and reflected practical choices for clinical use in semi-captive human-habituated cheetahs.
Traditionally in wildlife capture, there has been emphasis on rapid immobilisation, as a slow immobilisation time is thought to be associated with increased chance of overexertion, myopathy, or injury from environmental hazards, particularly for free-roaming animals (Arnemo et al. 2006). However, it is difficult to compare immobilisation time across different studies, due in part to different: 1) drug dosages used; 2) methods of drug delivery; 3) levels of habituation of animals to humans; and 4) endpoints used to define completion of immobilisation. Time to safe handling was used in this study to define immobilisation time because it presents a practical and definite endpoint for immobilisation. The time to lateral recumbency is commonly used but may not be practical as not all animals become laterally recumbent, particularly in felids, that may crouch in sternal recumbency with the head resting close to or on the ground soon after darting (Semjonov et al. 2019). Further, this measure may not be clinically useful as recumbency does not guarantee sedation and recumbent but insufficiently sedated animals may still pose a significant threat to personnel safety (Chinnadurai et al. 2016). While time to safe handling provides a definable endpoint to immobilisation, its use may on occasion result in unnecessarily long immobilisation times being recorded, such as cases where depth of sedation is in doubt and personnel safety is prioritised over testing immobilisation. The use of either KM or TZM in this study resulted in immobilisation times similar to those previously documented by Stegmann and Jago (2006) of 9.2 ± 3.4 min for KM and 16.8 ± 18.1 min for TZM, which were considered acceptable for captive animals.
The difference in potency of ketamine or tiletamine in cheetahs is not known and is complicated by the addition of zolazepam to tiletamine formulations. However, tiletamine is described as being at least twice to four times as potent as ketamine (Clarke et al. 2014; Lin et al. 1993). Given the similar immobilisation times in this study, the dosages administered could be considered equi-effective for immobilisation purposes, thereby allowing for comparison of physiological parameters in a clinically relevant way. However, it should be mentioned that there was a greater need for ketamine boluses prior to intubation following treatment KM (n = 5) versus TZM (n = 2). This indicates that while immobilisation time was similar, TZM resulted in more profound sedation than KM. Zolazepam has been shown to improve muscle relaxation and sedation when compared to tiletamine alone and likely contributed to the decreased need for ketamine boluses (Lin et al. 1993). The longer duration of action of tiletamine or a relatively lower dose of ketamine used could also have contributed (Braud et al. 2019; Clarke et al. 2014).
Based on the definition recommended for use in domestic cats, a systolic blood pressure of greater than 180 mmHg is considered severely hypertensive and a significant risk for target organ damage when sustained (Acierno et al. 2018). Cheetahs became markedly hypertensive with both immobilisation combinations, with systolic pressures well above 180 mmHg. Arterial blood pressure is the product of systemic vascular resistance and cardiac output, which itself is the product of heart rate and stroke volume (Clarke et al. 2014). Medetomidine causes pronounced vasoconstriction through action at peripheral alpha-2 adrenoreceptors, which is seen clinically as the dramatic increase in blood pressure (Pypendop & Verstegen 1998). Hypertension following the use of medetomidine is well documented in cheetah immobilisation where high doses of medetomidine are used to facilitate capture (Deem et al. 1998; Semjonov et al. 2019; Stegmann & Jago 2006). Both ketamine and tiletamine may indirectly potentiate the hypertension through indirect sympathetic activation. Both drugs cause an increase in circulating endogenous catecholamines leading to activation of vascular postsynaptic alpha-1 adrenoceptors, thereby enhancing vasoconstriction and the release of noradrenaline within the myocardium, resulting in increased cardiac inotropy and chronotropy (Berry 2015). It should be cautioned that acute, severe hypertension poses a risk of haemorrhage or oedema in the brain or lungs, while sustained hypertension can cause retinal lesions, encephalopathy and renal damage (Acierno et al. 2018). Although no cheetahs in this study appeared to suffer any ill effects of the hypertension, follow-up studies would be required to be certain. An avenue for future studies is the peripheral acting alpha-2 adrenoceptor antagonist vatinoxan (MK-467), which has been shown in dogs to reverse the vasoconstrictive effects of medetomidine without affecting the central effects and thus may prove useful in preventing hypertension without altering depth of sedation (Rolfe et al. 2012).
In domestic dogs and cats, the hypertension seen with medeto-midine is usually accompanied by a baroreceptor-mediated reflex reduction in heart rate (Sinclair 2003). This is compounded by an alpha-2 adrenergic agonist-mediated dampening of sympathetic tone through reduced noradrenaline outflow within the central nervous system (Sinclair 2003). With this in mind, the HR observed in this study are perhaps higher than expected at 66 ± 9 beats/minute for KM and 72 ± 7 beats/minute for TZM, especially when compared to beagle dogs receiving 0.01 to 0.02 mg/kg medetomidine, where HR was close to 40 beats/minute (Pypendop & Verstegen 1998). This may suggest that the chronotropic effects of the dissociative anaesthetic drugs may have an important effect. The higher-than-expected heart rate could potentially also be the result of an initial phase of compensation due to myocardial hypoxia as a result of the low PaO2.
With both combinations of drugs, a reversal of the P(a-E')CO2 was observed. Generally, there is a positive difference between the PaCO2 and PE'CO2 of 2 to 5 mmHg that results from physiological ventilation-perfusion (V/Q) mismatching in the lungs (Hudcova & Schumann 2006). Where the difference becomes negative, it is termed 'reversed', and although less common, it is well documented in neonates, pregnancy, obesity, exercise and with malignant hyperthermia (Lin et al. 2014; Shankar et al. 1991). The underlying physiological mechanism causing this gradient to reverse is thought to be a low ventilatory rate and large tidal volume in combination with a relatively high cardiac output state (Shankar et al. 1991). This allows gas emptying from "slow" alveoli to reach the mouth and also relatively better ventilation of well perfused alveoli causing low V/Q compartments to make a more substantial contribution to gas exchange, ultimately resulting in PE'CO2 exceeding PaCO2 (Shankar et al. 1991). Curiously, despite the use of medetomidine, where the profound vasoconstriction and subsequent hypertension stereotypically result in a rebound bradycardia and reduced cardiac output (Sinclair 2003), the reversal of the P(a-E')CO2 gradient suggests that cardiac output may have been maintained. Cardiac output was not measured in this study; however, the dissociative anaesthetic agents are known to increase inotropy and chronotropy, which may offset a medetomidine-induced decrease in cardiac output (Lin et al. 1993). An additional contributing factor may have been an apneustic breathing pattern, as is commonly seen with dissociative anaesthetic drugs, the pattern of gas emptying from the alveoli (Lin et al. 1993). It should be noted that this reversed gradient could also result artefactually from samples being collected at different times; however, every effort was made to collect blood gas samples and record PE'CO2 within the same minute.
Hypoxaemia, defined as a PaO2 of less than 80 mmHg (10.7 kPa), was a finding with both combinations. This is consistent with previous trials with the same immobilisation drugs (Deem et al. 1998; Stegmann & Jago 2006). Minute ventilation was not determined, and only respiratory rate, PE'CO2 and PaCO2 were used as indicators of ventilation. All three variables were within expected reference intervals, and while there may have been a degree of hypoventilation contributing to the hypoxaemia, the widening of the P(A-a)O2 gradient is highly suggestive of oxygen diffusion impedance or right-to-left intrapulmonary shunting rather than dead space ventilation or hypoventilation as major causes (Wagner 2015). In dogs, medetomidine has been shown to increase pulmonary artery pressure, and pulmonary hypertension has been shown to cause right-to-left intrapulmonary shunting and oxygen diffusion deficits when the rapid transit time of blood decreases time for oxygen diffusion (Rolfe et al. 2012; Vodoz et al. 2009). It has been shown that even in healthy people, there is insufficient transit time for oxygen to equilibrate following exercise at altitude, due to high flow rates and decreased red cell transit times with the relatively low available oxygen (Wagner et al. 1986), and although at intermediate altitude (1 460 m), a similar scenario could be envisioned with these cheetahs following excitation at darting. A final thought regarding the cause of the hypoxaemia is that there may have been a lower oxygen content in the blood returning to the pulmonary capillaries, resulting in a widened P(A-a)O2 (Wagner 2015). Two plausible explanations exist for this - either the cheetahs may have been in a state of high oxygen demand following darting, resulting in a relative oxygen deficit or the speculated vasoconstriction and decreased cardiac output caused by the medetomidine may have delayed blood flow through the peripheral tissues, allowing extra time for oxygen extraction (Kaartinen et al. 2010). Regardless of the cause, the moderate hypoxaemia seen highlights the importance of supplemental oxygen being provided to animals immobilised with either combination.
Although the normal reference interval for blood glucose for cheetahs has not been established, that of immobilised free-ranging lions is reported as 42.6 to 151.0 mg/dL (2.4 to 8.4 mmol/L) (Broughton et al. 2017). By this definition, both combinations resulted in mild hyperglycaemia. Medetomidine is well documented as causing increased plasma glucose concentrations, presumably through its actions of decreasing insulin secretion in combination with stimulation of glyco-genolysis in the liver (Ambrisko & Hikasa 2002). Additionally, ketamine is known to cause an increase in blood glucose when used for induction in people and given their similar pharmacodynamic actions, a similar response to tiletamine could be anticipated (Gal & Malit 1972). However, while both combinations included the same dose of medetomidine, when administered TZM, there was a significantly higher blood glucose than with KM. In humans, benzodiazepine agonists have been shown to decrease insulin sensitivity and interfere with non-insulin-mediated glucose disposal, and there is a trend towards increasing serum glucose concentrations in the blood after a single dose of diazepam (Chevassus et al. 2014; Syvälahti & Kanto 1975). Zolazepam may therefore contribute to the hyperglycaemia. Further investigation is required but this is an important consideration when assessing health based on blood results.
Serum potassium remained within the normal reference intervals established for cheetahs with both treatments (Hudson-Lamb et al. 2016). However, hyperkalaemia is a serious complication reported frequently during immobilisation of wild felids, and curiously treatment TZM resulted in significantly higher serum potassium than KM (Romano et al. 2018; Steeil et al. 2013). Medetomidine has been implicated in many cases of hyperkalaemia (Reilly et al. 2014; Steeil et al. 2013). Possible mechanisms of action include a medetomidine-induced decrease in insulin secretion causing a decrease in Na/K-ATPase-mediated intracellular influx potassium (Reilly et al. 2014) or a release of potassium from the liver during catecholamine stimulation as a result of alpha-1 and alpha-2 adrenoreceptor-mediated activity of calcium-dependent potassium channels (Moratinos & Reverte 1993). Ketamine induction is generally associated with a decrease in serum potassium from baseline (Gal & Malit 1972), and we speculate the same would be true for tiletamine. However, the difference between the combinations suggest there may be additional contribution from zolazepam. This is supported by findings in rhesus monkeys, were tiletamine-zolazepam for immobilisation resulted in higher serum potassium than ketamine alone (Woodward & Weld 1997). Whether this is a result of the anti-insulin effects of the benzodiazepine agonist, a novel mechanism or simply artefactual requires further investigation.
Although there were significant differences in haematocrit between the two treatments, they remained within normal reference intervals. An explanation for this based on drug effect is unlikely, and in dogs the use of ketamine or TZ did not result in different haematocrit values (Hampton et al. 2019). This could be artefactual or may reflect differences in management practices, such as ecto- and endoparasite control.
An additional consideration when comparing the two combinations is the volume of drugs to be administered. When using the standard commercial formulations of ketamine (100 mg/ml) and tiletamine-zolazepam (100 mg/ml), there is a notable difference in the volume to be administered between the two combinations. For a 40 kg cheetah, the KM dose to administer would be over 2 ml, while for the ZM the dose would be less than 0.5 ml. Darts of smaller volume have been advocated to avoid injury, as the lighter the dart, the lower the kinetic energy at impact (Caulkett & Arnemo 2015). Additionally, reducing dart volume can decrease the injection velocity and improve the accuracy of dart placement, as a lighter dart has more accurate flight (Caulkett & Arnemo 2015). This difference in doses may also be important where semi-tame or tame animals are immobilised by hand injection, where it is easier to inject a smaller volume.
A major limitation in this study is that recovery was not assessed. With wild animals, recovery from anaesthesia should be rapid and complete to reduce chance of injury following release (Chinnadurai et al. 2016). The effect of immobilisation drugs plays an important role in recovery characteristics following short periods of anaesthesia and assessment of recovery time and quality would give a more complete comparison of the combinations. In this study, anaesthesia was prolonged for over an hour using different maintenance drugs (propofol or isoflurane) (Buck et al. 2017), and as a result, recovery characteristics of these drug combinations were not assessed. Another limitation is the delay between the time to safe approach and the collection of cardiopulmonary data. Although a time delay was unavoidable due to the clinical nature of the study, faster instrumentation would have allowed for better comparison of the effects of immobilisation. Similarly, collection of a second data set five to 10 minutes after the first data set would have been valuable; however, this was not possible due to the administration of different drugs for anaesthetic maintenance. A further limitation to this study is the long time period between data collections, whereby a whole year elapsed between anaesthetic episodes. This was intended to allow data collection to coincide with normal clinical management of the cheetahs. While all anaesthetic procedures were standardised, there may have been differing management practices over different years, such as different feeding practices or parasite management plans, which may have caused changes in the cheetahs' physiology.
Conclusion
Both KM and TZM provide reliable, similar immobilisation for semi-captive cheetahs in a field setting. However, both combinations resulted in hypertension and hypoxaemia, and as such, careful monitoring of blood pressure and provision of supplemental oxygen is advised when using these drugs. Further investigation is required into the role of zolazepam in glucose and potassium homeostasis.
Ethical approval
This study was performed with the approval of the University of Pretoria Animal Ethics committee.
ORCID
RK Buck https://orcid.org/0000-0001-5999-2751
ASW Tordiffehttps://orcid.org/0000-0001-5416-3153
GE Zeiler https://orcid.org/0000-0001-7653-7726
References
Acierno, M.J., Brown, S., Coleman, A.E., et al., 2018, ACVIM consensus statement: Guidelines for the identification, evaluation, and management of systemic hypertension in dogs and cats, J Vet Int Med 32(6), 1803-1822. https://doi.org/10.1111/jvim.15331. [ Links ]
Ambrisko, T.D., Hikasa, Y., 2002, Neurohormonal and metabolic effects of medetomidine compared with xylazine in beagle dogs, Can J Vet Res 66(1), 42-49. [ Links ]
Arnemo, J.M., Ahlgyist, P., Andrsen, R., et al., 2006, Risk of capture-related mortality in large free-ranging mammals: Experiences from Scandinavia, Wild! Biol 12(1), 109-113. https://doi.org/10.2981/0909-6396(2006)12[109:ROCMIL]2.0.CO;2. [ Links ]
Berry, S.H., 2015, Injectable anesthetics in Grimm, K.A., Lamont, L.A., Tranquilli, W.J., Greene, S.A., Robertson, S.A. (eds) Veterinary Anesthesia and Analgesia: The Fifth edition of Lumb and Jones, Ames, Iowa: Wiley Blackwell, pp 283-286. [ Links ]
Braud, C., Mitchell, E.P., Van der Merwe, V., Tordiffe, A.S.W., 2019, A veterinary survey of factors associated with capture-related mortalities in cheetahs (Acinonyx jubatus), J S Arf Vet Assoc 90(0), 1-7. https://doi.org/10.4102/jsava.v90i0.1723. [ Links ]
Broughton, H.M., Govender, D., Shikwambana, P., et al., 2017, Bridging gaps between zoo and wildlife medicine: establishing reference intervals for free-ranging African lions (Panthera leo), J Zoo Wildl Med 48(2), 298-311. https://doi.org/10.1638/2016-0021R.1. [ Links ]
Buck, R.K., Tordiffe, A.S.W., Zeiler, G.E., 2017, Cardiopulmonary effects of anaesthesia maintained by propofol infusion versus isoflurane inhalation in cheetahs (Acinonyx jubatus), Vet Anaesth Analg 44(6), 1363-1372. https://doi.org/10.1016/j.vaa.2017.05.007. [ Links ]
Caulkett N.A., Arnemo J.M., 2015. Comparative anesthesia and analgesia of zoo animals and wildlife in Grimm, K.A., Lamont, L.A., Tranquilli, W.J., Greene, S.A. & Robertson, S.A. (eds) Veterinary Anesthesia and Analgesia: The Fifth edition of Lumb and Jones, Ames, Iowa: Wiley Blackwell, pp 764-776. https://doi.org/10.1002/9781119421375.ch40. [ Links ]
Clarke, K.W., Trim, C.M., Hall, L.W., 2014, Veterinary anaesthesia, 11th edn, WB Saunders, Oxford, pp13-80. [ Links ]
Chevassus, H., Mourand, I., Molinier, N., et al., 2004, Assessment of singledose benzodiazepines on insulin secretion, insulin sensitivity and glucose effectiveness in healthy volunteers: a double-blind, placebo-controlled, randomized cross-over trial [ISRCTN08745124], BMC Clin Pharmacol 4(3), 1-10. https://doi.org/10.1186/1472-6904-4-3. [ Links ]
Chinnadurai, S.K., Strahl-Heldreth, D., Fiorello, C.V., Harms, C.A., 2016, Best-practice guidelines for field-based surgery and anesthesia of free-ranging wildlife. I. Anaesthesia and analgesia, J Wildl Dis 52(2S), 14-27. https://doi.org/10.7589/52.2S.S14. [ Links ]
Deem, S.L., Ko, J.C.H., Citino, S.B., 1998, Anesthetic and cardiorespiratory effects of tíletamíne-zolazepam-medetomídíne in cheetahs, J Am Vet Med Assoc 213(7), 1022-1026. [ Links ]
Gal, T.J., Malit, L.A., 1972, The influence of ketamine induction on potassium changes and fasciculations following suxamethonium, Br J Anaesth 44(10), 1077-1080. https://doi.org/10.1093/bja/44.10.1077. [ Links ]
Hampton, C.E., Riebold, T.W., LeBlanc, N.L., et al., 2019, Effects of intravenous administration of tiletamine-zolazepam, alfaxalone, ketamine-diazepam, and propofol for induction of anesthesia on cardiorespiratory and metabolic variables in healthy dogs before and during anesthesia maintained with isoflurane, Am J Vet Res 80(1), 33-44. https://doi.org/10.2460/ajvr.80.L33. [ Links ]
Hopper, K., Haskins, S.C., 2008, A case-based review of a simplified quantitative approach to acid-base analysis, J Vet Emerg Crit Care 18(5), 467-476. https://doi.org/10.1111/j.1476-4431.2008.00344.x. [ Links ]
Hudson-Lamb, G.C., Schoeman, J.P., Hooijberg, E.H., et al. 2016, Reference intervals for selected serum biochemistry analytes in cheetahs (Acinonyx jubatus), J S Afr Vet Assoc 87(1), 1-6. https://doi.org/10.4102/jsava.v87i1.1316. [ Links ]
Hudcova, J., Schumann, R., 2006, Arterial to end-tidal CO2 gradient reversal during laparoscopic pheochromocytoma resection, Can J Anesth 53(4), 409-412. https://doi.org/10.1007/BF03022509. [ Links ]
Kaartinen, J.M., Pang, D.S.J., Moreau, M., et al., 2010, Hemodynamic effects of an intravenous infusion of medetomidine at six different dose regimens in isoflurane-anesthetized dogs, Vet Therap 11(1), 1-16. [ Links ]
Lin, H.C., Thurmon, J.C., Benson, G.J., Tranquilli, W.J., 1993, Telazol - a review of its pharmacology and use in veterinary medicine, J Vet Pharmacol Therap 16(4), 383-418. https://doi.org/10.1111/j.1365-2885.1993.tb00206.x. [ Links ]
Lin, H.-T., Wang, S.-C., Zuo, Z., et al., 2014, Increased requirement for minute ventilation and negative arterial to end-tidal carbon dioxide gradient may indicate malignant hyperthermia, J Chinese Med Assoc 77(4), 209-212. https://doi.org/10.1016/j.jcma.2014.01.002. [ Links ]
Moratinos, J., Reverte, M., 1993, Effects of catecholamines on plasma potassium: the role of alpha- and beta-adrenoreceptors, Fundam Clin Pharmacol 7(3-4), 143-153. https://doi.org/10.1111/j.1472-8206.1993.tb00228.x. [ Links ]
Pypendop, B., Verstegen, J.P., 1998, Hemodynamic effects of medetomidine in the dog: a dose titration study, Vet Surg 27(6), 612-622. https://doi.org/10.1111/j.1532-950X.1998.tb00539.x. [ Links ]
Reilly, S., Seddighi, MR., Steeil, J.C., et al., 2014, Selected clinical, biochemical, and electrolyte alterations in anesthetized captive tigers (Panthera tigris) and lions (Panthera leo), J Zoo Wildl Med 45(2), 328-334. https://doi.org/10.1638/2013-0202R.1. [ Links ]
Rolfe, N.G., Kerr, C.L., McDonnell, W.N., 2012, Cardiopulmonary and sedative effects of the peripheral a2-adrenoeceptor antagonist MK 0467 administered intravenously o intramuscularly concurrently with medetomidine in dogs, Am J Vet Res 73(5), 587-594. https://doi.org/10.2460/ajvr.73.5.587. [ Links ]
Romano, M., Boesch, J., Peralta, S., et al., 2018, Hyperkalemia in two jaguars (Panthera onca) anesthetized with dexmedetomidine, ketamine and isoflurane, J Zoo Wildl Med 49(2), 505-507. https://doi.org/10.1638/2017-0147.1. [ Links ]
Semjonov, A., Raath, J.P., Laubscher, L., et al., 2019, Evaluation of butorphanol- azaperone-medetomidine in captive cheetah (Acinonyx jubatus) immobilization, Vet Anaesth Analg 46(1), 90-95. https://doi.org/10.1016/j.vaa.2018.09.038. [ Links ]
Shankar, K.B., Moseley, H., Kumar, Y., 1991, Negative arterial to end-tidal gradients, Can J Anaesth 38(2), 260-261. https://doi.org/10.1007/BF03008164. [ Links ]
Sinclair, M.D., 2003, A review of the physiological effects of a2-agonists related to the clinical use of medetomidine in small animal practice, Can Vet J 44(11), 885-897. [ Links ]
Steeil, J., Ramsay, E.C., Schumacher, J., et al., 2013, Hyperkalemia in exotic felids anesthetized with an alpha - 2 adrenoreceptor agonist, ketamine, and isoflurane, ProcAnnual Conference AAZV, 13. [ Links ]
Stegmann, G.F., Jago, M., 2006, Cardiopulmonary effects of medetomidine or midazolam in combination with ketamine or tiletamine/zolazepam for the immobilisation of captive cheetahs (Acinonyx jubatus), J S Afr Vet Assoc 77(4), 205-209. https://doi.org/10.4102/jsava.v77i4.378. [ Links ]
Syvälahti, E.K.G., Kanto, J.H., 1975, Serum growth hormone, serum immunoreactive insulin and blood glucose response to oral and intravenous diazepam in man, Int J Clin Pharmacol 12(1-2), 74-82. [ Links ]
Vodoz, J.F., Cottin, V., Glerant, J.C., et al., 2009, Right-to-left shunt with hypoxaemia in pulmonary hypertension, BMC Cardiovascular Disorders 9(15), 1-7. https://doi.org/10.1186/1471-2261-9-15. [ Links ]
Wagner, P.D., Gale, G.E., Moon, R.E., et al., 1986, Pulmonary gas exchange in humans exercising at sea level and simulated altitude, J Appl Physiol 61(1), 260-270. https://doi.org/10.1152/jappl.1986.61.1.260. [ Links ]
Wagner, P.D., 2015, The physiological basis of pulmonary gas exchange: implications for clinical interpretation of arterial blood gases, Eur Respir J 45(1), 227-243.https://doi.org/10.1183/09031936.00039214. [ Links ]
Woodward, R.A., Weld, K.P., 1997, A comparison of ketamine, ketamine-acepromazine, and tiletamine-zolazepam on various hematologic parameters in Rhesus monkeys (Macaca mulatto), Contemp Top Lab Anim Sci 36(3), 55-57. [ Links ]
 Correspondence:
Correspondence:
email: roxanne.buck@up.ac.za


{kind=link}
{kind=link}