










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkJournal of the South African Veterinary Association
versão On-line ISSN 2224-9435
versão impressa ISSN 1019-9128
J. S. Afr. Vet. Assoc. vol.85 no.1 Pretoria Jan. 2014
http://dx.doi.org/10.4102/jsava.v85i1.1144
CASE REPORT
Congenital hypothyroidism and concurrent renal insufficiency in a kitten
Chee Kin LimI, II; Chantal T. RosaI; Yolanda de WittI; Johan P. SchoemanI
IDepartment of Companion Animal Clinical Studies, University of Pretoria, South Africa
IIDepartment of Veterinary Clinical Sciences, Purdue University, United States of America
ABSTRACT
A 3-month-old male domestic short-hair kitten was presented with chronic constipation and disproportionate dwarfism. Radiographs of the long bones and spine revealed delayed epiphyseal ossification and epiphyseal dysgenesis. Diagnosis of congenital primary hypothyroidism was confirmed by low serum total thyroxine and high thyroid stimulating hormone concentrations. Appropriate supplementation of levothyroxine was instituted. The kitten subsequently developed mild renal azotaemia and renal proteinuria, possibly as a consequence of treatment or an unmasked congenital renal developmental abnormality. Early recognition, diagnosis and treatment are vital as alleviation of clinical signs may depend on the cat's age at the time of diagnosis.
Introduction
Feline congenital hypothyroidism is a rare disease causing disproportionate dwarfism (Johnson & Watson 2010; Scott-Moncrieff 2007). Affected kittens have short limbs and spine, block-like trunks and broad, short skulls (Arnold et al. 1984; Crowe 2004; Scott-Moncrieff 2007; Szabo & Wells 2007). Besides the hallmark sign of failure to thrive, other clinical signs such as lethargy, impaired mental status, neuromuscular deficits, retention of juvenile hair coat, delayed dental eruption, constipation, bradycardia, hypothermia, sealed eyelids and stenotic ear canals, macroglossia, abdominal distension secondary to accumulation of myxoedematous fluid and bilateral cryptorchidism have also been observed in hypothyroid kittens (Bojanic, Acke & Jones 2011; Feldman & Nelson 2004; Johnson & Watson 2010; Mooney & Anderson 1993; Pettigrew et al. 2007; Quante et al. 2010, Scott-Moncrieff 2007; Szabo & Wells 2007). Causes of primary congenital hypothyroidism include thyroid dysgenesis (developmental defects of the thyroid gland and thyroid aplasia as a result of thyroid stimulating hormone [TSH] receptor abnormalities - non-goitrous) and thyroid dyshormonogenesis (defects in iodine uptake and thyroid hormone synthesis - goitrous) (Greco 2006). Familial dyshormogenesis has been described in a family of Abyssinian cats (Jones et al. 1992). Secondary hypothyroidism can occur as a result of TSH resistance (TSH receptor or gene mutation causing ineffective signal transduction or an abnormal TSH molecule) or TSH deficiency (Bojanic et al. 2011). Only cases of TSH resistance associated with defective TSH or its receptor have been reported in cats (Tanase, Kudo & Horikoshi 1991; Traas et al. 2008). Tertiary hypothyroidism associated with a lack of thyroid-releasing hormone (TRH) has not been reported in cats.
The purpose of this study case report was to describe the diagnosis, treatment and outcome of a dwarf kitten diagnosed with primary congenital hypothyroidism that subsequently developed renal azotaemia during treatment. Possible pathomechanisms for the renal insufficiency are discussed.
Ethical consideration
This is a case report describing a clinical case of a client-owned pet presenting to the Onderstepoort Veterinary Academic Hospital (OVAH). The animal reported was treated and housed according to the standard OVAH protocols for the management of client-owned pets. All diagnostic tests were performed as part of the work-up. No diagnostic tests or treatments were conducted for research purposes.
Informed consent
The owner of the cat reported here has given written consent for publishing purposes.
Case presentation
A 3-month-old male domestic short-hair kitten weighing 1.2 kg was presented with chronic constipation of 6 weeks' duration. An obviously small for age and disproportionate stature was noted. All four limbs and tail were short and stubby, whilst the head was broad with flattened facial features (Figure 1a). The coat was dry and oral examination revealed only a few semi-erupted incisor teeth and marked macroglossia. The abdomen was moderately distended with palpable firm faecal balls in the colon. Thoracic auscultation was within normal limits. Rectal temperature was mildly subnormal (37.3 °C). On neurologic examination, mental dullness and proprioceptive ataxia manifesting as a 'bunny-hopping' gait were detected.
In this case, disproportionate dwarfism was the most striking feature. Causes of congenital feline dwarfism include endocrinopathies such as hypothyroidism, hypopituitarism, juvenile diabetes mellitus and hypoadrenocorticism. Non-endocrine causes included portosystemic vascular anomalies, renal disease, osteochondrodysplasia, cardiac defects and lysosomal storage diseases (Johnson & Watson 2010). Malnutrition and gastrointestinal diseases were less likely causes of dwarfism based on the history and absence of vomiting and/or diarrhoea. Pituitary dwarfism was also considered unlikely as affected animals demonstrate proportionate dwarfism (Johnson & Watson 2010).
Peripheral blood smear, haematology, limited serum biochemistry profile, feline immunodeficiency virus (FIV) and feline leukaemia virus (FeLV) serological testing (Anigen Rapid FIV Ab/FeLV Ag Test Kit, Bionote Inc., Gyeonggi-do, Korea) and radiographs of the long bones and spine were performed. Haematology and peripheral blood smear evaluation were normal, but the haematocrit (0.25/L, reference interval [RI] 0.24-0.45), total red cell count (5.34 x 1012/L, RI 5.5-10.0) and haemoglobin (83 g/L, RI 80-140) were at the lower limit of the reference range. Serum biochemistry revealed severe hypercholesterolaemia (8.28 mmol/L, RI 1.8-3.8); FIV and FeLV testing were negative. Radiography revealed generalised delayed epiphyseal ossification and dysgenesis of the long bones and vertebrae (Figures 2a and 2b), delayed ossification of the carpal bones (Figure 3a) and spina bifida occulta (Figure 2b). Abdominal radiographs revealed megacolon with constipation (Figures 2a and 2b).

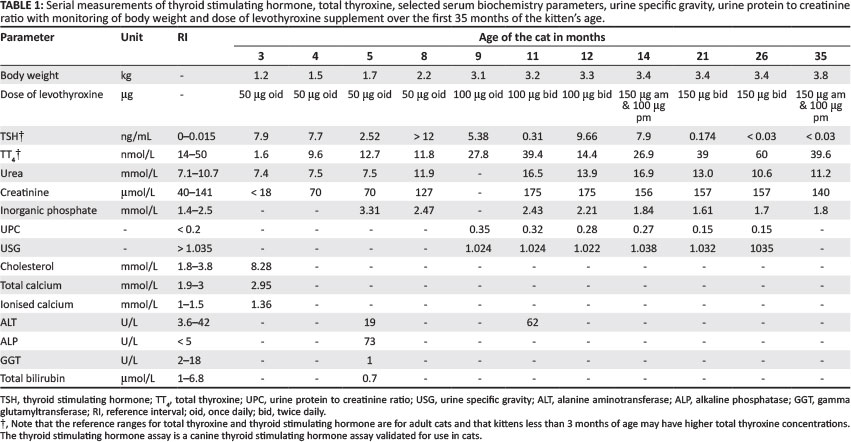
Serum total thyroxine (TT4) and TSH were subsequently performed. TT4 concentrations were measured (Immulite® 1000 Canine Total T4 analyser, Siemens Healthcare Diagnostic Products Ltd, United Kingdom) and TSH concentrations were measured (Immulite® 1000 canine TSH analyzer, Siemens Healthcare Diagnostic Products Ltd, United Kingdom) as previously validated for cats (Williams, Elliott & Syme 2010). This revealed severely decreased TT4 (1.62 nmol/L, RI 14-50) and markedly elevated TSH (7.9 ng/mL, RI 0-0.15) (Table 1 and Figure 4). Ultrasonography of the thyroid glands was within normal limits. The overall clinical signs, laboratory results and radiological findings were compatible with a diagnosis of primary congenital hypothyroidism.

Management and outcome
Treatment was initiated with levothyroxine 50 µg PO q 24h (Eltroxin®, Aspen Pharmacare) administered with food and lactulose 1 mL PO q 12h (Laxette®, Cipla Medpro) for 6 weeks. Marked improvement of the kitten's facial conformation from the originally broad head and flattened facial features to a more 'pointy' muzzle and lower jaw was noted on follow-up. The kitten was also more active. As expected, TT4 increased and TSH reduced over the months of follow-up (Table 1). The levothyroxine dose was adjusted accordingly. Up to 8 months of age, TT4 remained subnormal and TSH markedly elevated, likely as a result of the 'overdrive' effect of prolonged decreased TT4 on the pituitary. By 11 months of age, the kitten became polyuric and polydipsic with mild renal azotaemia and hyperphosphataemia, borderline proteinuria (urine protein to creatinine [UPC] ratio 0.32, RI 0.2-0.4) and inadequately concentrated urine (urine specific gravity [USG] 1.024). Abdominal ultrasound revealed hyperechoic renal cortices with poor corticomedullary definition. Systolic/diastolic blood pressure measurements were within normal limits at 125/89 mmHg. These findings were suggestive of non-hypertensive, borderline proteinuric, International Renal Interest Society stage 2 chronic renal insufficiency. The levothyroxine dose was further increased and thyroid and renal values monitored. Serial serum TT4, TSH, urea, creatinine, UPC and USG showed progressive improvement, with normalisation of all parameters over time, except for mild renal azotaemia, which persisted. Follow-up radiographs at 26 months of age (Figures 2c and 3b) revealed complete closure of the physes of the vertebrae and long bones, ossification of the carpal and tarsal bones and resolution of the spina bifida occulta. At the time of submission of the last draft of the manuscript the patient was 41 months old, led a normal life and was on a levothyroxine dose of 150 µg in the morning and 100 µg at night (Figure 1b).
Discussion
Even though congenital hypothyroidism is a very rare condition in cats, with few published reports (Arnold et al. 1984; Crowe 2004; Jones et al. 1992; Quante et al. 2010; Sjollema et al. 1991; Stephan & Schutt-Mast 1995; Szabo & Wells 2007; Tanase et al. 1991; Tobias & Labato 2001), the actual prevalence of feline congenital hypothyroidism may be higher than reported, as many kittens may have died undiagnosed or mistakenly been managed for chronic constipation (Bojanic et al.2011).
Thyroid hormones are essential for normal postnatal development of the skeletal and nervous systems (Greco 2006; Scott-Moncrieff 2007). Bone growth is influenced by thyroid hormone via two mechanisms, (1) stimulation of growth hormone production by the pituitary gland and (2) interaction with growth hormone to balance the sequence of growth cartilage production-degeneration and regulation of endochondral ossification until physeal closure (Saunders & Jezyk 1991). Therefore, delayed epiphyseal ossification and epiphyseal dysgenesis with disproportionate dwarfism are the hallmarks of congenital hypothyroidism (Greco 2006). An absolute definitive diagnosis of hypothyroidism requires a TSH or TRH stimulation test (Gunn-Moore 2005).
Thyroid hormones influence renal tubular function and electrolyte absorption or secretion, mitochondrial enzymes and neural renal functions (Braunlich 1984; Mariani & Berns 2012) and therefore hypothyroidism can have a negative influence on renal function (Van Hoek & Daminet 2009). Hypothyroidism may lead to decreased protein synthesis and cellular development decreasing functional renal mass, density and size (Canavan et al. 1994; Slotkin et al. 1992). Alteration of renal function in humans (Den Hollander et al. 2005) and dogs (Gommeren et al. 2009) via direct and indirect effects has been well documented. The direct effects include intrarenal and peripheral vascular vasoconstriction (Singer 2001), decreased response to vasodilators in the kidney (Den Hollander et al. 2005) and decreased activity of the renin-angiotensin-aldosterone system (Asmah et al. 1997), all of which result in decreased renal blood flow. The indirect effects on renal function relate to decreased cardiac output (Katz, Emmanouel & Lindheimer 1975), leading to further decreased glomerular filtration rate (GFR) and increased serum creatinine (Capasso et al. 1999; Den Hollander et al. 2005). Hypothyroidism in dogs that have been shown to have reduced GFR is at least partially reversible by re-establishing euthyroidism (Gommeren et al. 2009). In hypothyroid dogs, improvement of renal function is observed with thyroxine supplementation, and a strong correlation between changes in thyroid status, serum creatinine concentration and GFR have been reported (Den Hollander et al. 2005; Gommeren et al. 2009). A recent study in cats demonstrated that hypothyroid cats had significantly higher plasma creatinine concentrations than euthyroid cats (Williams et al.2010). To the best of the authors' knowledge, renal insufficiency in feline congenital hypothyroidism has never been reported. It is believed that in this case the low thyroid concentration could have affected kidney development and function as a result of reduced GFR, with reduced metabolism and excretion of creatinine (Van Hoek & Daminet 2009). Interestingly, children with congenital hypothyroidism have reduced renal mass and a higher prevalence of renal and urologic abnormalities such as dysplastic kidneys (Kumar et al. 2009). Moreover, it is believed that the growth and a concomitant increase in muscle mass in the kitten led to an increase in creatinine production. This, together with inadequate restoration of euthyroidism by an inadequate dose of levothyroxine, caused mild renal azotaemia to persist until approximately 12 months of age. Subsequent increases in the doses of levothyroxine were accompanied by a steady rise in TT4concentrations with resultant reductions in the concentrations of TSH and the consequent establishment of euthyroidism. It is further postulated that the concomitant increment in USG, the reduction of serum creatinine and the normalisation of the UPC ratio from the time when euthyroidism was established support the assertion that inadequate establishment of euthyroidism played a role in the renal azotaemia in the patient. Although this could not be proven as no GFR evaluation was performed, it has been shown to occur in dogs and humans. In fact, a recent human study lends credence to the above argument as it demonstrated that children with acquired hypothyroidism had significantly lower GFR than normal children for up to 5 years after the start of thyroxine treatment and the restoration of euthyroidism (Elgadi et al. 2008). Further renal histopathology and GFR evaluation would have been indicated, but was unfortunately not performed. Renal histopathology would not have changed treatment decisions and the proteinuria normalised when euthyroidism was attained.
Cats with congenital hypothyroidism treated with levothyroxine should have a normal life expectancy as long as treatment is not stopped, but the long-term prognosis is unknown (Feldman & Nelson 2004; Szabo & Wells 2007) and is dependent on aetiology and age of initiation of treatment (Bojanicet al. 2011). The findings in this case indicate that early diagnosis and timing of treatment can reverse the typical clinical signs and improve skeletal development. An important finding in this case is that the dose of sodium levothyroxine needs to be in the range of 30 µg/kg bid in order to establish euthyroidism, which is much higher than the 10 µg/kg - 20 µg/kg bid recommended for dogs. An improvement in activity is expected within the first weeks of treatment and the remaining dermatological, cardiovascular and neurological signs should improve after weeks to months of treatment, as was seen in this case. At the time of reporting the cat's constipation, polyuria and polydipsia had completely resolved.
This is the first reported case of feline primary congenital hypothyroidism with concomitant renal insufficiency.
Acknowledgements
Competing interests
The authors declare that they have no financial or personal relationship(s) that may have inappropriately influenced them in writing this article.
Authors' contributions
C.K.L. (University of Pretoria) was the primary author and was responsible for the imaging interpretations, collaborating work of co-authors and writing the manuscript. C.T.R. (University of Pretoria) helped in medical interpretations and contributed intellectually to the manuscript preparation and in its writing. Y.d.W. (University of Pretoria) was the owner of the kitten as well as the primary veterinary nurse responsible for care, observation and diagnostic work-up of the kitten. J.P.S. (University of Pretoria) was the primary clinician responsible for diagnosis and follow-up of the case and contributed intellectually to the manuscript.
References
Arnold, U., Opizt, M., Grosser, I., Bader, R. & Eigenmann, J.E., 1984, 'Goitrous hypothyroidism and dwarfism in a kitten', Journal of the American Animal Hospital Association 20, 753-758. [ Links ]
Asmah, B.J., Wan Nazaimoon, W.M., Norazmi, K., Tan, T.T. & Khalid, B.A., 1997, 'Plasma renin and aldosterone in thyroid diseases', Hormone and Metabolic Research 29, 580-583. http://dx.doi.org/10.1055/s-2007-979105 [ Links ]
Bojanic, K., Acke, E. & Jones, B.R., 2011, 'Congenital hypothyroidism of dogs and cats: A review',New Zealand Veterinary Journal 59, 115-122. http://dx.doi.org/10.1080/00480169.2011.567964 [ Links ]
Braunlich, H., 1984, 'Postnatal development of kidney function in rats receiving thyroid hormones',Expert Clinical Endocrinology 83, 243-250. http://dx.doi.org/10.1055/s-0029-1210336 [ Links ]
Canavan, J.P., Holt, J., Easton, J., Smith, K. & Goldspink, D.F., 1994, 'Thyroid-induced changes in the growth of the liver, kidney, and diaphragm of neonatal rats', Journal of Cell Physiology 161, 49-54. http://dx.doi.org/10.1002/jcp.1041610107 [ Links ]
Capasso, G., De Tommaso, G., Pica, A., Anastasio, P., Capasso, J., Kinne, R. et al., 1999, 'Effects of thyroid hormones on heart and kidney functions', Mineral and Electrolyte Metabolism 25, 56-64. http://dx.doi.org/10.1159/000057421 [ Links ]
Crowe, A., 2004, 'Congenital hypothyroidism in a cat', Canadian Veterinary Journal 45, 168-170. [ Links ]
Den Hollander, J.G., Wulkan, R.W., Mantel, M.J. & Berghout, A., 2005, 'Correlation between severity of thyroid dysfunction and renal function', Clinical Endocrinology 62, 423-427. [ Links ]
Elgadi, A., Verbovszki, P., Marcus, C. & Berg, U.B., 2008, 'Long term effects of primary hypothyroidism on renal function in children', Journal of Pediatrics 152, 860-864. http://dx.doi.org/10.1016/j.jpeds.2007.10.050 [ Links ]
Feldman, E.C. & Nelson, R.W., 2004, 'Feline hypothyroidism', in E.C. Feldman & R.W. Nelson (eds.),Canine and Feline Endocrinology and Reproduction, 3rd edn., pp. 143-151, Saunders Elsevier, Philadelphia. [ Links ]
Gommeren, K., Van Hoek, I., Lefebvre, H.P., Benchekroun, G., Smets, P. & Daminet, S., 2009, 'Effect of thyroxine supplementation on glomerular filtration rate in hypothyroid dogs', Journal of Veterinary Internal Medicine 23, 844-849. http://dx.doi.org/10.1111/j.1939-1676.2009.0331.x [ Links ]
Greco, D.S., 2006, 'Diagnosis of congenital and adult-onset hypothyroidism in cats', Clinical Techniques in Small Animal Practice 21, 40-44. http://dx.doi.org/10.1053/j.ctsap.2005.12.007 [ Links ]
Gunn-Moore, D., 2005, 'Feline endocrinopathies', Veterinary Clinics of North America Small Animal Practice 35, 171-210. http://dx.doi.org/10.1016/j.cvsm.2004.09.002 [ Links ]
Johnson, K.A. & Watson, A.D.J., 2010, 'Skeletal diseases', in S.J. Ettinger & E.C. Feldman (eds.),Textbook of veterinary internal medicine, 7th edn., vol. I, pp. 819-845, Saunders Elsevier. [ Links ]
Jones, B.R., Gruffydd-Jones, T.J., Sparkes, A.H. & Lucke, V.M., 1992, 'Preliminary studies on congenital hypothyroidism in a family of Abyssinian cats', Veterinary Record 131, 145-148. http://dx.doi.org/10.1136/vr.131.7.145 [ Links ]
Katz, A.I., Emmanouel, D.S. & Lindheimer, M.D., 1975, 'Thyroid hormone and the kidney', Nephron15, 223-249. http://dx.doi.org/10.1159/000180514 [ Links ]
Kumar, J., Gordillo, R., Kaskel, F.J., Druschel, C.M. & Woroniecki, R.P., 2009, 'Increased prevalence of renal and urinary tract anomalies in children with congenital hypothyroidism', Journal of Pediatrics154, 263-266. http://dx.doi.org/10.1016/j.jpeds.2008.08.023 [ Links ]
Mariani, L.H. & Berns, J.S., 2012, 'The renal manifestations of thyroid disease', Journal of the American Society of Nephrology , 23, 22-26. http://dx.doi.org/10.1681/ASN.2010070766 [ Links ]
Mooney, C.T. & Anderson, T.J., 1993, 'Congenital hypothyroidism in a boxer dog', Journal of Small Animal Practice 34, 31-35. http://dx.doi.org/10.1111/j.1748-5827.1993.tb02573.x [ Links ]
Pettigrew, R., Fyfe, J.C., Gregory, B.L., Lipsitz, D., DeLahunta, A., Summers, B.A. et al., 2007, 'CNS hypomyelination in rat terrier dogs with congenital goiter and a mutation in the thyroid peroxidase gene', Veterinary Pathology 44, 50-56. http://dx.doi.org/10.1354/vp.44-1-50 [ Links ]
Quante, S., Fracassi, F., Gorgas, D., Kircher, P.R., Boretti, F.S., Ohlerth, S. et al., 2010, 'Congenital hypothyroidism in a kitten resulting in decreased IGF-1 concentration and abnormal liver function tests', Journal of Feline Medicine and Surgery 12, 487-490. http://dx.doi.org/10.1016/j.jfms.2010.01.013 [ Links ]
Saunders, H.M. & Jezyk, P.K., 1991, 'The radiographic appearance of canine congenital hypothyroidism: Skeletal changes with delayed treatment', Veterinary Radiology 32, 171-177. http://dx.doi.org/10.1111/j.1740-8261.1991.tb00103.x [ Links ]
Scott-Moncrieff, J.C., 2007, 'Clinical signs and current diseases of hypothyroidism in dogs and cats',Veterinary Clinics of North America Small Animal Practice 37, 709-722. http://dx.doi.org/10.1016/j.cvsm.2007.03.003 [ Links ]
Singer, M.A., 2001, 'Of mice and men and elephants: Metabolic rate sets glomerular filtration rate',American Journal of Kidney Diseases 37, 164-178. http://dx.doi.org/10.1016/S0272-6386(01)80073-1 [ Links ]
Sjollema, B.E., Den Hartog, M.T., De Vijlder, J.J.M., Van Dijk, J.E. & Rijnberk, A., 1991, 'Congenital hypothyroidism in two cats due to defective organification: Data suggesting loosely anchored thyroperoxidase', Acta Endocrinologica (Copenhagen) 125, 435-440. [ Links ]
Slotkin, T.A., Seidler, F.J., Kavlock, R.J. & Bartolome, J.V., 1992, 'Thyroid hormone differentially regulates cellular development in neonatal rat heart and kidney', Teratology 45, 303-312. http://dx.doi.org/10.1002/tera.1420450309 [ Links ]
Stephan, I. & Schutt-Mast, I., 1995, 'Kongenitale Hypothyreose mit disproportioniertem Zwergwuchs bei einer Katze' [Congenital hypothyroidism with disproportional dwarfism in a cat], Kleintierpraxis40, 701-706.
Szabo, S.D. & Wells, K.L., 2007, 'What is your diagnosis?', Journal of the American Veterinary Medical Association 230, 29-30. http://dx.doi.org/10.2460/javma.230.1.29 [ Links ]
Tanase, H., Kudo, K. & Horikoshi, H., 1991, 'Inherited primary hypothyroidism with thyrotrophin resistance in Japanese cats', Journal of Endocrinology 129, 245-241. http://dx.doi.org/10.1677/joe.0.1290245 [ Links ]
Tobias, S. & Labato, M.A., 2001, 'Identifying and managing feline congenital hypothyroidism',Veterinary Medicine 96, 719-721. [ Links ]
Traas, A.M., Abbott, B.L., French, A. & Giger, U., 2008, 'Congenital thyroid hypoplasia and seizures in 2 littermate kittens', Journal of Veterinary Internal Medicine 22, 1427-1431. http://dx.doi.org/10.1111/j.1939-1676.2008.0203. [ Links ]
Van Hoek, I. & Daminet, S., 2009, 'Interactions between thyroid and kidney function in pathological conditions of this organ systems: A review', General and Comparative Endocrinology 160, 205-215. http://dx.doi.org/10.1016/j.ygcen.2008.12.008 [ Links ]
Williams, T.L., Elliott, J. & Syme, H.M., 2010, 'Association of iatrogenic hypothyroidism with azotemia and reduced survival time in cats treated for hyperthyroidism', Journal of Veterinary Internal Medicine 24, 1086-1092. http://dx.doi.org/10.1111/j.1939-1676.2010.0566.x [ Links ]
 Correspondence:
Correspondence:
Chee Kin Lim
Private Bag X04
Onderstepoort 0110
South Africa
Email: lim152@purdue.edu
Received: 29 Nov. 2013
Accepted: 19 Aug. 2014
Published: 14 Nov. 2014


{kind=link}
{kind=link}