










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkJournal of the South African Veterinary Association
On-line version ISSN 2224-9435
Print version ISSN 1019-9128
J. S. Afr. Vet. Assoc. vol.83 n.1 Pretoria Jan. 2012
CASE REPORT
Immunohistochemical study of a canine neurofibroma
Hamidreza FattahianI; Pejman MortazaviII; Hamidreza MoosavianIII; Hamid MohyeddinIV; Roozbeh MoridpourI
IDepartment of Surgery, Science and Research Branch, Islamic Azad University, Iran
IIDepartment of Pathology, Science and Research Branch, Islamic Azad University, Iran
IIIDepartment of Clinical Sciences, University of Tehran, Iran
IVDepartment of Clinical Sciences, Garmsar Branch, Islamic Azad University, Iran
ABSTRACT
Accurate diagnostic approaches to differentiate peripheral nerve sheet tumours from others have not been firmly established. The aim of this case report was to diagnose neurofibroma using a combination of diagnostic imaging, histopathology and immunohistochemistry, which were applied to a canine neurofibroma arising in the left mandible. The tumour was surgically excised and examined histologically. Round or spindle cells, with elongated, dense and homogenous chromatin and pale cytoplasm typical of Schwann cells in an abundant fibromyxomatous stroma, with ruby collagen fibres were seen. Immunohistochemistry demonstrated that S-100 and vimentin were more than 70% positive. Neurofibroma may therefore be recognisable using markers such as S-100 and vimentin.
Introduction
In humans, neurofibroma and schwannoma are distinct entities within the group of benign peripheral nerve sheath tumours (PNST)1 and the definitive diagnosis of PNST as a schwannoma or a neurofibroma is one of the important factors for patient management and prognosis.1,2 Differential diagnosis of these tumours can be made using histopathological features and additional diagnostic criteria such as immunohistochemistry and electron microscopy.2 Research focused on canine tumours has revealed naturally occurring PNST in different organs such as the nose, neck, periorbital area, flank, colon, zygomatic arch, tongue, kidney and hindlimbs.1,3,4 Distinct criteria for classification of benign PNST such as schwannoma or neurofibroma have not been agreed upon in the veterinary literature.5 This is probably because of low incidence of PNST and therefore a lack of studies about these in animals.2 The aim of the present clinical study was therefore to develop a complete profile of this tumour by performing clinical and paraclinical examinations.
Case history
A 4-year-old, 4 kg, female terrier breed dog was referred to a private clinic with anorexia, intermittent retching, general weakness and asymmetry of the neck caused by a subcutaneous mass on the left side of the neck (Figure 1).

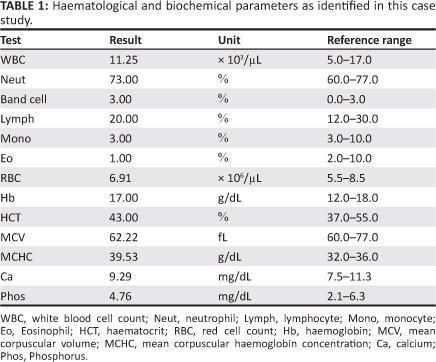
The blood cell count was undertaken manually and calcium and phosphorus concentration were measured by commercial kits (Pars Azmoon, Alborz, Iran) using a semi-automatic analyser (EMP 168 Vet Biochemical analyser; Shenzhen Emperor Electronic technology Co. Ltd, Shenzhen, China). Haematological and biochemical profiles (including blood cell count and serum calcium and phosphorus concentrations) were within normal ranges (Table 1).
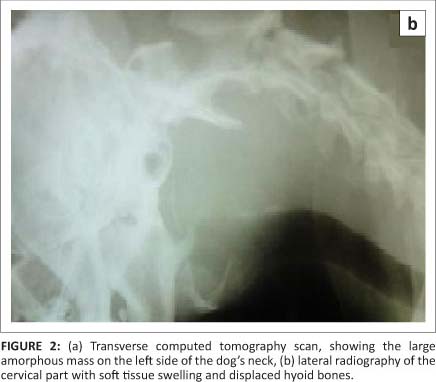
Diagnostic imaging was conducted using ultrasonography (portable linear scanning ultrasound system SIUI CTS-485V; Shantou Institute, Shantou, China), computed tomography (CT) (Figure 2a) (SOMATOM plus S; Siemens, Erlangen, Germany) and radiography (Figure 2b). The appearance of the mass was amorphous to ovoid with a distinguishable margin and hyperdense focal deposition of mineral in the central area (Figure 2a). This mass appeared to displace the transverse process of the 3rd cervical vertebrae dorsally. Its mass also displaced the hyoid apparatus, as seen in lateral radiography (Figure 2b), with a soft tissue opacity that measured approximately 8.70 cm x 6.18 cm by ultrasonography. There were numerous anechoic foci creating both distal acoustic enhancement and edge shadow artifacts beneath them. The frequency of ultrasound used in this study was 8 MHz.

Anaesthesia for partial excisional biopsy was induced with an intravenous line and the dog received normal saline solution 0.9% intravenously, to a total of 0.5 L (12 mL/kg/h) (Samen, Mashhad, Iran). Atropine sulphate (0.03 mg/kg) (Tamin, Tehran, Iran) was given subcutaneously as pre-medication. An intravenous combination of diazepam (0.27 mg/kg) (Tamin, Tehran, Iran) and ketamine hydrochloride (5.50 mg/kg) (Alfasan, Woerden, the Netherlands) were used for induction and maintenance of anaesthesia. The sample was fixed in formalin and embedded in paraffin for sectioning. The sections were stained with haematoxylin and eosin. For further study, paraffin sections were stained immunohistochemically with S-100, vimentine, cytokeratin and desmin markers (Abcam Co., Cambridge, USA).
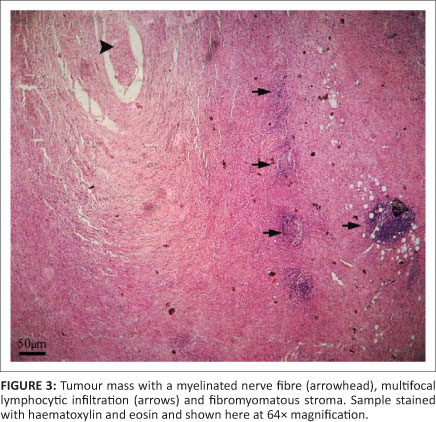
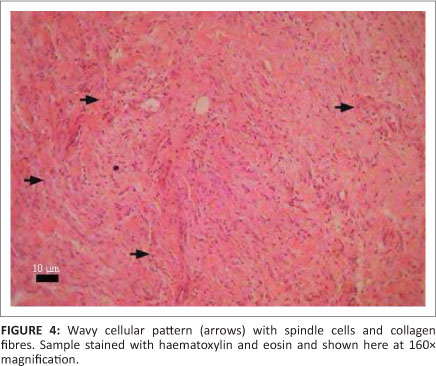
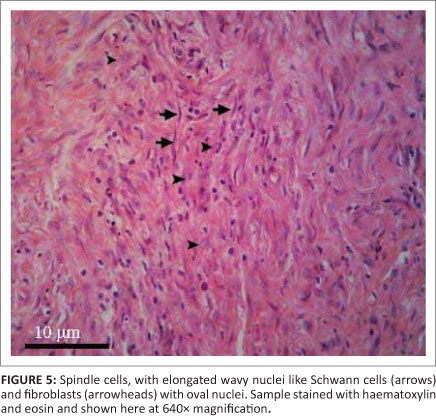
Histopathological examination showed isolated round or spindle cells, with elongated, often angulated and wavy nuclei, dense and homogenous chromatin, pale cytoplasm (Schwann cells), in an abundant fibromyxomatous with ruby collagen fibres, and few fibroblasts with oval nuclei. The mitotic rate was very low, with less than one mitotic figure per five 40x fields. The tumour had a variable cellular density. Mild multifocal lymphocytic infiltration was observed in the tumour. Pieces of myelinated axon nerve fibres were seen within the tumour mass (Figures 3-5). The demonstration of axons within the tumour was important in distinguishing neurofibroma from schwannoma.6
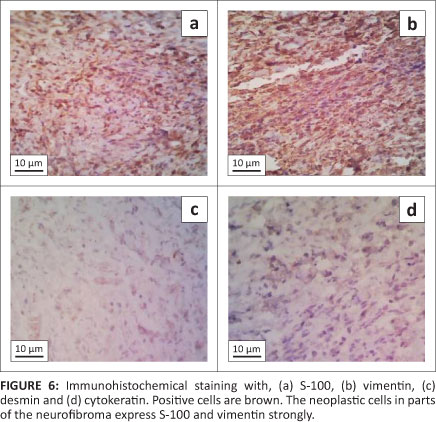
Using immunohistochemical staining, more than 80% of cells were positive for S-100, about 70% of cells were positive for vimentin, 30% for cytokeratin and 10% for desmin (Figure 6). A localised cellular neurofibroma was demonstrated on the basis of histopathology and immunohistochemistry.
Based on these results and at the owner's request, excisional surgery was performed. Anaesthesia was induced with an intravenous line and the dog received normal saline solution 0.9% at 12 mL/kg/h. Prophylactic antibiotics were administrated intravenously using cefazolin (20 mg/kg) (Jaber-ebne-hayyan, Tehran, Iran) 0.5 h before anaesthetic induction. Premedication, induction and maintenance of anaesthesia were as described previously for the partial excision biopsy. The dog was intubated with an orotracheal tube. Heart rate and partial oxygen pressure were monitored by pulsoximeter (Medair, Stockholm, Sweden), the dog was then positioned in a right lateral recumbency and the surgical area prepared aseptically. A 15 cm incision of the skin was made 2 cm ventral to the vertebral column (distal to the transverse process of the atlas) to the ventral aspect of the neck. Blunt dissection was made bilaterally for access to the medial wall of mass where it came into contact with cervical structures. Trauma to the vital structures (linguofacial vein, nerves, oesophagus, trachea and carotid artery) was avoided. The superficial vessels were ligated and smaller vessels were electrocauterised (Avanteb, Tehran, Iran). After complete undermining of the mass, avoiding trauma to the nerves, vessels, oesophagus and trachea, the mass was excised. The closure of the wound was undertaken in two layers using 3-0 polygalctin 910 (Supalon; Supa, Alborz, Iran) for the subcutaneous tissues and 4-0 nylon (Supalon; Supa, Alborz, Iran) for the skin, respectively. A passive drain (penrose drain; 4A Medical, Ankara, Turkey) was inserted into the surgical site through a stab incision (2 cm) ventrally and secured using two simple interrupted sutures using 4-0 nylon (Supalon; Supa, Alborz, Iran). The skin incision was bandaged to prevent self-mutilation and contamination for two weeks and changed every other day. Tramadol (Alborzdaru, Ghazvin, Iran) as analgesic was injected subcutaneously (2 mg/kg). The tumour mass was preserved in 10% buffered formalin and submitted to the pathology laboratory. Neurofibroma was reconfirmed using immunohistochemistry. Antibiotic therapy was continued intramuscularly using injectable penicillin (20 000 IU/kg) (Jaber-ebne-hayyan, Tehran, Iran) and gentamicin sulphate (8 mg/kg) (Exir, Tehran, Iran) for three days, routinely.
Discussion
This report is a study of a spontaneous PNST that confirms the existenceof acanine neurofibroma. In thiscase,haematological, biochemical, radiographic, CT scan, histopathological and immunohistochemical studies were conducted. The CT scan showed that that tumour centre had calcified, which is not unusual in benign tumours. The presence of intramural calcification may even be an indicator of neoplasia in some tumours such as mucinous tumours.6 Calcification has not been reported previously in canine neurofibroma.7 Elevated calcium levels in serum have been detected in the presence of paraneoplastic syndromes.3,7 Paraneoplastic syndromes are common concomitants of certain neoplastic diseases. Two of the main signs of paraneoplastic syndrome are cachexia and hypercalcemia,8 but we did not see cachexia in this case and the total calcium level was normal. Histopathology and immunohistochemistry are the most important techniques for differentiation of PNST in human and animal medicine.
Conclusion
The tumour in this study was diagnosed as a neurofibroma based on its histopathological and immunohistochemical features. The pathognomonic finding was the presence of nerve fibres within the tumour, as well as the neoplastic cells. Benign PNST must be differentiated from malignant PNST. Based on the low mitotic index and low number of poorly differentiated neoplastic cells, the tumour in this case study was identified positively as a neurofibroma.
Acknowledgements
Competing interests
The authors declare that they have no financial or personal relationships which may have inappropriately influenced them in writing this paper.
Authors' contributions
H.R.F. (Islamic Azad University) was the surgeon who performed the study and who also wrote the manuscript.
P.M. (Islamic Azad University) was responsible for the histopathologic analysis, whilst H.R.M. (University of Tehran) performed the laboratory test as biochemical and haematologic studies, H.M. (Islamic Azad University) performed diagnostic imaging process and R.M. (Islamic Azad University) assisted in the surgery and co-authored the manuscript.
References
1. Schoniger S, Summwers BA. Localized, plexiform, diffuse, and other variants of neurofibroma in 12 dogs, 2 horses and a chicken. Vet Path. 2009;46:904-915. http://dx.doi.org/10.1354/vp.08-VP-0322-S-FL, PMid:19429995 [ Links ]
2. Koestner A, Higgins RJ. Tumors of the nervous system. In: Meuten DJ, editor. Tumors in domestic animals. 4th ed. Ames, Iowa State University Press, 2002; p. 697-738. http://dx.doi.org/10.1002/9780470376928.ch14 [ Links ]
3. Brower A, Salamat S, Crawford L, Manley P. Unilateral limb enlargement in a dog with a malignant peripheral nerve sheath tumor. Vet Path. 2005;42:353-356. http://dx.doi.org/10.1354/vp.42-3-353, PMid:15872382 [ Links ]
4. Zwicker GM, Cronin NS. Naturally occurring renal neurofibroma in a laboratory beagle. J Toxicol Path. 1992;20:112-114. http://dx.doi.org/10.1177/019262339202000113, PMid:1384104 [ Links ]
5. Goldschmidt MH, Hendrick MJ. Tumors of the skin and soft tissues. In: Meuten DJ, editor. Tumors in domestic animals. 4th ed. Ames: Iowa State University Press, 2002; p. 45-118. http://dx.doi.org/10.1002/9780470376928.ch2 [ Links ]
6. Summers BA, Cummings JF, Lahunta A. Veterinary neuropathology. St. Louis: Mosby Year Book Inc.; 1995. [ Links ]
7. Okada S, Ohaki Y, Inoue K, et al. Calcification in mucinous and serous cystic ovarian tumors. J Nippon Med Sch. 2005;72:29-33. http://dx.doi.org/10.1272/jnms.72.29 [ Links ]
8. Yoneda T, Alsina MA, Chavez JB, Bonewald L, Nishimura R, Mundy GR. Evidence that tumor necrosis factor plays a pathogenetic role in the paraneoplastic syndromes of cachexia, hypercalcemia, and leukocytosis in a human tumor in nude mice. J Clin Invest. 1991;87:977-985. http://dx.doi.org/10.1172/JCI115106, PMid:1999505, PMCid:329890 [ Links ]
 Correspondence to:
Correspondence to:
Hamidreza Fattahian
No. 10, Second Alley
North Falamak
Shahrake Gharb, Tehran, Iran
hrfattahian@srbiau.ac.ir
Received: 04 Aug. 2011
Accepted: 16 Mar. 2012
Published: 07 Aug. 2012

