










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkJournal of the South African Veterinary Association
On-line version ISSN 2224-9435
Print version ISSN 1019-9128
J. S. Afr. Vet. Assoc. vol.81 n.2 Pretoria Jan. 2010
CLINICAL COMMUNICATION KLINIESE MEDEDELING
Oesophageal obstruction in Dorper ewes caused by impaction of a pelleted ration
R Anderson*; G F Bath; P N Thompson; M M Stadler
Department of Production Animal Studies, Faculty of Veterinary Science, Private Bag X04, Onderstepoort, 0010, South Africa
ABSTRACT
Two adult Dorper ewes developed an oesophageal obstruction (choke) by consuming a pelleted ration. The history, clinical signs and method of treatment were recorded in each case. One case was treated surgically via rumenotomy and the other conservatively. Both ewes recovered uneventfully and no recurrence was observed. Reasons for the compaction of the pelleted ration in the oesophagus are discussed.
Keywords: choke, oesophageal impaction, ovine, pelleted ration, sheep.
INTRODUCTION
According to several authorities1-10 oesophageal obstruction, also known as choke, is a fairly common occurrence in cattle but there are very few references to the condition in sheep. This report focuses on 2 cases presented from the same farm; 1 case was resolved surgically while the other was treated conservatively.
CASE HISTORIES
The sheep flock consisted of both commercial and stud Dorper sections. The sheep were fed a pelleted ration and lucerne hay in old tractor tyres turned inside out that served as feed troughs. The farmer had noticed that some of the lambs would eat greedily and then step away from the troughs and cough, often spitting out small amounts of the pelleted ration. Lambs that continued to cough were dosed with water into the oesophagus using a dosing syringe, and the lambs would stop coughing. After a coughing bout the farmer observed that the lambs would eat less greedily.
A case of choke had occurred in an adult ewe approximately 2 years previously with no further occurrence in adults until the 2 cases presented below, which occurred within a week of each other. These were the only 2 cases out of 200 ewes in recent times on the farm. The affected ewes were both full mouth ewes, the older being 7 years of age.
The coughing up of pelleted ration started from 3 months of age and affected any age group. The farmer observed that coughing up of the pelleted ration occurred more frequently just before spring.
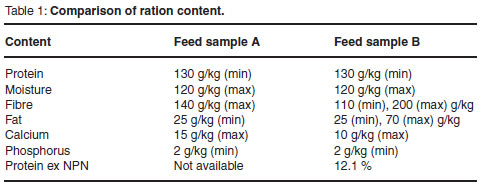
The pelleted ration was purchased from a feed manufacturer who had bought a new machine which produced bigger pellets. In Fig. 1 the usual pelleted ration (A) is 5 mm in diameter whereas the new pelleted ration (B) is 7 mm in diameter. Lengths of the pelleted ration varied in both samples A and B and the farmer suspected that the coughing would occur if 1 (or more) of the pellets became lodged across the oesophagus.
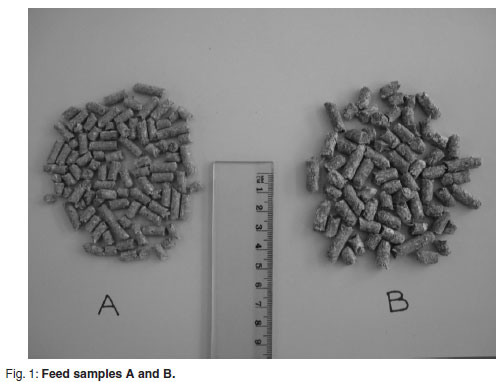
The ration content according to the manufacturer's label is recorded in Table 1. Individual ingredients in the feeds are unavailable. The major difference between the 2 feeds, according to Table 1, is the fibre content. It was noted that feed sample B smelled very strongly of lucerne. Feed was put out for the animals at regular intervals throughout the day to encourage the sheep to consume more feed in the hope that they would grow faster for show purposes.
Case 1: Surgical treatment
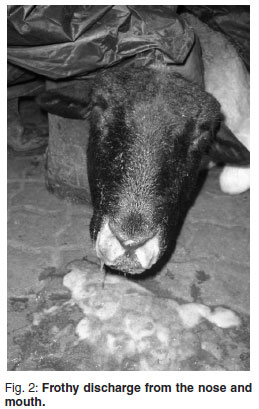
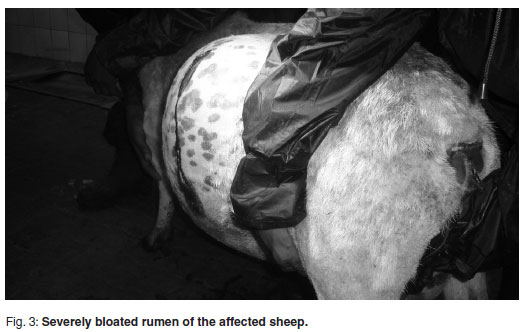
An 8-tooth Dorper ewe (weight estimated to be 65 kg) was presented with a history of consuming a large amount of a pelleted ration which led to an acute, severe bloat (Fig. 3.) and respiratory distress. The ewe was 1 to 2 weeks post partum with triplet lambs. There was a frothy green discharge from the nose and mouth (Fig. 2.). The owner had already tried to deflate the rumen by inserting large gauge needles into it. Introduction of a stomach tube confirmed a complete obstruction in the thoracic cavity cranial to the cardiac sphincter. When removed, there was impacted food (apparently the pelleted ration) present in the end of the stomach tube.
As the abdomen was severely distended, it was decided that using a general anaesthetic or sedative would lead to severe respiratory distress and possibly death. The ewe was therefore restrained in a standing position to avoid excess pressure on the abdomen and the left paralumbar fossa was surgically prepared.
Local anaesthetic was administered (Lignocaine HCl 2 %, Centaur, Bayer AH) using an inverted L block, and a rumenotomy was performed. The rumen was filled with hay to a level dorsal to the cardiac sphincter. On removal of most of the rumen contents the rumen wall was assessed as healthy. A finger was inserted into the cardiac sphincter cranially and a dry, hard mass was palpated in the oesophagus. A 5-mm-diameter stomach tube was inserted caudal to the obstruction and lukewarm running water used to soften the impaction. As the feed loosened, the tube was advanced until a large amount of feed moved into the rumen. A stomach tube was inserted orally and passed through into the rumen. The rumen and subcutaneous tissue was sutured with chromic surgical catgut (Ethicon®, Johnson & Johnson) and the skin sutured with Ethilon blue monofilament polyamide 6 (Ethicon®, Johnson & Johnson).
Post-operatively the ewe was given florfenicol 300 mg/m (Nuflor, Schering-Plough AH) at a dosage rate of 1 mℓ per 15 kg, 60 m propylene glycol 15 % and 5mℓ hyoscine-n-butylbromide 4 mg, dipyrone 500 mg/mℓ (Buscopan Compositum, Janssen). The ewe was able to stand immediately post-operatively and suckled her lambs when put into the vehicle to be taken back to the farm. No recurrence was reported.
Case 2: Non-surgical treatment
An 8-tooth Dorper ewe weighing 70 kg was presented with severe bloat 1 week after the previous case. The owner had already given the ewe hyoscine-n-butylbromide 4 mg, dipyrone 500 mg/mℓ (Buscopan Compositum, Janssen) and deflated the rumen twice with 15 gauge needles. The ewe swallowed often and a mixture of mucus and feed discharged from the nose and mouth. The ewe's breathing was shallow. A stomach tube was passed orally into the oesophagus and a complete obstruction felt cranial to the thoracic inlet. It was noted that the ewe became distressed upon tubing. It was decided to dislodge the obstruction orally under sedation.
The ewe was sedated with ketamine base 100 mg (hydrochloride form), benzethonium chloride 0.01 % m/v (Anaket-V, Centaur Labs) and diazepam 10mg, alcohol 5.8 % v/v, benzyl alcohol 1.5 % v/v (Transject 10 mg, Merck Generics) intravenously and was placed in right lateral recumbency with the head hanging over the edge of the operating table. A stomach tube was passed orally and a large dosing syringe was used to flush the oesophagus with warm water whilst gently moving the tube backwards and forwards. Small amounts of the pelletted feed were flushed out at a time. The obstruction extended to the cardia of the rumen and after approximately 15 minutes the tube passed into the rumen. The ewe was given florfenicol 300 mg/m (Nuflor, Schering-Plough AH) at 1 m per 15 kg to protect against aspiration pneumonia and was put into a pen where she immediately began to eat lucerne hay, swallowing without difficulty. The condition did not recur.
DISCUSSION
Cattle are more frequently affected by oesophageal obstruction than sheep9 or goats.4,10 This is assumed to be at least partly because of the method of feeding.
Cattle have relatively insensitive tongues and are known to ingest foreign objects like wire, giving rise to 'hardware disease' or traumatic reticulo-peritonitis. They are also more likely to swallow large food masses such as apples and potatoes that can readily obstruct the oesophagus. By contrast, this is seldom seen or reported in either sheep or goats, presumably because they are more fastidious feeders. There is also no published reference to oesophageal obstruction in small ruminants resulting from impaction by a milled feed either in pelleted or loose form.
Since this form of choke is very rare (and apparently not previously reported in small ruminants), some consideration of the possible contributory factors is needed.
Contributory factors include:
1. Type of ration. It is possible that either the physical structure or the ingredients were prone to compact into dense concretions.
2. Palatability of the feed. Excessive intakes over a short time may have played a role. It was observed that feed sample B in Fig. 1 smelled strongly of fresh lucerne which may have been more appealing to the sheep than feed sample A.
3. Competition for feed. This could have been a factor if sufficient trough space for all animals was allowed which could have resulted in very rapid consumption by more greedier feeders.
4. Genetic factors. Dorpers are bred for fast growth and this, together with feeding management on this particular farm, requires an ability and inclination for rapid feeding and high intakes.
5. Lack of sufficient trough space. This may cause dominant individuals to overeat although at a slower pace.
6. Production or nutritional demands. Both weaners with rapid growth and lactating ewes (especially those with multiple lambs) were affected. Although all sheep were prone to coughing out pelleted ration occasionally, it appeared that the weaners were mostly affected.
7. Excessive rumen fill. Ingestion of large quantities of hay prior to ingestion of pelleted ration could fill the rumen dorsal to the level of the cardiac sphincter. Thus when the pelleted ration was consumed it was unable to pass into the rumen and so compacted in the oesophagus.
8. Feed trough height. Upon closer observation of the lambs' feeding behaviour, the farmer noticed that the feed trough was too high for the lambs and that the edge of the feed troughs was placing pressure on the necks of the smaller sheep. This could explain why the younger animals were observed coughing out small amounts of feed as the oesophagus was partially obstructed by the pressure of the feeding troughs on the neck, possibly leading to a build up of pelleted ration in the oesophagus. The farmer put shallower feeding troughs in the lambs' camps and the problem seemed to be resolved for the lambs. However, this does not explain the complete obstruction in the adult ewes.
9. Time of year. These cases were observed to occur throughout the year but more so just before spring. It could be that the sheep were inclined to ingest more at this time of year as well as eat more greedily due to higher production demands.
10. Ability of the sheep to ruminate effectively. This as well as rumination time allowed before being given the pelleted ration could play a role. Sheep with worn teeth cannot ruminate effectively thereby creating a relatively larger 'raft' layer in the rumen leading to rumen overfill. This could provide the initial obstruction of the passage of the pelleted ration into the rumen.
Since the occurrence of oesophageal impaction of pelleted feed is apparently rare, the diagnosis may present some problems. The presenting clinical sign is bloat, and both frothy and free gas forms would need primary consideration. Other causes of acute abdominal enlargement would need to be considered, but failing to pass a stomach tube would isolate obstructive free gas bloat as the likeliest cause. Where obstructive bloat is diagnosed, pelleted ration should be considered as a possible cause and in such cases both surgical and non-surgical treatment results in successful removal of the obstruction. The value of the animal and the severity of the choke will determine which treatment option is the best for each case.
REFERENCES
1. Aitkin I D 2007 Diseases of sheep (4th edn). Blackwell, Oxford [ Links ]
2. Bath G F, de WetJ2001 Sheep and goat diseases. Tafelberg, Cape Town [ Links ]
3. Brightling A 1988 Sheep diseases. Inkata Press, Melbourne [ Links ]
4. Baxendell S A 1987 The diagnosis of the diseases of goats. University of Sydney Post Graduate Foundation in Veterinary Science, Sydney [ Links ]
5. Fraser A, Stamp J T 1987 Sheep husbandry and diseases (6th edn). Collins, London [ Links ]
6. Kimberling C V 1988 Jensen and Swift's diseases of sheep. Lea and Febiger, Philadelphia [ Links ]
7. Hindson J C, Winter A C 1990 Outline of clinical diagnosis in sheep. Wright, London [ Links ]
8. Plant J 1992 Diagnosis of diseases of sheep. University of Sydney Post Graduate Foundation in veterinary Science, Sydney [ Links ]
9. Radostits O M, Gay C C, Blood D C, Hinchcliff K W 2000 Veterinary medicine. A textbook of the diseases of cattle, sheep, pigs, goats and horses (9th edn). W B Saunders, London [ Links ]
10. Sherman D M, Smith M C Goat medicine. Lea and Febiger, Philadelphia [ Links ]
Received: November 2009.
Accepted: March 2010.
* Author for correspondence. E-mail: rhoda.anderson@up.ac.za

