










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkStudia Historiae Ecclesiasticae
versão On-line ISSN 2412-4265
versão impressa ISSN 1017-0499
Studia Hist. Ecc. vol.44 no.3 Pretoria 2018
http://dx.doi.org/10.25159/2412-4265/4701
ARTICLE
The rise, fall and re-establishment of Trinity Health Services: Oral history of a student-run clinic based at an inner-city Catholic Church
Deanne JohnstonI; Anthony EganII; Patricia McInerneyIII
IUniversity of the Witwatersrand deanne.johnston@wits.ac.za, https://orcid.org/0000-0001-6431-2140
IIUniversity of the Witwatersrand Jesuit Institute South Africa a.egan@jesuitinstitute.org.za, https://orcid.org/0000-0002-4191-4701
IIIUniversity of the Witwatersrand Patricia.McInerney@wits.ac.za, https://orcid.org/0000-0002-1011-8032
ABSTRACT
The Catholic Church played a significant role in healthcare within South Africa through the establishment of 73 hospitals by the 1950s. However, the majority of these had been taken over by the state by 1970. Trinity Health Services (THS), a student-run clinic providing free healthcare to the homeless and operating from a Catholic Church in Johannesburg, proposes a new model for involvement of the church (and by extension the wider religious community) in healthcare. This oral history describes the story of THS, a joint partnership between Holy Trinity Catholic Church and the University of the Witwatersrand. It defines the stakeholders, namely the students, the Faculty of Health Sciences at the University of the Witwatersrand, and Holy Trinity Catholic Church, and explains their contributions to the clinic. The clinic was established in 2004 by two medical students and soon expanded its services, therefore needing more space and resources, including a pharmacy. The clinic was closed from 2011-2015 while registering the pharmacy. It reopened in February 2016, offering medical and pharmaceutical services. Convergent and divergent themes are described between the history of THS and more traditional Catholic healthcare. Similarities are drawn between the communities they serve, their approach to healthcare, and legislative challenges faced. The differences relate to the involvement of both secular and religious people in THS who are motivated to serve for humanitarian reasons, compared to religious sisters who were serving as part of their mission. THS shows the importance of healthcare projects with religious links. This new paradigm calls for the involvement of multiple partners, involving both religious and secular entities, in providing much needed services to underserved communities within society.
Keywords: Catholic healthcare; student-run clinics; social justice; Trinity Health Services (THS)
Introduction
History shows the interconnectedness between religions, medicine and healthcare. Koenig et al. (2012, 24-49) outline historical events indicating the links of Buddhism, Christianity, Hinduism, Islam and Judaism to healthcare.
Health, healing and wellbeing are constitutive elements in religious traditions. While a narrowly defined "magical" understanding of religious healing (i.e. faith healing) is inadmissible in modern medicine (as indeed it was for Catholic sisters who founded hospitals and clinics in South Africa during the 19th and 20th centuries), modern medicine acknowledges a holistic understanding of medicine. The bio-psychosocial model of healthcare that is the gold standard of pedagogy in South African medical faculties (including the University of the Witwatersrand) is much closer to an understanding of the healing that the Catholic sisters brought.
Traditional hospital-based models of Catholic healthcare, we shall suggest, are no longer viable. The time for religious sisters working as nurses has passed; there are no longer vocations and many of these orders are in rapid numerical decline. Nor can the Catholic Church afford to operate hospitals run entirely by lay staff. There has been a shift to greater professionalisation of healthcare and the need to comply with legislation. Most of the remaining religious sisters with medical training have moved into home-based healthcare. The decline in vocations means they will not be replaced.
In stark contrast to religious vocations, homelessness has increased in South Africa. Homeless people in South Africa are most in need of food, water, sanitation and housing. They face several challenges when accessing healthcare, for example inability to provide identification documents and/or proof of residence (Wentzel and Voce 2012, 84). Holy Trinity Catholic Church in Braamfontein provides a daily soup kitchen for feeding the homeless. The church is seen as their place of refuge where they form a community.
Student-run clinics (SRCs) are spaces where healthcare students under the supervision of qualified professionals take the lead in providing healthcare services to underserved communities. There are five SRCs associated with Medical Schools in South Africa (Gordon 2016, 21). The Students' Health and Welfare Centres Organisation of the University of Cape Town, established in 1942, is perhaps the most well-known SRC and consists of mobile healthcare services which travel to communities in need (Favara and Mendelsohn 2012, 401402).
The subject of this article is an inner-city clinic, based at Holy Trinity Catholic Church, serving the homeless. It proposes a new paradigm for the involvement of a religious organisation in healthcare and to our knowledge it is the only such clinic in South Africa. This is a story which needs to be told as it illustrates religion and medical science working together, pointing to a new direction for the churches' involvement in healthcare in an era where the older paradigms are no longer possible.
Catholic Healthcare in South Africa
To contextualise our story and to substantiate our claims, it is necessary to review the role of Catholicism in healthcare within South Africa. Catholicism established itself in South Africa from 1818 onwards, after the British had occupied the Cape in 1806. This opened the door for missionaries who were initially sent to educate communities as a way of spreading the faith. However, the missionaries found a clear need for healthcare. In the 19th century Bishop Jolivet saw the opportunity to expand into social work and healthcare in Natal, but needed to gain the confidence of the Zulus who stayed within their tribes and believed in traditional medicine (Brain 1982, 86). Over time, people migrated inland as they found opportunities in mining. Soon there was a need for hospitals, as frequent disease outbreaks occurred due to poor living conditions and inadequate sanitation, as well as an increasing number of mining injuries (Brain 1991, 89-90).
Faced with this need there was a rapid increase in Catholic hospitals, totalling 73 by 1950 (CATHCA 2011, 117). Care in these hospitals was provided regardless of race and religion. The religious nurses believed that all people were entitled to quality services and strived to uphold high standards in the hospitals they founded. They opposed apartheid government policies such as prohibiting "white" nurses from treating "black" patients (Brain 1991, 91).
The Johannesburg General Hospital (later renamed the Charlotte Maxeke Johannesburg Academic Hospital [CMJAH]) had an initial close relationship with Catholic religious sisters. Brain (1991, 86-92) describes the involvement of the sisters of the Holy Family of Bordeaux in the establishment of the Johannesburg General Hospital. In 1888 the sisters started to work in the temporary hospital until the Johannesburg General Hospital on Hospital Hill was officially opened in 1890. The sisters continued to serve in the hospital, despite many challenges such as the small pox outbreak in 1893 and the dynamite explosion of 1896. They showed devotion to nursing as they "undertook in the most whole-hearted way the entire nursing of the male natives, which always has been and will be embarrassing to arrange owing to local prejudices ... and have in addition nursed a small portion of white patients" (Brain 1991, 91). They served at the hospital until 1915.
Catholic hospitals faced many challenges (CATHCA 2011, 17, 116-120). The majority of Catholic hospitals were funded by oversees sponsors and few received state subsidies. Nurses, mostly religious sisters trained and qualified in their home countries, faced many challenges as legislation in South Africa demanded registration of nursing staff and their foreign qualifications were not always approved. Doctors and nurses often volunteered or were paid a meagre salary. Hospitals became expensive to run and with a declining global number of people joining religious orders from the 1970s onwards (particular sisters' congregations focused on active ministry, as opposed to contemplative orders), a number of facilities could not continue to operate. Declining vocations meant fewer sisters working in Catholic hospitals. With the increased cost of hiring lay staff, Catholic hospitals either had to adopt the private system of healthcare to survive or be handed over to the state. With increasing numbers of lay nurses and doctors in both public and private hospitals, religious communities also felt that there was no longer a need which they had to fill and they embarked on new missions serving in more rural areas.
Nearly all mission hospitals were appropriated to the state in the 1970s, except St Vincent's Hospital (Bela-Bela) and St Mary's Hospital (Mariannhill) (CATHCA 2011, 120). Although there was far less involvement of the missionaries in hospitals, they focused their attention on other areas such as home-based healthcare and outreach projects in rural communities.
Catholic Involvement in Healthcare Today
The Poor Sisters of Nazareth arrived in South Africa in 1881 and set up houses and orphanages to care for the elderly and children in Johannesburg, Cape Town, Kimberley, Port Elizabeth and Durban (CATHCA 2011, 111). The sisters continue until today to serve the communities in the houses they established and have extended their role to provide care for approximately 5 000 HIV-positive patients at the Clinic of Hope and Love (SACBC Aids Office 2012). They partnered with the Department of Health to provide antiretroviral drugs and laboratory testing, ensuring sustainability of the clinic and hospice (SACBC Aids Office 2014).
The Catholic Health Care Association (CATHCA), established in 1987, describes its vision as "to enable the provision of high-quality healthcare services to all, especially the poor and marginalised in South Africa, in the spirit and service of Christ" (Morgan and Goemans 2013, 191). CATHCA sees the necessity for the Catholic Church to partner with other stakeholders to address the needs of South Africans through advocacy in government policies. They are involved in training programmes for home-based healthcare, HIV/AIDS prevention education as well as HIV/AIDS testing and counselling (Morgan and Goemans 2013, 191-207).
This history of Trinity Health Services describes a clinic formed at Holy Trinity Catholic Church in Braamfontein and provides a new paradigm in Catholic healthcare in South Africa. It explains the role of the church and the partnerships needed in serving the homeless community of the parish. It is encapsulated in this statement:
... an inner-city parish somewhere in a poor city started a project like this based on the vision of a fourth-year student, and sheer doggedness has brought it to something like this ... (Interview, Pugin 2017)
The Rise of Trinity Health Services
Trinity Health Services (THS) is a student-run clinic that first served the homeless community on 26 July 2004 at Holy Trinity Catholic Church (Weber 2005), a parish served since the 1970s by the priests of the Society of Jesus (Jesuits), who have worked in South Africa since the 1870s (Ryan 1990). The Jesuits are a religious order with a long history of innovative ministry, including pioneering religious inculturation in China in the 17th and 18th centuries, secondary and tertiary education, academic research (including work in many sciences) and ecumenism (Bangert 1972; Woodrow 1990; Worcester 2008). By the late 20th century, the Jesuits were also deeply committed throughout the world to social justice, epitomised in Decree 4 of its 32nd General Congregation (1975), which insisted that all Jesuit ministries should have a justice dimension (GC32, 1975). These commitments could be found at Holy Trinity in 2004, where Jesuit pastors, working with the Society of St Vincent de Paul (SVDP) (a lay Catholic organisation dedicated to charitable work) embraced local homeless people as an integral part of the parish's life. They also serve two student chaplaincies, the University of Witwatersrand and the University of Johannesburg.
The clinic was started by two fourth year medical students, Bronwyn Weber and Michael Flynn. Weber, residing in Trinity House, worked at the parish's soup kitchen on Monday evenings. Trinity House is a student residence owned by the Catholic Archdiocese of Johannesburg adjacent to the church building. Students living at the residence come from various religious backgrounds but are requested as far as possible to participate in parish and student chaplaincy life. While volunteering at the SVDP soup kitchen as part of the latter engagement, Weber thought this would be an ideal location for an ad-hoc clinic. She noted that "as students, you want to be out there, you want to make a difference, you want to help and there wasn't anything" (Interview, Pitman [nee Weber] 2018). She approached the Jesuit priests at Trinity, Graham Pugin SJ (parish priest) and Anthony Egan SJ (student chaplain), in early 2004. Egan was asked by Weber whether he thought a clinic would be a good idea as she had observed that a number of people attending the soup kitchen were sick and didn't seem to visit any healthcare facilities. He agreed, but noted that this was outside the expertise of priests and the parish, and urged her to formulate a plan before approaching Graham Pugin. Weber approached Pugin and, following numerous discussions, approval was given. Egan recalls that Pugin was a little unsure, and said: "... it may be a little enthusiasm ... it might work for a few weeks, it might work for a few months, it may even last a year, he says, 'you know, the old Gamaliel principle; if it's God's will it will last, if it isn't, well you know, it's a nice little try'" (Interview, Egan 2017).
In the establishment of the clinic, students at the University of the Witwatersrand's Faculty of Health Sciences took the lead. From the start they came from a variety of religious backgrounds, if any. Unlike the SVDP, the focus was overtly humanitarian rather than religious. As the "founder," Weber (Interview, Pitman [nee Weber] 2018) was responsible for what she described as the "nagging." This involved getting the necessary permissions, determining how the clinic would complement the soup kitchen and negotiating the required space. Flynn (Interview 2018) was responsible for the logistics and fundraising. The role of the church, as Pugin (Interview 2017) recalled, was supportive: "[W)e have resources, we have contacts, we have people, we have networks, we have facilities, and to a modest extent we have money. And all those are things that a baby project like this desperately needs, and so it was providing the facilities, it was providing very basic supplies and it was providing contacts." The role of the Faculty of Health Sciences in the establishment was, at that point, minimal, though Weber remembers the faculty being aware of the project and encouraging it as it was seen as students doing voluntary community service. Pugin (Interview 2017) further describes the role of the faculty as follows: "... the students were getting no recognition for the hours they were doing, the work they were doing and ... felt: a) they were doing a good thing; and they felt b) they were getting some experience that they didn't get otherwise. I don't recall any enthusiastic support from the faculty, although individual doctors [who helped supervise the students] may well have had faculty links ..."
Weber and Flynn approached their fellow students to volunteer at the clinic. Student volunteers were, as noted above, from various cultural, religious and racial backgrounds. Pitman [nee Weber] (Interview 2018) recalls how the clinic operated. The volunteers would arrive dressed in their white coats and would set up a clinic outside, between the church and the priests' house, with chairs and tables for patients to be seen. The more severe cases, needing more privacy, were taken to a small consultation room in the basement of the church. Initially very few people accessed the clinic but in the weeks that followed more and more people came: "[W]e realised there was a huge need . [I]n fact, we were probably quite unprepared for the need" (Interview, Pitman [nee Weber] 2018).
Very limited services were initially offered, recalls Flynn (Interview 2018) ". a very basic, almost like first-aid type of service . [extended] into very basic over-the-counter medications . occasionally . a doctor . would come in and support us and . a more senior medical student would be there." Patients, who were mostly male, most commonly presented with psychological problems, alcohol abuse, sexually transmitted infections, dermatological conditions and tuberculosis. As the scope of the clinic was limited, patients needing additional care were referred to the CMJAH or Hillbrow Community Health Centre with a referral letter, which was "something more of a way for a patient to get into it . to encourage them to go and seek help rather than being something that could be used by the service that they were referred to ." (Interview, Flynn 2018).
For the next few years the service continued its limited medical care, providing over-the-counter medication and medical advice (Interview, Lorhman 2018). However, students began to see a need for the clinic to expand: "[O]ur goal was to try to turn it into a more functional clinic that could provide a few more services . [W]e found that basically everyone who had anything actually wrong with them, we had to refer, and even . for like minor complaints ..." (Interview, Lorhman 2018). Russell Pollitt SJ (Interview 2017), the then parish priest, confirmed this, saying ". these people needed the space and in order . [to] give better medical treatment, equipment was needed . So I remember thinking to myself it would be really good if we had space for people to be treated with dignity . that they weren't just on a chair outside in full view of everybody."
Father Tim Curtis, the then Director of the Jesuit Missions Office of the British Jesuit Province (of which the South African Jesuits were a region), had just visited South Africa and was impressed with the soup kitchen and clinic. Pollitt then wrote to Jesuit Missions, who sent out an appeal for donations towards the clinic in a publication called Jesuits and Friends.
THS received approximately R120 000.00, which was enough to reconfigure the available space at the parish to provide for three consultation rooms, a pharmacy and a store room. The remaining funds were used to buy necessary equipment. Fine (Interview 2018) describes how the services of the clinic expanded into the new spaces: "... we had formal consultation rooms which were fully stocked for examinations. We built up the pharmacy ... using the primary healthcare EDL [Essential Drug List] as our guideline and started providing a much larger range of primary healthcare type management." The official opening of the renovated facilities took place on 10 April 2010 and was supported by students and their families, as well as supervising professional staff and clergy.
The clinic's expansion into new spaces mirrored the formalisation of students into a committee. The committee consisted of eight members with defined portfolios: chairperson, vice-chair, treasurer and secretary as well as separate portfolios responsible for the pharmacy, HIV testing and referral, sterilisation and roster of volunteers (Trinity Health Services 2011). Members of the committee were voted in by the students who were volunteers at THS during a meeting held in October of each year. The committee outlined the aims of THS as follows:
Provide free basic healthcare for the homeless, unemployed and foreign people in Braamfontein and the surrounding areas.
Provide an opportunity for Health Science students to be exposed to patients, practise their clinical skills and use their theoretical knowledge in a clinical setting, in order to gain experience and to supplement their learning.
Give younger students an opportunity to learn from more experienced students as well as the consulting doctors. (Trinity Health Services 2011)
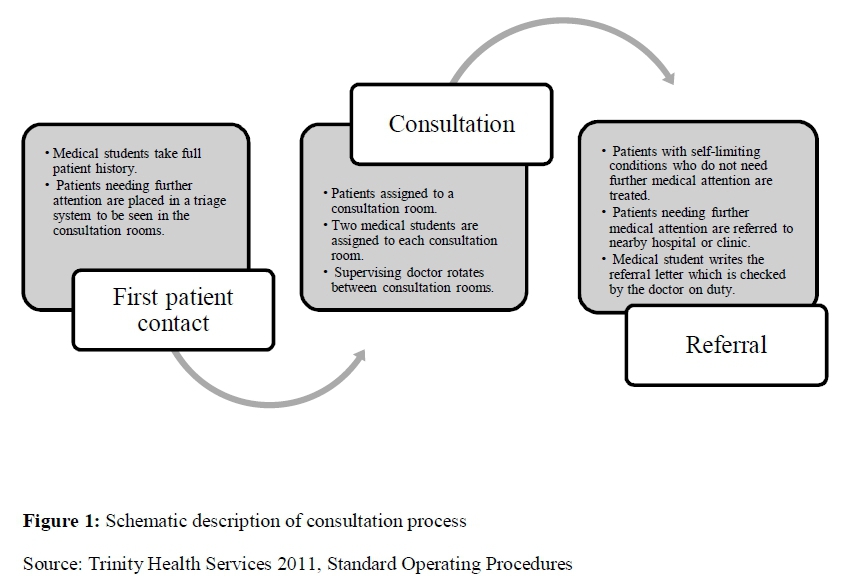
The clinic was thus a space where students from different years of study could work together in serving the community. The consultation process outlined in Figure 1 divides the tasks which volunteers were given, based on their year of study (Trinity Health Services 2011). The more junior students, first and second years, saw the patients first and could take vital measurements, performed outside in the area between the church and priests' house. The third and fourth year students consulted patients in rooms situated in the basement of the church and they presented cases to the senior students (fifth and sixth years), before obtaining final approval from the supervising doctor. The referral list expanded to include more specialised sites and specific facilities for South African and foreign patients. It was perceived that foreign patients were frequently turned away from certain hospitals and clinics.
Expanding Services to Include HIV Voluntary Counselling and Testing
Flynn (Interview 2018) explained that in the early stages the clinic would have liked to offer services such as HIV Voluntary Counselling and Testing (VCT), but it was not possible. This was one of the services that the clinic was able to provide through its expansion. Lorhman (Interview 2018) explains the reasoning for offering VCT: "[W]e always knew we were working with a very high-risk population ... homeless inner-city people, a lot of immigrants ... sex workers ... have a higher prevalence [of HIV] and they often get lost in the health care system ..."
The clinic partnered with New Start, a non-profit HIV programme, which was able to assist in training students and supporting the initiative. Students were excited to learn this new skill. Fine (Interview 2018) explains that "in some ways there was a selfish aspect to it in that it was something that we could learn, it was new for us, it would give us . a certificate to say that we were able to do something that our colleagues . still had to learn."
At this time "there was no research done on HIV prevalence for homeless people ." (Interview Botha 2018) which led to the development of a research project. Bruce Botha SJ, another Jesuit priest then based at Trinity, and Graham Lorhman, a medical student, together with researchers from the Wits Perinatal HIV Research Unit, applied for permission from the Human Research Ethics Committee of the University to conduct research which culminated in a publication entitled "HIV and the Urban Homeless in Johannesburg" published in the South African Journal of HIV Medicine (Lorhman et al. 2012). The study found that HIV prevalence in this community was not much different from the South African population of similar demographic profile. Homelessness on its own was not a risk factor, however, poverty and unemployment contributed to a higher prevalence of HIV (Lorhman et al. 2012).
With limited funding and resources, the clinic was "nowhere near a position to prescribe antiretrovirals" (Interview, Lorhman 2018). Patients testing positive needed to be referred to the Hillbrow Community Health Centre, unless the patient was a foreigner (often an "illegal" immigrant) in which case they were sent to Nazareth House for further assessment (as mentioned in the introduction, Nazareth House, in partnership with the Department of Health, provides antiretroviral medication to HIV positive patients). This was necessitated because, despite South Africa's Bill of Rights and the National Health Act, which both reject discrimination against patients on grounds of nationality, perceived "illegal immigrants" were sometimes chased away from state hospitals, particularly during times of heightened xenophobia.
The church was supportive of this initiative, despite opposing views regarding the use of condoms to promote safe sexual practices. In accordance with official Catholic teaching regarding family planning, the Catholic Church opposes the use of condoms in almost all circumstances (Paul VI 1968). Many Catholic moral theologians disagree with this, particularly in a context where the primary intention of condom use is to prevent HIV infection and save lives (Azetsop 2016; Bate and Munro 2014; Keenan et al. 2000; Kelly 1998). Students claimed that they were not allowed to advocate for the use of condoms and promote family planning (Interview, Fine 2018; Interview, Tambuze 2018), yet in the interviews conducted some of the priests said that the students needed to advocate for the needs of the patients first: "... if somebody's having multiple sex partners, you can't tell them don't use condoms" (Interview, Botha 2018); ". we have to negotiate our way around some official church policies which are extraordinarily neuralgic, regarding family planning, reproductive health, those kinds of things, and therefore very much touching on HIV issues ." (Interview, Pugin 2017); and "if they wanted to prescribe condoms to these folks, we're not going to ask questions, we're not going to look at it" (Interview, Egan 2017). The latter's observation reflects the actual complexity of the Catholic response to the AIDS crisis in South Africa; while officially strongly opposed to condom use, in practice through a multitude of state-run clinics in rural or peri-urban Catholic parishes, as well as through home-based healthcare, the church has become one of the largest distributors of antiretrovirals in South Africa and has frequently engaged in heated debate about condoms (Joshua 2010a; 2010b; 2014).
Whether the students perceived in some way that they were restricted from providing condoms, or whether other Catholics told them that, is uncertain. Strictly speaking, it can be argued that the medical use of condoms, following a reading of the encyclical Humanae Vitae itself, is allowed for "... therapeutic means necessary to cure bodily diseases ..." (Paul VI 1968). Though at the time Rome and the majority of bishops in South Africa rejected this claim (an exception being Bishop Kevin Dowling of Rustenberg [Joshua 2010b]), there is a strong tradition in Catholic moral theology that a dissenting view, if morally probable, may be entertained (a point one of the Jesuits at Trinity, a moral theologian by training, would have pointed out had he been asked) (Interview, Egan 2017). The decision to use or not use condoms, according to traditional Catholic ethics, is ultimately a matter of conscience which must be followed, whether or not it conforms to the official teaching of the church.
Another point worth raising is that the majority of the homeless community as well as the doctors were not Catholic, thus not "bound" by the church's moral teaching. However, as "guests" of the parish, possibly misinformed about the complexity of moral theology, or simply uneasy with raising a controversial issue, the students did not pursue the question further. Though it presented a challenge in the close collaboration between Trinity and THS, this issue reflects the complexity of the relationship and mirrors the subtle tension that always seems to exist between religious belief and medicine.
The Fall of Trinity Health Services
With the expansion of services, there was a need to prescribe and dispense more medication, necessitating the inclusion of a pharmacy. Although there was a room known as the "pharmacy" with a person assigned to dispense, there was no pharmacist present and the facility was not registered as such with the legislative authorities. Up until this point (September 2011) the required medication was prescribed by one of the supervising professional doctors and dispensed in bulk by a local pharmacy. The medication was kept in a toolbox, which was stored in a nearby pharmacy on days when the clinic was closed. On Mondays students would collect the medications from the pharmacy, take them to the clinic and medication was dispensed by a medical student in accordance with the prescriptions written. The medication was then (at the end of the day) returned to the pharmacy for safe keeping.
The student committee wanted to legalise the dispensing of medication and needed to register the pharmacy. They approached members of the Department of Pharmacy and Pharmacology. The initial perception of the committee was that this was a relatively easy task: "... our initial understanding, our initial sort of thoughts were that it would be a relatively quick process ..." (Interview, Fine 2018). This was confirmed by Bhikhoo (Interview 2018): "... you know when you . read about it, it just seems easy because you just follow the steps and it's . okay, get pharmacist, register pharmacy, get certain books, change pharmacy plans ... " The committee first applied for a community pharmacy license at the end of 2011, with Deanne Johnston, a lecturer from the Department of Pharmacy and Pharmacology, appointed as the Responsible Pharmacist.
In registering the pharmacy, the students needed to engage with the university. Students and the parish priest, Russell Pollitt, met with the Dean of the Faculty of Health Sciences and a few staff members. Although the dean was said to support this initiative, the clinic posed numerous legal risks. Pollitt (Interview 2017) described the meeting as follows:
I remember going to a meeting where his kind of question was "with whose permission are you doing this?" [I]t's always been supported, but no, you didn't ask for my permission, was the kind of attitude that we got from him. He raised all sorts of ... legal problems ... stuff around insurance and the university's culpability should something go wrong because it was no longer just sort of taking people's blood pressure but ... getting a little bit more serious. And I think there were questions about that insurance and then he involved the . legal department of the university and all sorts of things . I felt instead of finding an amicable way of doing this, it was basically ordered that the place be shut down ...
The students were disappointed. Many no longer wanted to help as they feared that it might compromise their future careers (Interview, Bhikhoo 2018). With a dwindling group of volunteers and pressure from the faculty, the clinic was temporarily closed in September 2011. Notices were placed around the church to inform the homeless community.
The response from the community was noted by Pollitt (Interview 2017): "I remember for weeks them coming to beg me because they just weren't getting any treatment at places like [CMJAH] . or they were getting poor treatment . they really, really suffered ." Bhikhoo (Interview 208) makes a valid point that the homeless are not often consulted when services are withdrawn: "[They are] used to sort of getting disappointed . you were entitled to this and now we are taking this away from you ... it's not a population that is used to having something."
Students also voiced their disappointment to Fine (Interview 2018): "Other students, younger students who had heard about Trinity, would often come up to me and say 'oh but I wanted to help' and they were quite disappointed when they heard that it was not functional."
A strong faculty supporter of the clinic, Adjunct Professor Lionel Green-Thompson (Interview 2018), who frequently supervised at THS, described his reaction: "I was so cross with the faculty for closing the clinic down. I was hopping mad, you know. And nobody could ever give me a full story . it was 'so and so' complained that we were overstepping our mark."
The Re-establishment
Following the temporary closure of the clinic, the primary task was to register the pharmacy with the South African Pharmacy Council (SAPC). This proved onerous, taking almost four years. The difficulty was in meeting the minimum standards for registering it as a community pharmacy. The Pharmacy Act 53 of 1974 (as amended) allows for the registration of community, consultant, manufacturing, institutional and wholesale pharmacy. The Act does not deviate from these categories and applies minimum standards which a pharmacy must meet according to the site plan of the pharmacy, submitted to the Department of Health. The only category, in which Trinity Pharmacy could be registered, was as a community pharmacy.
The committee's first application for a pharmacy license (in 2011) was unsuccessful. The SAPC raised concern with the ownership of the pharmacy being the church and the floor plans needed to be professionally drawn to scale reflecting the size of the pharmacy and premises. Ownership was discussed with the legal office of the university, with parish priest Pollitt, and with designated responsible pharmacist, Johnston. Following this meeting it was decided that the university should apply as the owner of Trinity Pharmacy.
The amended ownership documents and floor plans were submitted to the SAPC, but the license was denied once more in July 2012. The space demarcated for the pharmacy was too small and it could not meet the minimum standards for a community pharmacy. For example, there was no separate area for the receiving of stock, the dispensing area was too small and the pharmacy was not wheelchair accessible.
These findings were not easy to address and necessitated relocation of the pharmacy to ground level. Many meetings between the church, members of staff from the Department of Pharmacy and Pharmacology and the architect ensued. The required space was identified, and plans were drawn, but the required alterations were put on hold until the licence had been approved. The next application was sent to the Department of Health on 31 March 2014. Following a few minor changes, on 5 January 2015, the SAPC found the pharmacy to be compliant and sent a letter of recommendation to the Department of Health to issue a licence. The licence was signed on 14 February 2015 by the Director-General for Health. This marked the rejuvenation of Trinity Health Services and planning for the re-opening could now commence. The pharmacy site was on the ground floor of the priests' house. Building soon commenced, including a wheelchair ramp to allow access.
Meanwhile, following lengthy discussions between the church and the Faculty of Health Sciences, an agreement was reached. The church would be responsible for the premises of the clinic, including maintenance. The university, now the owner, assumed legal responsibility for the clinic, responsible for the staffing and management of funds (including fundraising). Many of the tasks would be allocated to the students.
Over the period when the clinic was closed, student involvement in the project dwindled as many of the tasks were out of their scope. Most of the students at the time of reopening had had no previous involvement with the project: "I remember I did speak to a few students in my class, and the way that they knew about the clinic is because they had siblings who had worked previously in the clinic who had already left Medical School . [S]tudents didn't actually know about the clinic because it wasn't something that was running when we were at Medical School ..." (Interview, Tambudze 2018).
The Wits Rural Health Club (WRHC), another student-run organisation, showed initial interest in the reopening of THS. Katherine Tambudze, a member of WRHC, together with interested students took responsibility for spreading the word and mobilised the students to form a separate committee. Gilbert Mardai SJ, the new parish priest when the clinic reopened, recalls the students' commitment: "I was very moved by the kind of spirit that I saw in the students when they were setting it up, the Saturdays that they came and cleaned up the rooms and prepared them, when they could have gone and studied. Just the positive energy that they had when they arrived there and trying to make sure that everything is well done" (Interview, Mardai 2018).
The inclusion of a pharmacy within the clinic necessitated the involvement of pharmacy students. The pharmacy students were enthusiastic as expressed in an interview with a fourth year pharmacy student, Thabo Justice Lephalala: "Other people out there, pharmacy students and other students at medical school, are ready to help because people just need a platform for 'okay so you can help here'; so now that we have a pharmacy and we have the knowledge and the skills to provide services, they will be willing to come and provide those services" (Lephalala in Random Acts of Kindness 2015).
On 1 February 2016, THS reopened its doors to offer primary healthcare services staffed by seven students (four from medicine and three from pharmacy) supervised by a doctor and pharmacist. Since then the clinic has provided a regular service upon which the homeless community can depend. Tambudze (Interview 2018) explained that "initially there was just a little bit of apprehension . I did expect, and I would understand why . but after a while things did get better, and we even had people who started coming more than once and we soon realised that some people just actually wanted to come and talk because they didn't really have anyone to talk to."
The official reopening ceremony took place on 24 May 2016. Green-Thompson (Interview 2018), now Assistant Dean of Teaching and Learning, at the Faculty of Health Sciences, observed: "This is the work of the students but in many ways, it reflects our social justice dimension . This is something that's grown out of the students, even in the second round" (Interview, Green-Thompson 2018).
Tambudze (Interview 2018) became team leader of the students, supported by an interprofessional team of medical and pharmacy students and described the first year as "trying to find our feet and figure things out." The team of students formed a committee with defined roles and responsibilities.
Analysis: The Role of Key Stakeholders Role of the Church
Trinity is a classic example of a good working parish that's developed a good working relationship with the university, that is operating across and beyond the sort of narrow, confessional boundaries and moving ... beyond even religious boundaries. (Interview, Egan 2017)
Holy Trinity Church has included a number of social apostolates including Justice and Peace, a lesbian, gay, bisexual, transgender and intersex (LGBTI) ministry, Community of Sant'Egidio and SVDP. These groups were founded in marginalised sectors of society.
Egan (Interview 2017) describes the extent of feeding homeless people at Trinity as follows:
Holy Trinity Braamfontein Parish had run a soup kitchen ... there are actually two sets of soup kitchens; the one was a Monday night soup kitchen, which was run by the Saint Vincent De Paul Society ... And during the mornings, the parish house keeper, the redoubtable Yvonne ... would run her own little soup kitchen for the homeless people, so we would feed people Mondays to Fridays ... at about 11:00 in the morning and we'd also have the evening ... we used to sometimes call it the 'feeding of the five thousand' ... on a Monday night.
Pugin (Interview 2017) is uncertain of when the Monday night SVDP soup kitchen began, but thinks it could have been in the 1980s. It was from the Monday night soup kitchen that the vision of a clinic grew. Initially the role of the church was marginal but expanded as the clinic developed: "We got outside funding but the church managed the funding. They gave us a place to work, they gave us a lot of support, they put us in contact with people who were helpful to us, they helped us organise the HIV counselling, testing, they supported us in many ways" (Interview Fine 2018) and "they were kind of the last word on every matter ... if you wanted to make any structural changes, if you wanted to start any new programmes they had to give the okay" (Interview, Lorhman 2018). Pollitt (Interview 2017) acknowledged that the church may seem to have "owned" the clinic, however, the church felt it was a joint responsibility between the students and church: ". it was seen as the church's thing because it was initiated on church property and so forth ... but it's quite clear that without the medical students, that thing would never have been able to run . [F]or me, it was a very good partnership because I felt like there was a collective responsibility."
The support the students received from the parish priests went beyond that of the management of the clinic: "... they gave us I think a lot of, you know, just kind of emotional psycho-social, psychological support. We were, I guess, in a situation where as students we didn't realise . the impact we were having on a lot of these guys who otherwise were not accessing healthcare. We realised it but to a very shallow degree I think, and they helped us realise, so they were very supportive in terms of that" (Interview, Fine 2018).
When the clinic was reopened the church reaffirmed its commitment in providing additional space for the pharmacy as Tambudze (Interview 2018) explained: "I remember even when it came to the new pharmacy and actually have it in the priests' house . I was like, wow . that's a big ask."
Mardai (Interview 2018) saw the supportive role the church played as twofold: "[F]irst it helps those who are beneficiaries . homeless" and is the social justice platform for students to learn: "They learn medicine, they may want to go into big hospitals [when] patients are coming from wealthy backgrounds, but they need to also have an exposure to the poor and as a church that is something that we . needed to support."
Julia Moolman (Interview 2018), a medical doctor who was chairperson of the parish pastoral council of Trinity, questioned the involvement of the parish in the clinic: "From the parish side there were very few discussions about the clinic, and about how it should run and what services we should be offering . I was quite in favour of the parish council playing a more active role in conceptualising the clinic ... we maybe haven't established its importance in the global picture . I definitely think in moving forward in the sustainability of it, it's something that really needs to be [examined]." This raises the point of broadening the view that the church is represented by the clergy and embedding the clinic within the parish, particularly given contemporary Catholic theology-following the Second Vatican Council (1962-1965)-that the church is the whole people of God, and that laity ought to take full and active responsibility in church life (Lumen Gentium 1964: nn.9-17; Gaudium et Spes 1965: nn.31 et passim).
Role of the Faculty of Health Sciences
The role of the Faculty of Health Sciences was difficult to confirm as many of the key role players who perhaps decided whether to support the clinic, are no longer at the University.
In the early days of THS little involvement from the faculty was needed, as described by Flynn (Interview 2018): "I think that the faculty initially wasn't specifically involved ... it was of interest from the faculty [to make sure] that students were involved in other activities outside [of university] . but . as soon as the faculty was aware of what we were doing, there was . a very keen interest in building it up and establishing it."
Lorhman (Interview 2018) recalls help from individual doctors who worked in the faculty: ". a lot of support, individuals . we really didn't struggle to get people there. So, so Dr Green-Thompson was a big proponent for us as well . a lot of people from family medicine kind of rotated through."
Even though staff may have been involved in supervising students, support from the faculty was lacking, especially when it came to the legalities of a clinic and pharmacy: ". initial support was underwhelming. I think because their, from a legal standpoint they couldn't ... as an institution take the risk of getting involved until it was fully legal and operated . I think we felt quite unsupported by Wits, which was very disappointing. If you look at Wits's quite proud history of social activism in previous decades . [M]y feeling was that apart from a few individuals they were decidedly unhelpful for the most part" (Interview, Fine 2018).
In the re-establishment students still feel unsupported by faculty: "I think the extensions of the faculty, which was mainly Deanne [Johnston] and Prof. Green-Thompson were very, very involved and very excited . I really struggled to get the rest of the faculty on board" (Interview, Tambudze 2018). The lack of faculty commitment was evident at the reopening of the clinic: "I think we sent out and invited most of the members of the faculty and not a lot of the members of the faculty supported . [T]hat would have been a great statement for them, even one or two to come through just to show support" (Interview, Tambudze 2018).
Green-Thompson (Interview 2018) explains that he has continued to volunteer "to demonstrate to the students that there's a level of faculty leadership that will be able to engage at the lowest level in a socially just paradigm or dimension." However, students do not perceive the involvement of a few staff members as representing the faculty and call for support especially as they try to expand the inter-professional team.
Role of the Students
As a student-initiated and student-run clinic, ownership of the project and the responsibility of operations lie within the students' realm. This is echoed in these comments:
[I]t's nice to be part of something that's your own as a student, but it's not a forced activity by the faculty, it is something that you want to do and it is something that you are learning from and growing from. (Interview, Bhikhoo 2018)
[T]he basis of the clinic is a student-run clinic, and I think with that in mind, most of the responsibility lies with the students . (Interview, Tambudze 2018)
I did at one point feel like it was, that was my baby, that was my thing, you know I spent a lot more time on that than I did on my university work, and that may or may not reflect in my marks, but it was you know, that's what kept me going through the difficult times in three years of med school . [E]very Monday I could be going to do something that I felt was worthwhile, kept me going. (Interview, Fine 2018)
The commitment from the students to THS, both initially and since the reopening, was noted by the parish priests:
So there was a real sense that students were very dedicated, they were enthused by this . and I found that inspiring because you know, here's these young people, you know, who were dealing with what I suppose the world would look at as the real dregs of society, these people who lived on the streets. They would come faithfully every single week and they would, you know, look after these people ... (Interview, Pollitt 2017)
... there are people who are not actually doing this for marks, they are not doing this for any trophy, they truly believe in helping another human being ... (Interview, Mardai 2018)
The experience of THS has had a long-lasting impact on the students in where they find themselves today:
... having that exposure to patients, both in terms of clinical ability and in terms of humanness, made a big difference when I started practising, when I started working. In my clinical years at "varsity" and as intern, and as a whole it grew my interest in primary [health]care. So currently I'm a Registrar in Family Medicine ... which would be as close as you could get to that sort of medicine. (Interview, Fine 2018)
[Y]ou kind of pick up on when someone is, is having something going on at home, almost, if someone has something non-medical . when you have spent time at the clinic and you speak to patients . they kind of mention, their illnesses and they ... hint at what is actually going on and what is really troubling them, their situation ... and if you are not exposed to that and you don't see that ... (Interview, Bhikhoo 2018)
[I]f you've worked in... that sort of... degree of poverty... you appreciate what you have ... [I]t's just a more broad level, but also I think it tends to make you want to be a better doctor (Interview, Flynn 2018)
A multi-layered partnership in mission is established between the church, faculty and students:
1. The clinic is aligned to the social mission of the church.
2. It is the mission of the university to form and train socially accountable healthcare professionals.
3. The clinic provides an opportunity for students to encounter patients and put into practice the skills and knowledge learnt in lectures under the supervision of staff.
This partnership demonstrates a post-modern shift. Neither stakeholder claim monopoly on the discourse, be they medical or religious. Each stakeholder approaches it from their own perspective, interest and ideology but ends up working for a common purpose.
Framing THS: Social Justice
The words of Dom Hélder Câmara, a Brazilian Roman Catholic Archbishop, "When I give food to the poor, they call me a saint. When I ask why they are poor, they call me a communist" (Rocha 2000, 53), recalled by Pugin (Interview 2017), explain the role of the clinic in both advocating for the homeless, but also in teaching students about social justice:
... you learn to advocate for your patients because you know how difficult it is for them, you know where they are coming from ... (Interview, Bhikhoo 2018)
... social responsibility is important that we don't just see people as bodies, but we need to understand their social circumstances. (Interview, Tambudze 2018)
This too is confirmed by the comments from Pollitt (Interview 2017): "[A]nother very important part of that thing was to expose, and let's face facts. Most of the medics who came there at the time when I started were young white people, who kind of came from privileged backgrounds, and I think the socialisation of exposing them to life on the streets, life in Braamfontein ... was a good thing for them to do as well."
Underserved communities, such as the homeless, often find themselves at the margins of society and the institutions they encounter need to respond to their requirements, as echoed in the comment from Mardai (Interview 2018): "... when we are running an organisation or an institution, that institution will not be rendering itself relevant to the society around it if it doesn't reach out to them ..."
It is no surprise that an initiative such as this was established in a Jesuit parish. Their involvement in the clinic aligns to Decree 4 of the Society of Jesus' 32nd General Congregation: "... the promotion of justice is not one apostolic area among others, the 'social apostolate'; rather, it should be the concern of our whole life and a dimension of all our apostolic endeavors" (GC 32, 1974-75).
Convergent and divergent themes in the History of THS and Catholic Healthcare
The story of THS can be compared to the multiple roles of Catholicism in healthcare within South Africa. Similarities can be drawn in the communities they serve, their approach to healthcare and legislative challenges they faced. Catholic hospitals and clinics that were established in South Africa were staffed by sisters who believed they had a duty to serve all people, regardless of race. Their view was one that all patients were deserving of quality healthcare services. THS serves the homeless community, which faces tremendous challenges when seeking healthcare. It strives to provide the best service possible with the limited resources at its disposal.
That Catholic hospitals were staffed by sisters, many of whom had received their nursing education abroad, was problematic as nurses working in South Africa needed to comply with the Medical and Pharmacy Act of 1891. This Act required all nurses working in the Cape to be registered and given certificates of competence. Due to shortages of nursing staff and the demand, many hospitals continued to allow religious sisters to practise as nurses. THS has faced its own legislative difficulties in attaining a licence for the pharmacy and it was closed for almost five years until approval was received. Healthcare is highly legislated and compliance with the prevailing laws is critical for the sustainability of services. However, it is often challenging to balance the prevailing needs with the legal framework.
There are also differences which need to be emphasised. Originally Catholic hospitals and clinics were managed by and staffed mainly by religious sisters. With the dwindling numbers of vocations, they could not maintain a strong presence in these hospitals. In contrast, THS, although situated in a Catholic parish, had and has very little, if any, overt religious ties. Students and staff who volunteer are from a variety of religious backgrounds, or none, and very few are Catholic. Most are motivated by humanitarian reasons. For their part, the Jesuits see the work as a social apostolate of service rather than any form of evangelisation (whether of students or homeless people). It should be noted that a few years ago some of the homeless-consulting with the parish staff-indicated an interest in a Bible study group, which they themselves run together with other parishioners.
A sandpaper-like relationship is described between the Sisters of the Holy Family of Bordeaux and the lay nurses at the Johannesburg General Hospital, with these two groups of nurses not able to work together (Brain 1991, 90). These two groups of nurses reportedly had a different approach to nursing and the lay nurses refused to take orders from the nuns. THS needed (and needs) multiple partners to work together for the survival of the clinic. The church, faculty and students must understand each other's roles. Historically, when mutual beneficial relationships were seen in organisations such as Nazareth House partnering with secular members of the community and the Department of Health, this strengthened existing services. THS continues this tradition, though without full medical engagement by faculty personnel.
Conclusion
Catholicism has had a profound effect on healthcare in South Africa although its influence in facilities today is almost non-existent. Catholic healthcare today is on a far smaller scale, focusing mainly on home-based healthcare. THS presents a new potential development of healthcare projects with Catholic links (by extension, this could be true for other religious traditions too). These projects call for a new approach where multiple partners, both religious and secular, need to form innovative strategies to address prevailing healthcare problems. In closing, these remarks by Mardai (Interview 2018) summarise the relationships between the partners of THS in providing healthcare for underserved communities:
[P]eople come there but they are coming because we have invited them . [T]hey come and they have a sheltered place and they can receive this kind of service . Medical School has rendered itself relevant and so has Holy Trinity and I think that is something that any institution should be doing. [We] shouldn't remain as ivory towers, we should become institutions that are making a difference outside the institution and that's precisely what the clinic has managed to do . (Interview, Mardai 2018)
References
Azetsop, Jacquineau (Ed.). 2016. HIV and AIDS in Africa: Christian Reflection, Public Health, Social Transformation. Maryknoll NY: Orbis. [ Links ]
Bangert, William V. 1972. A History of the Society of Jesus. St Louis: Institute of Jesuit Sources. [ Links ]
Bate, Stuart, and Munro, Alison (Eds). 2014. Catholic Responses to AIDS in Southern Africa. Pietermaritzburg: Cluster Publications. [ Links ]
Brain, Joy B. 1982. Catholics in Natal II. Durban: Archdiocese of Durban. [ Links ]
Brain, Joy B. 1991. The Catholic Church in the Transvaal. Johannesburg: Missionary Oblates of Mary Immaculate. [ Links ]
CATHCA. 2011. In the Service ofHealing: A History of Catholic Health Care in Southern Africa. Johannesburg: Catholic Health Care Association. [ Links ]
Favara, D. M. and Mendelsohn, S. C. 2012. "The Students' Health and Welfare Centres Organisation (SHAWCO) of the University of Cape Town: A Review of the Past 69 Years." SAMJ: South African Medical Journal 102 (6): 400-402. http://www.scielo.org.za/scielo.php?pid=S0256-95742012000600031&script=sci_arttext&tlng=pt. [ Links ]
Gaudium et Spes. 1965. "Pastoral Constitution on the Church in the Modern World" (promulgated 7 December 1965). Vatican Council II: The Conciliar and Post Conciliar Documents, edited by Austin Flannery. Dublin: Dominican Publications 1975, 903-1001. [ Links ]
GC32. 1975. 32nd General Congregation of the Society of Jesus, 1974-1975. "Service of Faith and the Promotion of Justice." Accessed 5 August 2018. https://www.scu.edu/ic/programs/ignatian-tradition-offerings/stories/decree-4-gc-32-service-of-faith-and-the-promotion-of-justice.html. [ Links ]
Gordon, C., 2016. "Volunteer, Community-Based Student-Run Clinics for the Underserved: Can they be Used to Attain 21st Century Medical Education Goals?" PhD thesis, Stellenbosch: Stellenbosch University. http://scholar.sun.ac.za/handle/10019.1/98371. [ Links ]
Joshua, Stephen Muoki. 2010a. "A Critical Historical Analysis of the South African Catholic Church's HIV/AIDS Response between 2000 and 2005." African Journal of AIDS Research 9 (4): 437-447. https://doi.org/10.2989/16085906.2010.545660. [ Links ]
Joshua, Stephen Muoki. 2010b. "The 'Dowling Controversy', the 'Message of Hope', and the Principle of Oikonomia: A Historical-critical Reflection on the South African Catholic Church's Stance on the Use of Condoms in HIV Prevention between 2000 and 2005." Journal of Theology for Southern Africa 137 (July): 4-27. https://search.proquest.com/docview/856599063?accountid=15083. [ Links ]
Joshua, Stephen Muoki. 2014. "'Tell me where I can find the Condom!' Catholic AIDS Discourses in South Africa during the 1990s." Historia 59 (1): 72-87. http://www.scielo.org.za/scielo.php?pid=S0018-229X2014000100005&script=sci_arttext&tlng=pt. [ Links ]
Keenan, James F. et al. (Eds). 2000. Catholic Ethicists on HIV/AIDS Prevention. New York: Continuum. [ Links ]
Kelly, Kevin T. 1998. New Directions in Sexual Ethics: Moral Theology and the Challenge of AIDS. London: Geoffrey Chapman. [ Links ]
Koenig, Harold G., McCullough, Michael E., Larson, David B. 2001. Handbook of Religion and Health. New York: Oxford University Press. https://doi.org/10.1093/acprof:oso/9780195118667.001.0001. [ Links ]
Lohrmann, Graham M., Botha, Bruce, Violari, Avy, Grey, Glenda E. 2012. "HIV and the Urban Homeless in Johannesburg." Southern African Journal of HIV Medicine 13 (4): 174-177. http://dx.doi.org/10.4102/sajhivmed.v13i4.111. [ Links ]
Lumen Gentium. 1964. "Dogmatic Constitution on the Church" (promulgated 21 November 1964). Vatican Council II: The Conciliar and Post Conciliar Documents, edited by Austin Flannery. Dublin: Dominican Publications 1975, 350-426. [ Links ]
Morgan, Yvonne, Goemans Loek. 2013. "Catholic Health Care: The CATHCA Story." In A Story Worth Telling: Essays in Honour of Cardinal Napier, edited by Bate, Stuart C. and Egan, Anthony, 191-207. Pretoria: South African Bishops Conference. [ Links ]
Paul VI. 1968. "Humanae Vitae." Accessed 25 July 2018. http://w2.vatican.va/content/paul-vi/en/encyclicals/documents/hf_p-vi_enc_25071968_humanae-vitae.html. [ Links ]
Pharmacy Act No. 53 of 1974. Accessed 5 August 2018. https://www.mm3admin.co.za/documents/docmanager/0C43CA52-121E-4F58-B8F6-81F656F2FD17/00010723.pdf. [ Links ]
Random Acts of Kindness. 2015. Random Acts of Kindness, Trinity Health Services. Accessed 3 July 2018. http://www.702.co.za/articles/9843/random-act-of-kindness-trinity-health-service. [ Links ]
Rocha, Zildo. 2000. Helder, O Dom: uma vida que marcou os rumos da Igreja no Brasil [Helder, the Gift: A Life that Marked the Course of the Church in Brazil]. Petropolis: Editora Vozes. [ Links ]
Ryan, J. A., 1990. An examination of the achievement of the Jesuit Order in South Africa, 18791934. Maters dissertation, Rhodes University. https://core.ac.uk/download/pdf/145042931.pdf. [ Links ]
SACBC Aids Office. 2012. Nazareth House Johannesburg, Accessed 3 July 2018. http://aidsoffice.sacbc.org.za/nazerth-house-johannesburg/. [ Links ]
SACBC Aids Office. 2014. "Gauteng Department of Health signs MOU with Nazareth House, Johannesburg." Accessed 3 July 2018. http://aidsoffice.sacbc.org.za/gauteng-department-of-health-signs-mou-with-nazareth-house-johannesburg/. [ Links ]
Trinity Health Services. 2011. Standard Operation Procedures. THS Archives (in possession of Zeenat Bhikhoo). [ Links ]
Weber, Bronwyn. 2005. "Trinity Health Service." The Auricle, January, page 10. [ Links ]
Wentzel, D., and Voce, A. 2012. "Health Seeking Experiences and Behaviours of Homeless People in Durban, South Africa." Africa Journal of Nursing and Midwifery 14 (2): 77-89. http://uir.unisa.ac.za/handle/10500/13014. [ Links ]
Woodrow, Alain. 1990. The Jesuits. A Story of Power. London: Geoffrey Chapman. [ Links ]
Worcester, Thomas. (Ed.). 2008. The Cambridge Companion to the Jesuits. Cambridge: Cambridge University Press. https://doi.org/10.1017/CCOL9780521857314. [ Links ]
Interviews
Bhikhoo, Zeenat. 2018. Interview, 22 February. Johannesburg: Wits Medical School. [ Links ]
Botha, Bruce. 2018. Interview, 10 January. Johannesburg: Jesuit Institute. [ Links ]
Egan, Anthony. 2017. Interview 28 November. Johannesburg: Jesuit Institute. [ Links ]
Fine, Nicholas. 2018. Interview, 25 January. Eastern Cape: Zithulele Hospital (by telephone). [ Links ]
Flynn, Michael. 2018. Interview, 6 February. London: Stockwell (by telephone). [ Links ]
Green-Thompson, Lionel. 2018. Interview, 1 March. Johannesburg: Wits Medical School. [ Links ]
Lorhman, Graham. 2018. Interview, 8 February. Boston: Roxbury (by telephone). [ Links ]
Mardai, Gilbert. 2018. Interview, 10 January. Harare: Arrupe Jesuit University (by telephone). [ Links ]
Moolman, Julia. 2018. Interview, 22 February. Malawi (by telephone). [ Links ]
Pitman [nee Weber], Bronwyn. 2018. Interview, 4 January. Cape Town: Wynberg (by telephone). [ Links ]
Pollitt, Russell. 2017. Interview, 20 December. Johannesburg: Jesuit Institute. [ Links ]
Pugin, Graham. 2017. Interview, 18 December. Johannesburg: Holy Trinity Catholic Church. [ Links ]
Tambudze, Katherine. 2018. Interview, 8 February. Bloemfontein (by telephone). [ Links ]


{kind=link}