










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Sports Medicine
On-line version ISSN 2078-516X
Print version ISSN 1015-5163
SA J. Sports Med. vol.28 n.1 Bloemfontein 2016
http://dx.doi.org/10.17159/2078-516x/2016/v28i1a424
ORIGINAL RESEARCH
CASE STUDY
An elite runner with cerebral palsy: cost of running determines athletic performance
LF PrinsI; PCM WoltersI; E CasalinoII; D ZimmermanIII; JJ de KoningIV; JP PorcariV; C FosterVI
IM.S.; VU University - Amsterdam, Research Institute MOVE, Netherlands
IIPhD; University of Rome "Foro Italico", Italy
IIIM.S.; University of Wisconsin-La Crosse, USA
IVPhD; VU University - Amsterdam, Research Institute MOVE, Netherlands
VPhD; University of Wisconsin-La Crosse, USA
VIPhD, FACSM; University of Wisconsin-La Crosse, USA
ABSTRACT
BACKGROUND: Running performance is widely understood in terms of the Joyner model (VO2max, %VO2max at ventilatory threshold (VT), running economy (often measured as cost of running (CR) as VO2 in ml.kg-1.km-1.
OBJECTIVE: To test the Joyner model by evaluating a runner in whom one element of the Joyner model is systematically abnormal.
METHODS: The case of a two-time Paralympian with cerebral palsy (CP), 2nd place in the Sydney 2000 Paralympic 1500m (T37) is reported. Incremental and steady state treadmill runs as well as simulated competitions were completed. Incremental and steady state (50% PPO) cycling with two legs (2L), the non-affected leg (NL), and the affected leg (AL) were also completed.
RESULTS: His silver medal (2000 Sydney OG) performance for 1500m was 269 s (4:29) (77.2% of velocity in contemporary able-bodied world record (WR). At the time of study, his VO2max was 64.2 ml.min-1.kg-1. His cost of running (CR) (1% grade) was higher, at 257 vs 228, 211 and 188 ml.kg-1.km-1 (for ACSM norms, elite Europeans, elite East Africans). During cycling, his VO2max with 2L, NL and AL was 3.74, 3.78 and 3.71 l.min-1, and his gross efficiency (GE) was 18.4, 12.2 and 9.3%, respectively.
CONCLUSIONS: In a former elite runner with CP, there is little evidence of a central oxygen transport limitation. The higher CR (plausibly reflected by the reduced GE of his AL) appears to account for much of the difference in performance compared to able-bodied runners. The results provide both insight into the physiological limitations of runners with CP and support for the Joyner model of competitive running performance.
Keywords: biomechanics, athletic training, exercise performance, exercise physiology
Running performance is well described by the Joyner model which explains performance as a function of VO2max, the %VO2max at lactate/ventilatory threshold and running economy, often expressed at the cost of running (CR) or VO2 (ml.kg-1.km-1).[11 There has been general support for this model, over a generation of sports scientists. A novel way of further testing this model is to evaluate runners where one element of the model is systematically different. This paper reports a case study of an elite runner with cerebral palsy (CP). CP is "a disorder of the development of movement and posture, causing activity limitations attributed to non-progressive disturbances in the developing fetal or infant brain".'21 CP is classified from the nature of the movement disorder and the anatomical distribution of motor abnormalities or severity. Our subject had spastic hemiplegia on the right side of his body, with unilateral involvement or spasms of the muscles including both arm and leg. He began running in his youth, and competed in different distances (800 m, 1500 m, and 5000 m) at two Paralympic Games (Athens 1996, Sydney 2000). His best performance was the silver medal in the 1500 m (T37 class) at the Sydney 2000 Paralympic games. His personal bests (compared to contemporary WR's in able-bodied runners were: (800 m = 132 s (2:13) vs 102.3 s (1:43)=77.5%WR; 1500 m=269 s4:29) vs207.7 s(3:27.7)=77.2%WR; 5000 m = 1060 s (17:42) vs 769.6 s (12:49.6) = 72.5%WR).
The purpose of this study is to provide insight into two aspects of performance in athletes with CP. First, what are the characteristics of running performance of a runner with CP compared to able-bodied runners? Second, how do persons with CP adapt to pathological conditions to achieve optimal function. These authors believe that this is the first study to report on CR and physical adaptation in an elite runner with CP.
Methods
At the time of the study (2011), the subject was 31 years old. He had participated in the 1996 and 2000 Paralympics, and had trained competitively until 2004. Although not competitive at the time of the physiological studies, he was still running three times per week for 30-40 min and cycling for transportation, mostly at intensities below the ventilatory threshold (VT). The study was approved by the university human subjects committee, according to principles of the Declaration of Helsinki, and the subject provided written informed consent.
The tests consisted of three parts: treadmill running, cycle ergometry and race simulations. All tests were performed at the same time of day (18h00-20h00) during summer. He undertook no intense training for 48 hrs and no training (except cycling for transportation purposes) for 24 hrs before each test. Laboratory tests and races were separated by at least 48 hours.
The subject performed incremental treadmill running until exhaustion (2.68 m.s-1 (9.64 km.h-1) +0.22 m.s-1 (0.8 km.h-1) each minute). He also performed steady state treadmill running (5 minute stages with 1 min walking recovery between stages). Performed on a different day, the steady state runs began at 2.23 m.s-1 (8.0 km.h-1) and increased by 0.22 m.s-1 (0.8 km.h-1) until the velocity at blood lactate = 4 mmol.l-1 was exceeded. All treadmill runs were performed with the treadmill belt at 1% elevation to mimic wind resistance. Respiratory gas exchange was measured using open-circuit spirometry, with a mixing chamber based metabolic system (AEI Inc, Bastrop, TX), and standard calibration procedures. VO2max was accepted as the highest continuous 30 s VO2 observed during the test. The cost of running (CR) was calculated from the interpolated VO2-velocity relationship at a VO2=90% of that at VT. This was done to assure that the CR represented steady state conditions, and to allow comparison to published norms.[3] Blood lactate was measured in capillary blood obtained from a fingertip using dry chemistry (Lactate Plus).
Two 1500m time trials were performed on an outdoor 400m track, with an experienced pacemaker, to allow comparison of race results between 2000 and 2011. The pacemaker attempted to run the pace that the subject believed that he could sustain. During the run, based on verbal communication between the subject and pacemaker (e.g. too slow, just right, too fast), the pace was regulated every 50-100m. During the last 400m, the subject attempted to pass the pacemaker, as he would in competition. Times were recorded every 100m.
Because running is an inherently a bilateral activity, and (as in this subject) CP is often a unilateral pathology the authors felt that it was important to assess differences between his affected leg (AL) and non-affected leg (NL). Accordingly, he performed incremental exercise using both legs 25 W + 25 W per 60 s) and, separately, with both the non-affected and affected legs (25 W + 15 W per 60 s, with 90 s on and 30 s off). Additionally, he performed a 10 min ride at steady state (50% peak power output) on the same cycle ergometer (Lode Excalibur, Groningen, NL), both with 2L and separately with the AL and NL.
Results
At the time of the study, the subject's height and weight were 1.75 m and 63.3 kg respectively, which were unchanged from his competitive years. During his peak competitive years, he trained ~4 times weekly, totalling ~40 km per week, including 2-3 interval training sessions. He stated that if he trained >4 days per week, he tended to become injured.
During incremental treadmill running, his VO2max = 64.2 ml.min-1.kg-1, his VO2@VT=52.8 ml.min-1.kg-1, his VO2@RCT (respiratory compensation threshold)=60.8 ml.min^.kg-1. His vMax= 4.58 m.s-1, vVT=3.58 m.s-1, vRCT=4.25 m.s-1, v4mmol=3.39 m.s-1 and vVO2max=4.33 m.s-1. His gross VO2max was 4,074 ml.min-1, with VT and RCT at 80% and 95% of VO2max. These percentages are high compared to the normal range of endurance athletes, possibly because the vVO2max was limited by the coordination and work capacity of the AL. This finding is duplicated in the cycling results. He remarked that during his competitive career, when he was fatigued, the toe of his AL tended to drop, occasionally causing him to fall.
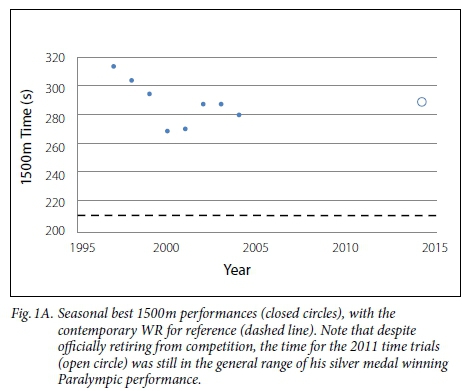
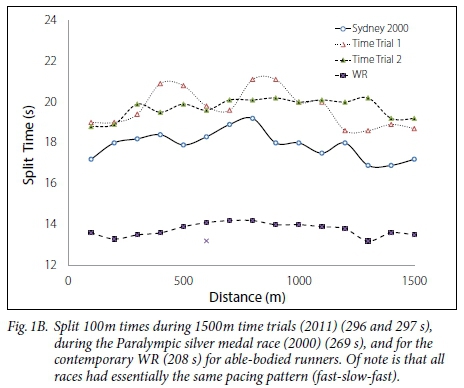
Comparing his silver medal race in 2000 with his 2011 1500m time trials shows that although he was slower (269 s (4:29) vs 297 s (4:57) and 296 s (4:56)) (Figure 1A), the pattern of pacing was virtually the same (Figure 1B). His final time in the two 2011 1500m time trials represented 91.0% and 91.4% of the velocity achieved during his silver medal race. Although the time trials were slower than his Paralympic race, they were in the general range of races during his late competitive career, which the authors believe provides evidence that the data collected during 2011 is representative of his physiological responses during his peak competitive period in 2000.
During cycling his peak power output (PPO) was 300 W, 105 W and 190 W with 2L, AL and NL, respectively. VOzinax was 3.74 (2L), 3.78 (AL) and 3.71 (NL) L.min-1. The VOzinax with 2L represented 92% of his running VO2max. It was remarkable that during 1L cycling with his AL, the pedalling action was very much "whole body", with a great degree of accessory muscle involvement, whereas with the NL the cycling action looked normal.
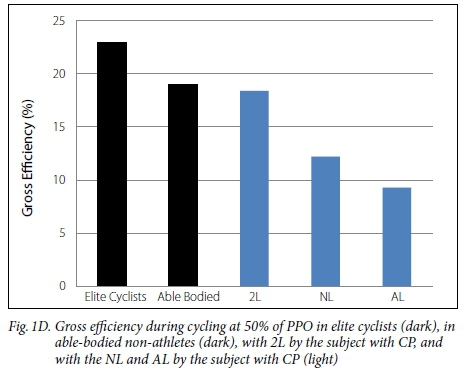
The higher CR ofour subject is presented in Figure 1C. The CR, with 1% grade, was 257 ml.kg-1.km-1 vs 228 ml.kg-1.km-1, 211 ml.kg-1.km-1 and 188 ml.kg-1.km-1 vs ACSM norms, elite Europeans and elite East Africans, respectively.'31 The GE during cycling is presented in Figure 1D, which depicts the range of elite cyclists, able-bodied individuals, and our subject's values for 2L, NL and AL. GE during 2L steady state cycling at 50% PPO was 18.4% (150 W, VO2=2.42 L.min-1, RER=0.84) (at the low end of normal), during 1L cycling with NL was 12.2% (95 W, VO2=2.27 L.min-1, RER=0.90) and during 1L cycling with his AL his GE was 9.3% (53 W, VO2=1.68 L.min-1, RER=0.95).

Discussion
The main finding of this case study was that an elite runner with CP was characterised by increased CR, which seems to define the mechanism of his reduced (compared to able-bodied runners) performance ability more than other variables in the Joyner model of running. This finding was supported by a decrease in GE during cycling in his AL. He was able to achieve VO2max even using the AL, apparently by extensive use of the accessory musculature to overcome the strength and coordinative deficit in the AL.
Extrapolating the speed-VO2 relationship observed in the laboratory his best 2011 performance would require a VO2 of 74 ml.min-1.kg-1, representing 115% VO2max. Assuming that the CR can improve by no more than 8%[4] and that VO2max is unlikely to increase smore than 2% with the addition of high-intensity interval training[5], the authors estimated that in Sydney at the 2000 Paralympic Games his CR was no lower than 238 ml.kg-1.km-1 and his VO2max was no higher than 66 ml.min-1.kg-1. On this basis, his Paralympic performance of 269 s would have required a VO2 of 79.9 ml.min-1.kg-1, or 121% of his estimated VO2max on race day. The percent of VO2max for both 2000 and 2011 performances are within reason for the relative intensity of elite able-bodied runners. While even his estimated Sydney 2000 race day VO2max is not equivalent to the ~75 ml.min-1.kg-1 typically seen in elite middle-distance runners (~85% as good), his best possible CR is high compared to elite ablebodied runners (~75% as good). Thus both the 2011 time trials and the projected values for his 2000 Paralympic performance support the Joyner model of running performance, and suggest that the primary difference between this elite runner with CP and elite able-bodied runners is dominantly related to an increase in the CR.[1]
His ability to adapt and have a very good performance despite the limitations imposed by CP appears attributable to his ability to recruit accessory muscles to overcome the limitations imposed by CP. This compensatory strategy extracts a cost in terms of reduced GE (e.g. increased CR), which is only possible if VO2max is reasonably high. A recent study from the authors' laboratory[6] in children with CP demonstrated that PPO (-25%) and Wingate PO (-40%) were more depressed than VO2max (-15%) compared to age matched controls. These data support the concept that limitations in mechanical power production (e.g. increased CR, decreased GE) contribute to the performance deficit in CP. They further suggest that therapeutic strategies with CP should include efforts to increase VO2max so that these patients can have the physiologic capacity to accommodate their neuromuscular deficit. Although not directly measured in this study, it is likely that the spasticity in the AL influenced the stretch-shortening cycle of the AL, decreasing the potential contribution of elastic recoil to propulsion. Further, chronic spasticity of the AL has the potential for reducing muscle blood flow, in much the same way that the extended duty cycle seen in speed skaters contributes to reduced muscle blood flow and VO2max.[7]
References
1. Joyner MJ. Modeling: optimal marathon performance on the basis of physiological factors. J Appl Physiol 1991;71:1496-1501. PMID: 1757375. [ Links ]
2. Bax M, Goldstein M, Rosenbaum P, et al. Proposed definition and classification of cerebral palsy. Dev Med Child Neurol 2005;47:571-576. [http://dx.doi.org/10.1016/j.jpeds.2008.04.013] [ Links ]
3. Foster C, Lucia A. Running economy: the forgotten factor in elite performance. Sports Med 2007;37:316-319. [http://dx.doi.org/10.2165/00007256-200737040-00011] PMID: 17465597. [ Links ]
4. Billat VL, Flechet B, Petit B, et al. Interval training at VO2max : effects on aerobic markers and overtraining markers. Med Sci Sports Exerc 1999;31:156-163. [http://dx.doi.org/10.1097/00005768-199901000-00024] PMID: 9927024. [ Links ]
5. Daniels JT, Yarborough RA, Foster C. Changes in VO2max and running performance with training. Eur J Appl Physiol Occup Physiol 1978;39:249-254. [http://dx.doi.org/10.1007/BF00421448] PMID: 710390. [ Links ]
6. Balemans AC, van Wely L, de Heer SJ, et al. Maximal aerobic and anaerobic exercise responses in children with cerebral palsy. Med Sci Sports Exerc 2013;45:561-568. [http://dx.doi.org/10.1249/MSS.0b013e3182732b2f] [ Links ]
7. Foster C, Rundell KW, Snyder AC, et al. Evidence for restricted muscle blood flow during speed skating. Med Sci Sports Exerc 1999;31: 1433-1440 [http://dx.doi.org/10.1097/00005768-199910000-00012] PMID: 10527516. [ Links ]
 Correspondence:
Correspondence:
C Foster
cfoster@uwlax.edu

