










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Journal of Sports Medicine
versión On-line ISSN 2078-516X
versión impresa ISSN 1015-5163
SA J. Sports Med. vol.28 no.1 Bloemfontein 2016
http://dx.doi.org/10.17159/2078-516x/2016/v28i1a745
ORIGINAL RESEARCH
Reliability and concurrent validity of an alternative method of lateral lumbar range of motion in athletes
Mark D HecimovichI; Jeffrey J HebertII
IPhD;University of Northern Iowa, Division of Athletic Training, 003C Human Performance Center, Cedar Falls, Iowa, USA
IIPhD;Murdoch University, School of Psychology and Exercise Science, 90 South Street, Murdoch, Western Australia, 6150
ABSTRACT
BACKGROUND: Cricket bowling involves combined spinal movements of side bending and rotation and, consequently, injury to the low back is a common problem. Therefore the assessment of lumbar spine kinematics has become a routine component in preseason screening. This includes static measurement of lateral spinal flexion as asymmetrical range of motion may predispose an athlete to low back injury.
OBJECTIVES: This study examined intra-rater reliability and concurrent validity of the fingertip-to-floor distance test (FFD) when compared to a criterion range of motion measure.
METHODS: Thirty-four junior-level cricket players aged 13-16 years were recruited. Lumbar spine lateral flexion was measured simultaneously with the fingertip-to-floor distance test and digital inclinometry methods. Relative and absolute intra-rater reliability were investigated with intraclass correlation coefficients (ICC3>1) of agreement, standard error of measurement (SEM) estimates, Bland and Altman bias estimates and 95% limits of agreement, respectively. The concurrent validity of the fingertip-to-floor distance test, compared to digital inclinometry measures, was examined with Pearson correlation coefficients.
RESULTS: Intra-rater reliability demonstrated substantial agreement for both measures (ICC3>1 > 0.84). The fingertip-to-floor distance test SEM values ranged from 1.71-2.01 cm with an estimated minimum detectable change (MDC) threshold of 4.73-5.55 cm. The inclinometry SEM values ranged from 1.00-1.09° with minimal detectable change estimates of 2.77-3.01°. There were strong correlations between the index test and criterion measure outcomes (r > 0.84, p < 0.001).
CONCLUSIONS: This study's results support the intra-rater reliability and concurrent validity of the finger-to-floor distance test, suggesting it to be a suitable surrogate measure for lumbar lateral flexion testing.
Keywords: authenticity, efficacy, range of motion, lumbar spine
Injury to the low back is a common problem in sporting populations[1] and more so in sports such as hockey,[2] cricket,[3] tennis[4] and sweep rowing[5] which involve combined spinal movements of side bending and rotation. Consequently the assessment of lumbar spine kinematics has become a routine component in preseason screening.[6,7,3] Tests include static measurement of lateral spinal flexion[7] as the asymmetrical range of motion may predispose an athlete to low back injury or be the result of a previous low back injury.[3] For example, it is accepted practice to measure lateral lumbar flexion in cricket players.[7]
In a sport such as cricket, considered to be a relatively low injury sport, only around five per cent of elite players are unavailable to play due to injury at any given time.[8,9] However, epidemiological studies in South Africa[10] have demonstrated that fast bowlers, who have an injury prevalence of approximately 15%,[9] have the highest risk of injury in cricket, with the low back being most susceptible to both traumatic and overuse injuries.[11] The reason for this is the inherent, high-load biomechanical nature of the bowling action'[9, 12] which may place undue stress on the pars interarticularis during the delivery stride due to large contralateral lumbar side-flexion motion coupled with large ground reaction forces.[13] The high prevalence of injury among fast bowlers[9,12] highlights the great need for research into factors associated with injury. Both extrinsic and intrinsic factors work in combination to predispose the bowler to injury.[14,15] Extrinsic or environment-related factors include bowling workload (the numbers of overs a bowler bowls), player position (first, second or third change) and time of play (morning or afternoon).[14,15] Intrinsic, or person-related, factors include flexibility (range of motion) muscle strength, balance and biomechanics.[14,15]
Young cricket players have a greater risk of injury to the back compared to adult cricket players. Successful prevention strategies for both adult and young players have been developed. These include identifying injury risk factors associated with physical characteristics to understand why an athlete may be predisposed to low back injury.[16,17] This has led to pre-participation screening protocols.[16] These protocols are commonly used to measure potential injury risk factors[17] that may predispose an athlete to low back injury. Included in these protocols are spinal and extremity range of motion, pelvic control, balance, and hip strength.[6,7] Currently, measurements such as spinal range of motion in lumbar lateral flexion and trunk rotation are obtained to measure asymmetries.[7] These measurements can be used in a prospective analysis of any injuries during a season.[7]
Measures of active lumber spine range of motion can be obtained with a number of methods including visual observation, tape measure/ruler, goniometry, linear measures, and inclinometry.[18] The method of assessment varies among clinicians and institutions based on factors such as time, educational inclination of the clinician, availability of equipment, and the specific movement or tissue being assessed.[18]
Digital inclinometry is recognised as a reliable and valid measure of joint range of motion.[19-21] However, this technology is expensive and not widely available to clinicians. As a result, measuring the fingertip-to-floor distance (FFD) for attainment of lateral spinal flexion of motion has been advocated as a suitable surrogate for digital inclinometry. Consequently, the FFD test is currently recommended by the Cricket Australia National Physiotherapy Working Group to quantify lateral lumbar spine range of motion as part of the annual preseason cricket screening program to allow a prospective analysis of any injuries suffered during a season.[7]
A preliminary report indicates the FFD test has an acceptable degree of measurement error.[7] However, a comprehensive investigation of FFD test reliability has not been undertaken and its level of concurrent validity compared to an accepted criterion standard is unknown. Therefore, the aim of this study was to examine the intra-rater reliability of the FFD test as well as its concurrent validity compared to digital inclinometry when measuring lumbar spine lateral flexion among a cohort of junior-level cricket players.
Methods
Ethics
The study protocol was approved by the Murdoch University Human Research Ethics Committee (2013/110) and all participants provided written consent prior to study enrolment.
Participants
Thirty-eight participants were recruited from members of the Talented Athlete Program of the Western Australian Cricket Association. Potential participants who reported a current history of spinal injury were excluded. All the participants recruited were required to undergo the annual preseason screening; however, this application may be used across all age and skill levels.
Procedures
For this study, lateral flexion of the lumbar spine was measured using two methods simultaneously. The index test was the FFD test at maximal lateral flexion. The criterion comparison was lumbar lateral flexion range of motion testing using dual digital inclinometry. Both methods were performed in a standing position with measures obtained by two examiners in a manner consistent with the National Physiotherapy Screening Protocol[7] and performed twice. The examiners underwent a two-hour training session in both methods given by a skilled professional of the methods. They were required to perform each method satisfactorily before being allowed to participate as examiners in the study.
Participants were guided through a warm-up before the measurements were recorded. The warm-up included a one-minute slow jog, seated lower extremity stretching which incorporated spinal flexion and rotation, and standing rotational and side bend stretching. The stretches were not taken to the participants' end range of motion. For both methods (Figs. 1a and 1b) participants stood barefoot with feet hip distance apart, with the contralateral base of fifth metatarsal and greater trochanter touching the wall. The arm nearest the wall was abducted, with the elbow comfortably flexed so that the participant did not push away from the wall. The participant was then instructed to 'slowly run your fingers down the outside of your leg and reach as far as you can while continuing to look straight ahead'. The participant maintained contact with the wall with both feet flat on the floor at all times. The participant laterally flexed at the trunk without a trunk or hip flexion or extension. The range of motion outcomes were measured bilaterally and categorised as Front Foot or Back Foot according to the participant's bowling side (throwing side).


For the index test, upon completion ofthe lateral flexion movement, the examiners used their finger to set the zero mark of the tape on the floor vertically below the mark on the participant's leg and level with base of the fifth metatarsal. While positioned side-on to the player, the examiner held the tape measure vertically and pulled it taut so that the tape was in contact with the participant's skin at the mark on their leg. The tape was then pulled taut along the contour of the leg up to the range of motion mark on the participant's leg.
The criterion test involved range of motion measures obtained with a Dualer IQ digital dual inclinometer (JTECH Medical, Salt Lake City, UT, USA), with primary and secondary sensors. With the participants standing in a neutral posture, the primary sensor was placed at the T12 spinal level with the secondary sensor placed at sacral midpoint. Once the participant reached their maximum lateral spinal flexion the range of motion measurement was recorded from the primary sensor by the second examiner.
Data were analysed with IBM SPSS version 21.0 software (IBM Corp, Armonk, NY). The relative and absolute intra-rater reliability of the index and criterion measures were examined by the authors. Relative reliability was examined with Model 3 agreement intra-class correlation coefficients of a single repetition (ICC3,1). ICC values greater than 0.75 are interpreted as indicating 'excellent' to 'good' reliability and those below 0.75 'poor' to 'moderate reliability'.[22] Absolute reliability was examined with the standard error of measurement (SEM).[22] The SEM estimates the variability of repeated measurements and is calculated from the sample standard deviation and the ICC (SEM = SDVi - ICC). Levels of minimal detectable change (MDC) from the SEM were calculated using the following formula: 1.96 x V 2 x SEM.[22] The MDC represents the smallest degree of change that exceeds measurement error and is used by clinicians to distinguish true change from change resulting from error. Finally, Bland and Altman plots were created and bias statistics calculated, and 95% limits of agreement.[23] To investigate the concurrent validity of the FFD test, the relationship of the test outcome was examined with the concurrent digital dual inclinometry measures using Pearson correlation coefficients. Alpha was 0.05 for all analyses.
Results
Thirty-four participants (27 male, 7 female) were enrolled with mean (SD) age = 14 (1) years, height = 172.0 (9.3) cm, weight = 62.0 (8.6) kg; and BMI = 21.6 (0.3) kg/m2.
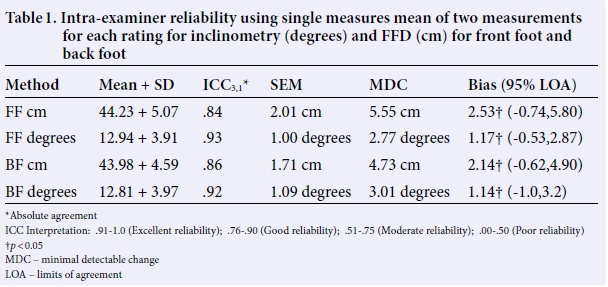
The intra-rater reliability analyses indicated substantial agreement for both measures (Table 1). The SEM for the Front Foot and Back Foot tape measure were 2.01 cm and 1.71 cm respectively with MDC estimates ranging from 5.55 cm (Front Foot) to 4.73 cm (Back Foot). The SEM for Front Foot and Back Foot inclinometry measures were 1.00 degrees and 1.09 degrees with MDC estimates of 2.77 degrees (Front Foot) and 3.01 degrees (Back Foot). Front Foot limits of agreement (LOA) were 2.53 cm (-0.74-5.80) and 1.17 degrees (-0.53-2.87) and Back Foot 2.14 cm (-0.62-4.90) and 1.14 degrees (-1.0-3.2), respectively
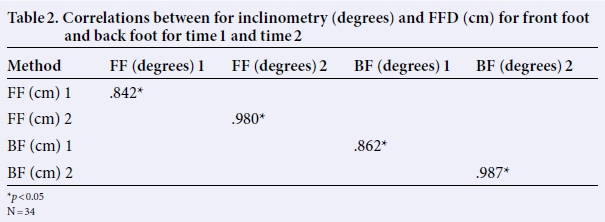
The results from the concurrent validity analyses are presented in Table 2. There were strong correlations between the index test and criterion measure (r > 0.84, p < 0.001).
Discussion
The intra-rater reliability of two measurement methods for standing lateral spinal flexion was examined as well as the concurrent validity ofa new test for lateral lumbar flexion range of motion in a cohort of healthy junior-level athletes. This was the first study to fully explore for potential sources of measurement error in the FFD test as well as to examine its validity by comparing its results with an accepted criterion standard.[24] This study's results support the intra-rater reliability (ICC3>1 = 0.84-0.86) and concurrent validity of the FFD as demonstrated by its strong associations with the criterion measure (r = 0.84-0.99). This result suggests the FFD test to be a suitable surrogate measure for lumbar lateral flexion testing.
This is consistent with a previous reliability analysis of the FFD test that reported substantial intra-rater reliability (ICC > 0.88).[7] However, there were several important measurement issues identified in the current study. First, both the FFD and digital inclinometry measures exhibited a positive bias between repetitions, indicating a source of systematic error. This means that the range of motion was greater during Repetition two than Repetition one, irrespective of measurement method. This finding suggests that to achieve measurement stability it is necessary to perform a series of 'warm-up' repetitions prior to testing lateral lumbar flexion range of motion. This practice is not part of current recommendations[7] and therefore additional research is needed to better understand this issue.
A comparison of ICC values between the two methods indicates the digital inclinometer measures to be more reliable than the FFD test outcomes. However, inspection of the absolute reliability estimates provides additional clarity. When compared to the mean values, the FFD had less error (SEM and MDC values) than digital inclinometry. For example, the MDC estimates were between 11-13% of the mean value for the FFD test and 21-24% for digital inclinometry. This means that compared to the FFD test, approximately twice as much change would need to occur in the inclinometry-derived range of motion measures before one could be confident that the difference resulted from 'true' change and not measurement error.
A likely explanation for the discrepancy between the relative (ICC) and absolute (SEM, MDC) reliability outcomes stems from the lower variance estimates observed with the FFD test. Low between-person variance depresses ICC values, making interpretation difficult. For example, a hypothetical study comparing ICC values for measures of elbow range of motion would likely find the ICCs of elbow flexion to be higher than for extension. This does not mean that clinicians are more reliable when measuring elbow flexion, but results from the fact that most people can extend their elbow to ~0 degrees, while there is much greater variability in elbow flexion. This limitation is well known[25] and highlights the importance of avoiding sole reliance on ICC analyses when making determinations about test reliability.
The utility of the FFD test is that it does not require expensive equipment and is easy to administer. However, individual differences in height and arm length are a potential source of bias in this measurement. Consequently, the FFD may be most appropriate for the quantification of range of motion change or side-to-side symmetry. For example, if the aim was to measure or monitor changes over time for a single player (effectiveness of a rehabilitation programme or injury) the FFD is ideal. If the aim was to obtain an angular measurement which can be used to compare between groups of players, the digital inclinometer would need to be utilised. Both the FFD and digital inclinometer can be used across all populations as the goal is to compare side-to-side measurements for symmetry.
Study limitations
These results should be considered within the study limitations. Although the examiners underwent standardised training for each method, the duration of the training was relatively brief (two hours). Therefore it is possible that more rigorous training may have enhanced measurement precision.[26,27] Another study limitation relates to the external validity of the results. As a cohort of young, healthy athletes was examined, these results should not be generalised to other populations, such as adults with low back pain or injury. Further research is needed to determine the optimal methodology for the FFD test, particularly with respect to the potential for systematic error resulting from a lack of measurement stability and the potential effect of a "warm-up" routine.
Conclusion
The high levels of intra-rater reliability (ICC3>1 = 0.84-0.86) and concurrent validity (r=0.84-0.99), demonstrate the FFD to be reproducible and a valid measure of lateral flexion range of motion. Measuring lateral flexion, especially for symmetrical side-to-side variations, is important in sports which involve combined spinal movements of side bending and rotation as differences may be a precursor for future injury. Thus clinicians can use this test as an alternative to digital inclinometry. This study's estimates of minimal detectable change demonstrate that approximately five cm of change is necessary before clinicians can be confident that the difference is not the result of measurement error. However, both methods demonstrate a small degree of systematic error (i degree, i.7 and 2.i cm) resulting from an increase in range of motion between repetitions, highlighting the potential importance of an appropriate 'warm up' routine prior to measurement.
References
1. Walker BF, Muller R, Grant WD. Low back pain in Australian adults. Prevalence and associated disability. J Manipulative Physiol Ther 2004;27(4):238-244. [http://dx.doi.org/10.1016/j.jmpt.2004.02.002] [ Links ]
2. Weir MR, Smith DS. Stress reaction of the pars interarticularis leading spondylolysis: a cause of adolescent low back pain. J Adolesc Health Care 1989;10(6):573-577. [http://dx.doi.org/10.1016/0197-0070(89)90029-6] [ Links ]
3. Stuelcken MC, Ginn KA, Sinclair PJ. Musculoskeletal profile of the lumbar spine and hip regions in cricket fast bowlers. Phys Ther Sport 2008;9(2):82-88. [http://dx.doi.org/10.1016/j.ptsp.2008.02.002] [ Links ]
4. Donatelli R, Dimond D, Holland M. Sport-specific biomechanics of spinal injuries in the athlete (throwing athletes, rotational sports, and contact-collision sports). Clin Sports Med 2012;31(3):381-396. [http://dx.doi.org/10.1016/j.csm.2012.03.003] [ Links ]
5. Strahan AD, Burnett AF, Caneiro JP, et al. Differences in spinopelvic kinematics in sweep and scull ergometer rowing. Clin J Sport Med 2011;21(4):330-336. [http://dx.doi.org/10.1097/JSM.0b013e31821a6465] [ Links ]
6. Dennis RJ, Finch CF, Elliott BC, et al. The reliability of musculoskeletal screening tests used in cricket. Phys Ther Sport 2008;9(1):25-33. [http://dx.doi.org/10.1016/j.ptsp.2007.09.004] [ Links ]
7. Cricket Australia Sport Science Sport Medicine Unit. National Physiotherapy Screening Protocol for 2013-14. Brisbane, AUS, 2013. [ Links ]
8. Mansingh A, Harper L, Headley S, et al. Injuries in West Indies cricket 2003-2004. Br J Sports Med 2006;40(2):119-123. [http://dx.doi.org/10.1136/bjsm.2005.019414] [ Links ]
9. Orchard JW, James T, Portus MR. Injuries to elite male cricketers in Australia over a 10-year period. J Sci Med Sport 2006;9(6):459-467. [http://dx.doi.org/10.1016/j.jsams.2006.05.001] [ Links ]
10. Stretch RA. Cricket injuries: a longitudinal study of the nature of injuries to South African cricketers. Br J Sports Med 2003;37(3):250-253. [http://dx.doi.org/10.1136/bjsm.37.3.250] [ Links ]
11. Weatherley CR, Hardcastle PH, Foster DH. Cricket. In: Watkins R (ed.). The spine in sports. St Louis (MO): Mosby, 1996;:414-429. [ Links ]
12. Frost WL, Chalmers DJ. Injury in elite New Zealand cricketers 2002-2008: descriptive epidemiology. Br J Sports Med 2014;48(12):2-7. [http://dx.doi.org/10.1136/bjsports-2012-091337] [ Links ]
13. Johnson M, Ferreira M, Hush J. Lumbar vertebral stress injuries in fast bowlers: a review of prevalence and risk factors. Phys Ther Sport 2012;13(1):45-52. [http://dx.doi.org/10.1016/j.ptsp.2011.01.002] [ Links ]
14. Orchard JW. Intrinsic and extrinsic risk factors for muscle strains in Australian football. Am J Sports Med 2001;29(3):300-303. [ Links ]
15. McBain K, Shrier I, Shultz R, et al. Prevention of sport injury II: a systematic review of clinical science research. Br J Sports Med 2012;46(3):174-179. [http://dx.doi.org/10.1136/bjsm.2010.081182] [ Links ]
16. Finch C. A new framework for research leading to sports injury prevention. J Sci Med Sport 2006;9(1):3-9. [http://dx.doi.org/10.1016/j.jsams.2006.02.009] [ Links ]
17. DiFiori J. Overuse injuries in children and adolescents. Phys Sportsmed 1999;27(1):75-89. [http://dx.doi.org/10.3810/psm.1999.01.652] [ Links ]
18. Clarkson HM. Head, neck, and trunk. In: Clarkson HM (eds.). Joint motion and function assessment: a research based practical guide. Philadelphia, PA: Lippincott Williams & Wilkins, 2005;:223-276. [ Links ]
19. De Winter AF, Heemskerk MA, Terwee CB, et al. Inter-observer reproducibility of measurements of range of motion in patients with shoulder pain using a digital inclinometer. BMC Musculoskelet Disord 2004;14:5-18. [http://dx.doi.org/10.1186/1471-2474-5-18] [ Links ]
20. Prushansky T, Deryi O, Jabarreen B. Reproducibility and validity of digital inclinometry for measuring cervical range of motion in normal subjects. Physiother Res Int 2010;15:42-48. [http://dx.doi.org/10.1002/pri.443] [ Links ]
21. Sohn J-H, Choi H-C, Lee S-M, et al. Differences in cervical musculoskeletal impairment between episodic and chronic tension-type headache. Cephalalgia 2010;30(12):1514-1523. [http://dx.doi.org/10.1177/0333102410375724] [ Links ]
22. Portney LG, Watkins MP. Foundations of clinical research: Applications to practice. 3rd ed. Philadelphia, PA: FA Davis Company, 2015. [ Links ]
23. Atkinson G, Nevill AM. Statistical methods for assessing measurement error (reliability) in variables relevant to sports medicine. Sport Med 1998;26(4):217-238. [http://dx.doi.org/10.2165/00007256-199826040-00002] [ Links ]
24. American Medical Association Guides to the Evaluation of Permanent Impairment. 5th ed. Chicago, IL: AMA, 2000. [ Links ]
25. De Vet HCW. Measurement in medicine: a practical guide. Cambridge, UK: Cambridge University Press, 2011. [http://dx.doi.org/10.1017/CBO9780511996214] [ Links ]
26. Brunse MH, Stochkendahl MJ, Vach W, et al. Examination of musculoskeletal chest pain - an inter-observer reliability study. Man Ther 2010;15(2):167-172. [http://dx.doi.org/10.1016/j.math.2009.10.003] [ Links ]
27. Cibere J, Thorne A, Bellamy N, et al. Reliability of the hip examination in osteoarthritis: effect of standardization. Arthritis Rheum 2008;59(3):373-381. [http://dx.doi.org/10.1002/art.23310] [ Links ]
 Correspondence:
Correspondence:
Mark Hecimovich
Mark.hecimovich@uni.edu


{kind=link}
{kind=link}