










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Sports Medicine
On-line version ISSN 2078-516X
Print version ISSN 1015-5163
SA J. Sports Med. vol.27 n.3 Bloemfontein Sep. 2015
http://dx.doi.org/10.7196/SAJSM.8112
ORIGINAL RESEARCH
Identifying risk factors that contribute to acute mountain sickness
Z MahomedI; D MartinII; E GilbertIII; C C GrantIV; J PatriciosV; F MotaraVI
IMB ChB, FCEM, MMed; Department of Sports Medicine, School of Medicine, Faculty of Health Sciences, University of Pretoria, South Africa
IIPhD; Centre for Altitude, Space and Extreme Environmental Medicine, University College London, UK
IIIMB ChB;Department of Sports Medicine, School of Medicine, Faculty of Health Sciences, University of Pretoria, South Africa
IVPhD;Department of Sports Medicine, School of Medicine, Faculty of Health Sciences, University of Pretoria, South Africa
VFACSM, FFSEM (UK); Centre for Altitude, Space and Extreme Environmental Medicine, University College London, UK
VIFCFP; Division of Emergency Medicine, Faculty of Health Sciences, Univeristy of the Witwatersrand, Johannesburg, South Africa
ABSTRACT
BACKGROUND: Acute mountain sickness (AMS) is an ever-increasing burden on the health sector. With reported incidences of greater than 50%, coupled with the fact that recreational activities at high altitude are gaining increasing popularity, more persons are developing AMS. Physicians are therefore increasingly faced with the task of managing and preventing AMS.
OBJECTIVES: The pathophysiology of AMS is poorly understood, with little understanding of risk factors for the development of AMS. This research aimed to identify epidemiological and physiological risk factors for development of AMS.
METHODS: This study is a questionnaire-based study conducted in London and at Everest Base Camp, in which 116 lowlanders were invited to participate and fill in a questionnaire to identify potential risk factors in their history that may have contributed to development of or protection against AMS.
RESULTS: A total of 89 lowlanders enrolled in the study. Thirty-seven of the participants had AMS at Everest Base Camp, giving a prevalence of 42%. Of the demographic variables, only weight and body mass index (BMI) were statistically significantly associated with AMS, with those who weighed less or had a lower BMI more likely to get AMS. Previous high-altitude experience was also associated with AMS, with those who had such experience less likely to get AMS.
CONCLUSION: Predicting AMS and furthering our understanding of the pathophysiology of AMS will be of tremendous benefit. Further research is needed in this regard.
Acute mountain sickness (AMS) is defined as the presence of a headache in an unacclimatised individual who has recently arrived at high altitude, along with gastrointestinal symptoms, insomnia, dizziness and lassitude or fatigue.[1] At the Seventh International Hypoxia Symposium held at Lake Louise, Canada,[2] AMS was further subdivided into mild, moderate and severe, based on the clinical presentation. This formed the basis for the Lake Louise Score, according to which mild AMS is defined as headache, nausea, dizziness and fatigue during the first 12 hours after ascent to altitude. Moderate AMS occurs when there is moderate to severe headache with marked nausea, dizziness, lassitude, insomnia and fluid retention at high altitude for 12 hours or more. Visitors to high altitude may also suffer from high-altitude cerebral oedema (HACE) and high-altitude pulmonary oedema (HAPE). HAPE and HACE are not severe forms of AMS; they can exist in their own right without preceding AMS and may have an entirely different pathophysiology.
The pathophysiology of AMS is not clearly understood. Signals generated at high altitude may activate the trigeminovascular system (i.e. neurons in the trigeminal nerve that innervate cerebral blood vessels) by both chemical and mechanical stimulation, causing a headache.[3] Many investigators believe that AMS is due to mild cerebral oedema and that all new climbers to high altitude may have mild cerebral oedema. In those with moderate to severe AMS, neuro-imaging demonstrated vasogenic oedema.[4] Capillary leakage following hypoxia-induced damage to the blood-brain barrier also plays a role. Mediators such as vascular endothelial growth factor, inducible nitric oxide synthase and bradykinin are also being studied. Several risk factors for the development of AMS have been identified; for example, speed of ascent greater than 300 - 500 m a day in the acclimatisation period, previous history of AMS or HAPE, obesity, migraine, persistence of a patent foramen ovale, Down syndrome, congenital pulmonary abnormalities, perinatal pulmonary vascular insult, and Holmes-Adie syndrome, are clinical conditions associated with susceptibility to AMS or HAPE.[5] This study was conducted at Everest Base Camp, with an altitude of 5 364 m. The incidence of AMS at Everest Base Camp has been reported to be as high as 57%.[6]
Approximately ten people a year die on Mount Kilimanjaro alone.[7] Millions of visitors travel each year to regions of high altitude, and the numbers are increasing as high altitude and extreme mountaineering become more accessible and ever more popular. It is evident that AMS will prove to be an ever-increasing burden on the healthcare industry. Identifying persons at increased risk of developing AMS and at an increased risk of progressing to HACE or HAPE will be invaluable to the high-altitude visitor as well as the healthcare professional.
Methods
Extreme Everest 2013 was an observational cohort study of human responses to progressive hypobaric hypoxia (during ascent) and subsequent normoxia (following descent), comparing sherpas (high-altitude ancestry) with lowlanders (lowland ancestry). Studies were conducted in London (35 m) in the UK and Kathmandu (1 300 m), Namche Bazaar (3 500 m) and Everest Base Camp (5 300 m) in Nepal. Of the 180 healthy volunteers departing from Kathmandu, 64 were sherpas and 116 were lowlanders. This research is a questionnaire-based study conducted in London and at Everest Base Camp. All 116 lowlanders participating in the Extreme Everest 2013 study were invited to take part in this study and to complete a questionnaire to identify potential risk factors in their history that may have contributed to development of AMS or protect against development of AMS. This cross-sectional, single-site study was limited to adults who are literate in English.
Procedure and design
At the testing sessions held at sea level in London volunteers were invited to participate in this study and to complete the study questionnaire. Thus the initial part of the questionnaire was completed at sea level in London, with the Lake Louise Score completed upon arrival at Everest Base Camp. Participants trekked in groups of up to 14. All lowlanders flew to Kathmandu and spent one night there prior to flying to Lukla (2 800 m). All participants followed an identical ascent and descent profile. The ascent to Everest Base Camp from Kathmandu was completed over 11 days, with rest days built into the schedule to reduce the likelihood of AMS.
The data collected in the questionnaire included the following:
- Biographical information: Participant's age, weight, height, gender, city of residence, previous high-altitude experience and previous episodes of AMS.
- Family history: Family history of heart attacks, cancer, high cholesterol, asthma, obesity, substance dependence, lung disease or high blood pressure.
- Personal medical conditions and medication use.
- A lifestyle evaluation questionnaire including exercise and fitness, nutrition, tobacco use, alcohol and drug use, emotional health, safety and disease prevention. (This questionnaire was developed by the United States Health and Human Services in 2006 so that the public perform self-evaluations on themselves.)
- A nutritional assessment questionnaire, adapted to assess food-related behaviour in the athlete. The higher the score, the poorer the participant's dietary habits.
- The frequency, intensity, time (FIT) index of Kasari (unpublished master's thesis, University of Montana, Missoula, 1976) which assesses frequency, intensity and time of exercise and sporting activity. This validated questionnaire was developed in the 1970s and shown to relate to aerobic fitness. It quantifies a respondent's participation in any form of physical activity; with an increase in the frequency, intensity and time of exercise there is an accompanying increase in the index score and fitness.
- The Physical Activity Readiness Score (PAR-Q), a self-screening tool developed by the British Columbia Ministry of Health and Multidisciplinary Board on Exercise to identify individuals who may be not be suitable for commencing strenuous exercise.
- The Paffenbarger Physical Activity Score, a short, self-administered questionnaire designed to measure participation in leisure-time physical activity. It consists of eight questions relating to daily activity; a physical activity index can be computed from the answers, providing an estimate of energy expenditure.
- The Lake Louise Score.[2]
Statistical analysis
Categorical data were described using frequency (percentage) and continuous data using median (interquartile range (IQR)). For comparisons between the two AMS groups (AMS, no AMS), the Mann-Whitney (7-test was used for continuous variables and the χ2 test or Fisher's exact test in the case of small expected counts for categorical variables. The non-parametric Mann-Whitney (7-test was used as the sample size was small and the distributions of variables were non-normal. All statistical analyses were performed using SPSS version 21.0 (IBM, USA). All tests were two-sided and a p-value <0.05 was considered to be statistically significant.
Ethical considerations
All participants were provided with patient information leaflets and all submitted written consent. The study design, risk management plan and protocols were approved (in accordance with the Declaration of Helsinki) both by the University College London Research Ethics Committee and the University College Committee on the Ethics of Non-National Health Service Human Research, and the Nepal Health Research Council.
Results
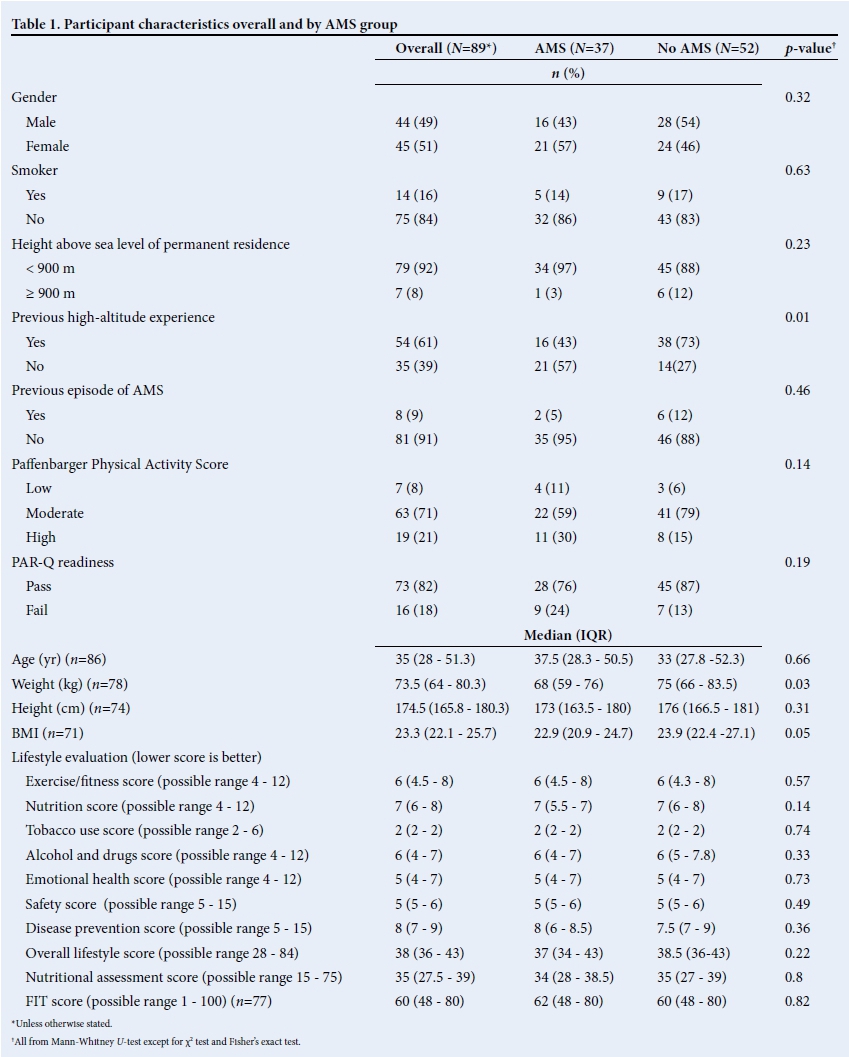
A total of 89 participants were enrolled into the study. The characteristics of the participants are presented in Table 1. Thirty-seven of the participants had AMS at Everest Base Camp, giving a prevalence of 42% (95% confidence interval (CI) 31 - 53%). For the demographic variables only weight (p=0.033) and body mass index (BMI) (p=0.047) were statistically significantly associated with AMS. Those participants who weighed less or had a lower BMI were more likely to get AMS. Previous high-altitude experience was also associated with AMS (p=0.005), with those who had previous high-altitude experience less likely to get AMS.
None of the lifestyle evaluation subscale scores nor the overall lifestyle score was significantly associated with AMS (p>0.05 for all). Similarly, the nutritional assessment score and FIT score were not significantly associated with AMS (p=0.799 and p=0.817, respectively). Those participants whose permanent residence was above 900 m (n=7) were less likely to get AMS than those whose residence was at a lower altitude, but the difference was not statistically significant (p=0.233). Similarly, those with a moderate Paffenbarger Physical Activity Score and those who achieved a pass on the readiness scale were less likely to get AMS, but the results were not statistically significant (p=0.141 and p=0.188, respectively).
The family medical histories ofparticipants are presented in Table 2. Only a family history of heart disease was statistically significantly associated with AMS (p=0.038), with those who had such a family history less likely to get AMS.

For the statistical analysis being overweight or obese were combined, and there was no statistically significant difference in BMI categories between the two AMS groups (p=0.171, χ2 test). BMI was left as a continuous variable for the results presented, and the difference between groups was statistically significant (as can be seen from Table 1).
Discussion
This cross-sectional study was conducted with the aim of identifying factors associated with a person's risk of developing AMS. The results largely conformed with those from existing research, with the exception of some interesting findings which will be discussed.
Does older age predispose one to developing AMS? This study showed no statistically significant protective benefit conferred by age, at least in the range of 19 - 74 years. However, other studies have showed that increased age conferred some benefit at high altitudes. For example, Roach et al.[8] studied the physiological and clinical response to moderate altitude (2 500 m) in 97 men and women aged 59 - 83 years, and found the incidence of AMS to be 16%, lower than that reported for younger persons. Even though 20% of the participants had coronary artery disease, 34% had hypertension and 9% had lung disease, the incidence of AMS remained low. Gaillard et al.[9] reported that people over the age of 55 years were 2.6 times less likely to suffer from AMS than people younger than 25 years, further suggesting that age might be a protective factor in developing AMS. A systematic review of the literature is required to answer this question definitively.
To date studies have shown that AMS is unrelated to gender. Hackett et al.[10] studied 278 hikers at Pheriche in Nepal, and their results showed that gender did not predispose one to developing AMS. Honigman et al.[11] showed that women may be less susceptible to HAPE, but equally as prone to AMS as men. Wang et al.[12] also showed no difference in prevalence of AMS between genders. Similarly, there was no significant difference between genders in this study (p=0.324).
Neither the lifestyle evaluation subscale scores nor the overall lifestyle score was significantly associated with AMS (p>0.05 for all). Similarly, the nutritional assessment score and FIT score were not significantly associated with AMS (p=0.799 and p=0.817, respectively). Physical fitness was also not shown to be protective against AMS, which is in keeping with the literature. Milledge et al.[13]showed no correlation between AMS scores and hypoxic ventilatory response or VO2 max.
One of the risk factors proposed by Hackett et al.[4] is that of residing at an altitude below 900 m: those participants whose permanent residence was above 900 m (n=7) were less likely to get AMS than those whose residence was at a lower altitude, but the difference was not statistically significant (p=0.233).
A prior history of AMS has been uniformly quoted as a risk factor by many authors.[1,8] This study showed that previous high-altitude experience was also associated with AMS (p=0.005), with those who had previous high-altitude experience less likely to get AMS.
In this study participants who weighed less or had a lower BMI were more likely to get AMS, which is in keeping with recent findings. Richalet et al.[5] recently reported regular physical activity as a risk factor for development of AMS. It would make sense that a fitter person with a lower BMI would do better at high altitude - but both Richalet et al.[5] and this study have shown the opposite. This is an interesting subject to explore and investigate further.
Chronic medical conditions and a family history of conditions such as hypertension, coronary artery disease, mild chronic obstructive pulmonary disease and diabetes, as well as pregnancy, do not appear to affect susceptibility to high-altitude illness.[14] The family medical histories of the participants are presented in Table 2. Only a family history of heart disease was associated with AMS (p=0.038), with those who had a family history less likely to get AMS.
Smoking has not yet proven to be a risk factor for development of AMS. Gaillard et al.[9]studied two cohorts of 500 trekkers in the Annapurna region of central Nepal, and found no relationship between AMS and smoking habits. Similarly, no relationship between smoking and developing AMS was found in this study (Table 1).
Conclusion
This study showed that certain parameters, such an increased weight, an increased BMI and previous altitude experience, decrease the risk of developing AMS. Lifestyle-scoring questionnaires did not predict those participants who might develop AMS. Furthermore, this study did not show a link between age, gender, fitness or smoking and the development of AMS.
With ever-increasing number of people visiting areas of high altitude, further research in this regard is anticipated to further expand our knowledge and understanding of AMS.
Acknowledgements. Xtreme Everest 2 was supported financially by the Royal Free Hospital NHS Trust Charity, the Special Trustees of University College London Hospital NHS Foundation Trust, the Southampton University Hospital Charity, the University College London Institute of Sports, Exercise and Health, The London Clinic, University College London, University of Southampton, Duke University Medical School, the United Kingdom Intensive Care Society, the National Institute of Academic Anaesthesia, the Rhinology and Laryngology Research Fund, the Physiological Society, Smiths Medical, Oroboros Instruments, Deltex Medical, Atlantic Customer Solutions, and the Xtreme Everest 2 volunteer participants who trekked to Everest base camp.
Some of this work was undertaken at University College London Hospital/University College London Biomedical Research Centre, as well as at the University Hospital Southampton/ University of Southampton Respiratory Biomedical Research Unit, both of which received a proportion of funding from the UK Department of Health's National Institute for Health Research Biomedical Research Centre's funding scheme.
Xtreme Everest 2 is a research project coordinated by the Xtreme Everest Oxygen Research Consortium, a collaboration between the University College London Centre for Altitude, Space, and Extreme Environment Medicine, the Centre for Human Integrative Physiology at the University of Southampton and the Duke University Medical Centre.
Membership, roles, and responsibilities of the Xtreme Everest 2 Research Group can be found at www.xtreme-everest.co.uk/team.
Members of the Xtreme Everest 2 Research Group: S Abraham, T Adams, W Anseeuw, R Astin, B Basnyat, O Burdall, J Carroll, A Cobb, J Coppel, O Couppis, J Court, A Cumptsey, T Davies, S Dhillon, N Diamond, C Dougall, T Geliot, E Gilbert-Kawai, G Gilbert-Kawai, E Gnaiger, M Grocott, C Haldane, P Hennis, J Horscroft, D Howard, S Jack, B Jarvis, W Jenner, G Jones, J van der Kaaij, J Kenth, A Kotwica, R Kumar, J Lacey, V Laner, D Levett, D Martin, P Meale, K Mitchell, Z Mahomed, J Moonie, A Murray, M Mythen, P Mythen, K O'Brien, I Ruggles-Brice, K Salmon, A Sheperdigian, T Smedley, B Symons, C Tomlinson, A Vercueil, L Wandrag, S Ward, A Wight, C Wilkinson, S Wythe.
Scientific Advisory Board: M Feelisch, E Gilbert-Kawai, M Grocott (chair), M Hanson, D Levett, D Martin, K Mitchell, H Montgomery, R Moon, A Murray, M Mythen, M Peters.
References
1. Mehta SR, Chawla A, Kashyap AS. Acute mountain sickness, high altitude cerebral oedema, high altitude pulmonary oedema: The current concepts. Med J Armed Forces India 2008;64(2):149-153. [http://dx.doi.org/10.1016/s0377-1237(08)80062-7] [ Links ]
2. Sutton J, Coates G, Houston C, eds. Hypoxia and Mountain Medicine: Proceedings of the 7th International Hypoxia Symposium, Lake Louise, Canada. Oxford: Pergamon Press, 1991:327-330. [ Links ]
3. Sanchez del Rio M, Moskowitz MA. High altitude headache. Lessons from headaches at sea level. Adv Exp Med Biol 1999;474:145-153. [http://dx.doi.org/10.1007/978-1-4615-4711-2_13] [ Links ]
4. Hacket PH, Yarnell PR, Hill R, et al. High altitude cerebral edema evaluated with magnetic resonance imaging: Clinical correlation and pathophysiology. JAMA 1998;280:1920-1925. [http://dx.doi.org/10.1097/00008506-199904000-00020] [ Links ]
5. Richalet JP, Larmignat P, Poitrine E, et al. Physiological risk factors for severe high altitude illness. Am J Respir Crit Care Med 2012;185(2):192-198. [http://dx.doi.org/10.1164/rccm.201108-1396oc] [ Links ]
6. Murdoch DR. Symptoms of infection and altitude illness among hikers in the Mount Everest Region of Nepal. Aviat Space Environ Med 1995;66(2):148-151. [ Links ]
7. Johnston J. The other side of the mountain. 2000. http://www.alpineascents.com/kili-article.htm (accessed 20 May 2012). [ Links ]
8. Roach RC, Houston SC, Honigman B, et al. How well do older persons tolerate moderate altitude? West J Med 1995;162(1):32-36. [ Links ]
9. Gaillard S, Dellasanta P, Loutan L, et al. Awareness, prevalence, medication use and risk factors of acute mountain sickness in tourists trekking around the Annapurnas in Nepal: A 12 year follow-up. High Alt Med Biol 2004;5(4):410-419. [http://dx.doi.org/10.1089/ham.2004.5.410] [ Links ]
10. Hackett PH, Rennie D, Levine HD. The incidence, importance and prophylaxis of acute mountain sickness. Lancet 1976;2(7996):1149-1155. [http://dx.doi.org/10.1016/s0140-6736(76)91677-9] [ Links ]
11. Honigman B, Theis MK, Koziol-McLain J, et al. Acute mountain sickness in a general tourist population at moderate altitudes. Ann Intern Med 1993;118(8):587-592. [http://dx.doi.org/10.7326/0003-4819-118-8-199304150-00003] [ Links ]
12. Wang SH, Chen YC, Kao WF, et al. Epidemiology of acute mountain sickness on Jade Mountain, Taiwan: An annual prospective observational study. High Alt Med Biol 2012;11(1):43-49. [http://dx.doi.org/10.1089/ham.2009.1063] [ Links ]
13. Milledge JS, Beeley JM, Broome J, et al. Acute mountain sickness susceptibility, fitness and hypoxic ventilatory response. Eur Respir J 1991;4(8):1000-1003. [ Links ]
14. Schoene RB. High altitude: An exploration of human adaption. Integr Comp Biol 2002;42(4):910. [http://dx.doi.org/10.1093/icb/42.4.910] [ Links ]
Corresponding author: Z Mahomed (zeynmahomed@gmail.com)


{kind=link}