










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Journal of Sports Medicine
versión On-line ISSN 2078-516X
versión impresa ISSN 1015-5163
SA J. Sports Med. vol.27 no.2 Bloemfontein jun. 2015
http://dx.doi.org/10.7196/SAJSM.536
ORIGINAL RESEARCH
Concussion knowledge and return-to-play attitudes among subelite rugby union players
SP Walker
MSocSc (Couns Psych), PhD; Unit for Professional Training and Services in the Behavioural Sciences (UNIBS), Faculty of the Humanities, University of the Free State, Bloemfontein, South Africa
ABSTRACT
BACKGROUND: Concussion is a significant health issue in rugby union. However, little is known about players' levels of concussion knowledge or return-to-play (RTP) attitudes.
OBJECTIVES: To determine the concussion knowledge and concussion-related RTP attitudes of subelite rugby union players in South Africa.
METHODS: Subelite rugby union players (n=127; mean age 24.1 years) completed a measure of concussion knowledge and a concussion-related RTP attitude scale. Frequencies were calculated with regard to concussion knowledge and RTP attitudes for the total sample, as well as separately for previously concussed and non-concussed participants. Pearson's χ2 tests and t-tests for independent groups were employed to determine significant differences in concussion knowledge and RTP attitudes between previously concussed and non-concussed participants.
RESULTS: Participants displayed varying, yet generally less than optimal levels of concussion knowledge. Knowledge of concussion-related RTP protocols (20 - 23%) and the efficacy of safety equipment (20 - 25%) was particularly poor. The subelite rugby players included in the sample did not hold notably conservative RTP attitudes, with the majority expressing a willingness to participate in practice (74%) and competition (47 - 56%) without having fully recovered from a concussion. No significant differences were apparent with regard to the RTP attitudes and concussion knowledge of the previously concussed and non-concussed players.
CONCLUSION: The general level of concussion knowledge among subelite rugby union players appears less than optimal. Moreover, the majority of these players expressed an intention to RTP before they had fully recovered from concussion.
Concussion has been identified as a high priority health issue in rugby union.[1-4] An incidence of 7.97 concussions per 1 000 player game hours has been reported for non-professional Australian rugby players.[1] Concussions accounted for 9.7% of the injuries reported for elite southern hemisphere rugby union players across one season, while constituting 4.8% of injuries reported across the same season of English Premiership Rugby.[5] In South Africa (SA), the seasonal incidence of concussion has been estimated to range from 4% to 14% at school level and between 3% and 23% at senior level.[2] However, a number of researchers contend that it is extremely difficult to accurately determine the incidence of sport-related concussion and that the current research literature might significantly underestimate the extent of the problem.[6,7]
Effective concussion prevention and management has been highlighted as a priority in contact sports in general, and particularly in rugby union. A series of consensus statements have called for the implementation of uniform measures aimed not only at the effective identification and management of concussion, but also at a reduction in the incidence of concussion in contact sports.[8,9] These consensus statements recommend focusing on (i) the standardised identification and management of concussion, (ii) the implementation of regulations and rule changes in various sporting codes intended to reduce the risk of concussion, and (iii) the implementation of education initiatives aimed at increasing awareness of sport-related concussion. These recommendations have been officially adopted and implemented by numerous sporting bodies across the world, including the International Rugby Board (IRB) and the South African Rugby Union (SARU).[3,10]
The administrative and medical guidelines recommended in the consensus statements on sport-related concussion appear to have been partially effectively implemented in rugby union. Uniform processes for screening for and diagnosing concussion, as well as specific return-to-play (RTP) guidelines have been implemented by SARU at both the professional and amateur levels.[3] However, while a number of broad-based concussion education initiatives have been introduced worldwide, these appear to have had a less than optimal impact on the concussion-related knowledge and behaviour of rugby union players in a number of countries. One study found that 78% of concussed Australian amateur rugby union players did not receive any RTP advice.[11] Moreover, those players who did receive RTP advice generally failed to follow those guidelines. Similarly, a study conducted in New Zealand indicated that a significant proportion of schoolboy rugby players had limited concussion knowledge and failed to comply with recommended concussion-related RTP guidelines.[12] The parents of schoolboy rugby union players generally seemed more knowledgeable than their children with regard to the identification of concussion and the potential dangers thereof.[13] However, these parents still demonstrated less than optimal knowledge regarding recommended concussion-related RTP guidelines. Similarly, a recent investigation into the concussion knowledge of coaches in Australian Rules Football and Rugby League concluded that the prescribed guidelines on concussion prevention and management did not appear to be filtering down to the coaches and paramedical staff involved in these sports in Australia.[14]
Policy and rule changes seem to have contributed to a reduction in the incidence of concussion.[1,4] However, the limited number of studies published in the field suggest that educational interventions aimed at increasing concussion knowledge and promoting player compliance with RTP guidelines have been less successful. [11-14] This is of particular concern when the dangers associated with premature post-concussion RTP are considered. Premature RTP following a concussion may result in a number of complications that include prolonging cognitive and self-regulation difficulties frequently associated with concussion, increasing the risk of subsequent concussions, post-concussion syndrome, second impact syndrome or even chronic traumatic encephalopathy.[4,15,16]
There seems to be a dearth of information regarding the level of concussion knowledge and RTP attitudes among elite and subelite rugby union players both nationally and internationally. Consequently, the current study aimed to determine the level of concussion knowledge among subelite rugby union players in SA. The study also aimed to explore concussion-related RTP attitudes in this population.
Methods
Participants
Ethical clearance to conduct the study was obtained from the relevant institutional body. Two provincial rugby unions granted permission for data to be collected among clubs registered under their auspices. Seven of a potential 25 clubs agreed to participate in the study and informed consent was obtained from 139 subelite rugby union players. Participants completed the measures listed below before or after practices, depending upon the preferences of their coaches. Twelve questionnaires were excluded due to incomplete data. The mean age of the final sample (n=127) was 24.1 years (standard deviation (SD) 4.9). Fifty-one (40%) participants reported club rugby as their highest level of competition, while 16% had competed provincially at under-19 level and 17% at under-21 level. Twenty players (16%) reported selection for development teams as their highest level of competition.
Measures
Concussion knowledge was measured by means of a 13-item multiple-choice questionnaire based on previous work done among coaches and healthcare professionals in primary school rugby.[17] Items on the questionnaire sampled knowledge regarding the identification of concussion, concussion risks, the management of concussion and RTP guidelines.[9] Each item was presented as a question or statement with one correct response and a number of distractors. The questionnaire was scored by awarding one mark for endorsement of the correct response to each question and zero for endorsement of one of the distractors. The scores across all 13 items were added to yield a total concussion knowledge score.
Concussion-related RTP attitudes were measured via a five-item questionnaire compiled by the researcher. Respondents were required to indicate the extent to which they would be inclined to participate in a practice, play a friendly game, play in a league final, participate in provincial trials and participate in national trials despite not having fully recovered from a concussion. Responses were recorded along a five-point Likert-type scale anchored by (1) should/ would definitely play and (5) should/would definitely not play.
Both measures were translated into Afrikaans via the back-translation method.[18] The questionnaires were administered in either English or Afrikaans depending upon participant preference. Biographical data pertaining to age and highest level of competition were collected. Participants were required to indicate whether they had ever suffered a concussion by endorsing one of three response options (yes, no or unsure). Those participants stating that they had previously been concussed were also required to indicate the number of concussions they had suffered across their playing careers.
Analysis
Descriptive statistics were calculated with regard to the number of rugby-related concussions reported by the participants. The 13 concussion knowledge items were scored and frequencies were calculated for the sample as a whole. Furthermore, in order to investigate whether players reporting a history of concussion differed from those reporting no history of concussion with regard to their concussion knowledge, frequencies were also calculated for the previously concussed and previously non-concussed participants separately. Pearson's χ2 tests were conducted to determine the statistical significance of any differences in the scores obtained by previously concussed and non-concussed participants on the concussion knowledge items. [19] In addition, the number of individuals indicating a definite intention not to return to play or practice before fully recovering from concussion was calculated for each of the five concussion-related RTP scenarios. These frequencies were calculated for the total sample, as well as for the previously concussed and non-concussed groups separately. Pearson's χ2 tests were employed to determine whether any statistically significant differences were apparent in the concussion-related RTP attitudes of the previously concussed and non-concussed players. Independent groups' t-tests were also employed to determine whether the total concussion knowledge and mean RTP attitudes of the two groups differed significantly. All analyses were performed using the Statistical Software Package for the Social Sciences (SPSS), version 21 (IBM Corporation, USA).[20]
Results
The frequency distribution in the sample with respect to the number of rugby-related concussions is shown in Table 1.
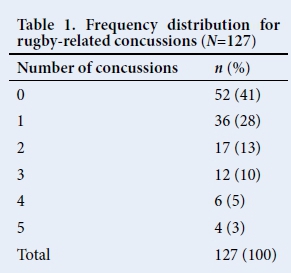
It is evident from Table 1 that the majority (59%) of the participants reported having suffered at least one concussion during their rugby playing careers. Furthermore, 31% indicated that they had been concussed on two or more occasions. Ten players (8%) reported suffering four or more concussions.
The level of concussion knowledge possessed by the subelite rugby union players participating in the study is reported in Table 2. These data are displayed for the sample as a whole, as well as for the previously concussed and non-concussed participants.
The data displayed in Table 2 indicate that correct response rates of 80% and above were recorded for four ofthe 13 concussion knowledge items. The vast majority of the respondents (95%) were aware that a concussion was a brain injury, 87% were aware that a previous concussion increased the risk of a player suffering a concussion in the future and 84% correctly indicated that concussion-related RTP decisions should be made by a medical doctor. Furthermore, 82% of the participants were aware that concussion can be present in the absence of positive neuroimaging findings.
The majority (78%) of the participants incorrectly believed that a scrum cap offers effective protection against concussion. Ninety-six (76%) of the players participating in the study believed that while a scrum cap would not completely prevent a concussion, it did serve a protective function. Only 21% of the sample correctly stated that a professional rugby player could only RTP once he had been cleared by a medical doctor. Most (58%) participants were of the opinion that a professional player who had suffered a concussion could play in the next match without being cleared by a medical doctor, provided the match was played at least 2 days after the incident in which he suffered the concussion. An additional 16% believed that this player could RTP during the same game in which the concussion had been suffered as long as he was cleared by the team's medical staff. Slightly less than half (46%) of the rugby players who participated in the study displayed inadequate knowledge relating to the range of activities that individuals recovering from concussion should avoid. Furthermore, only 61% of the sample identified concussion-related education as the most effective means of reducing the incidence of sport-related concussion. Developing strong neck muscles was viewed as the most effective means of reducing the risk of concussion by 13% of the sample, while 13% believed that proper stretching before and after exercise would be most effective, and 11% endorsed concussion education workshops for injured players as the most effective means of reducing the incidence of concussion.
An independent-samples t-test indicated no significant differencein the total concussion knowledge scores for the previously concussed participants (mean (SD), 9.6 (1.8)) and the non-concussed players (9.1 (2.1); t(125)=1.407, p=0.162). Generally the players who reported previously having suffered a concussion provided a higher proportion of correct answers on 8 of the 13 concussion knowledge items. Furthermore, a significantly larger proportion (χ2=4.757, p=0.029) of previously concussed players correctly identified tackles as the phase of play in which concussions were most frequently suffered.
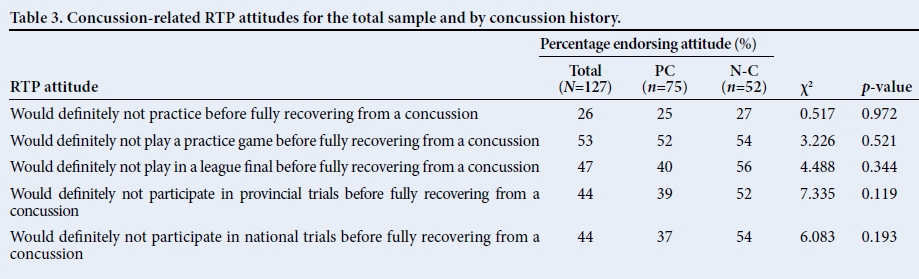
It is apparent from Table 3 that the rugby players participating in the study generally did not hold particularly conservative or cautious attitudes with respect to returning to practice and competition after a concussion. Only 26% indicated that they would definitely not return to practice before having fully recovered from a concussion. Slightly fewer than half of the participants indicated that they would definitely not play in a league final (47%), participate in provincial trials (44%) or play in national trials (44%) before having fully recovered from a concussion. However, 53% indicated that they would definitely not play in a practice match before fully recovering.
The data displayed in Table 3 suggest that the players with no reported history of concussion tend to be slightly more cautious in their concussion-related RTP attitudes when compared to players with a history of concussion. However, no statistically significant differences were apparent between the two groups with regard to the individual concussion-related RTP scenarios (practice, friendly, league final and trials). Moreover, an independent-samples i-test revealed no significant difference in the mean concussion-related RTP attitudes for the previously concussed participants (15.1 (4.2)) and the non-concussed players (16.1 (4.4); t(125)=-1.206, p=0.230).
Discussion
The objective of this study was to determine the concussion knowledge and concussion-related RTP attitudes of subelite rugby union players. While not a primary objective of the research, data were also gathered with regard to self-reported lifetime incidence of rugby-related concussion. The incidence of concussion reported by the rugby union players in this study indicates that more than half the sample had suffered at least one concussion and almost a third had been concussed on two or more occasions. It is conceded that the primary objective of this study was not to determine the incidence of concussion among subelite rugby players. Consequently, the reported incidence of concussion should be viewed circumspectly, not least as a result of the methodological limitations with regard to determining the incidence of concussion in this study.
The participants displayed a relatively high level of knowledge with regard to what constitutes a concussion, the risk that a history of concussion holds with regard to future concussion, and the authority that should rest with medical doctors in clearing players to RTP following concussion. Participants in the current study demonstrated superior knowledge in this respect compared with that reported for Australian rules football and rugby league coaches and trainers in Australia.[14] The previously concussed players were also reasonably knowledgeable about the phase of play in which a concussion was most likely to be suffered. Moreover, these players were significantly more inclined to endorse the correct answer in this regard compared to those participants who had not previously been concussed. Similar, though not significant, differences were apparent between previously concussed players and players with no history of concussion with regard to knowledge of a loss of consciousness not being a prerequisite for the diagnosis of a concussion, as well as what constitutes adequate RTP guidelines for amateur players. These findings raise the possibility that some aspects of players' concussion knowledge are perhaps more a function of personal experience of having been concussed than of effective information dissemination and education.
In excess of a third of the participants did not view educational initiatives as the most effective means of reducing the incidence of concussion in rugby union. Similar to findings in other countries, not only are educational indicatives in SARU seemingly not having the desired impact, but a substantial proportion of subelite players do not view information dissemination initiatives as an effective means of reducing concussion rates.[12-14,17,21] Slightly more than half of the participants demonstrated adequate knowledge regarding the range of activities that players recovering from concussion should avoid, and the vast majority (79%) were of the opinion that professional players could RTP much faster than amateurs. Although the reasons for the latter view are not apparent, it is troubling that there appears to be a perception that players competing at higher levels are somehow less affected by concussion. Less than adequate knowledge regarding the activities recovering players should refrain from is perhaps further evidence of the work that still has to be done with regard to effectively disseminating RTP information at all levels of the game. In addition, the widely held misperception that a scrum cap provides protection against concussion also appears to suggest that accurate information is not reaching players. However, it is possible that this particular misperception might be more due to commercial product promotion than ineffective dissemination of information.
The concussion knowledge of the participants in this study seemingly failed to translate into appropriately cautious RTP attitudes. It is of particular concern that almost three-quarters of the participants indicated that they would, to some extent, be inclined to participate in a practice despite not having fully recovered from a concussion. This finding, along with less than half of the participants indicating that they would not participate in important matches or trials before having fully recovered from concussion, might at least partially result from the relatively low levels of knowledge regarding RTP guidelines reported earlier. Taken together, the findings with regard to RTP attitudes are consistent with other studies on concussion-related RTP.[11-14,21,22] Furthermore, the discrepancy between the participants' knowledge and their RTP attitudes suggests that knowledge alone is not sufficient to bring about attitudinal and behavioural change in this regard. It would be advisable for future initiatives to specifically target attitudes and motivation in addition to the existing information dissemination strategies.[23]
Study limitations
The current sample was drawn from only two metropolitan areas. Consequently, the findings cannot be reliably generalised beyond this specific geographical context. The methodology employed in the study is not appropriate for validly determining concussion incidence. This is primarily due to the fact that participant recall was relied upon rather than objective records of diagnosed concussions. In addition, participants were not provided with a definition of concussion in order to help them determine whether or not they may have been previously concussed. The findings relating to the incidence of concussion within the sample should thus be treated circumspectly.
No indication of concussion knowledge prior to the implementation of various SARU sanctioned educational initiatives could be found. As a result, the extent to which these initiatives have succeeded or failed in improving player knowledge could not be determined. Similarly, the items used to determine concussion knowledge were largely based on the general recommendations of the consensus statements on concussion in sport and do not necessarily provide a valid indication of the extent to which players have internalised the particular information communicated via the existing education programmes. Future research should ensure closer correlation between the information provided by these initiatives and the content of measures of player concussion knowledge.
Conclusion
The rugby union players participating in the current study displayed satisfactory knowledge of what constitutes a concussion, the risks associated with repeated concussion and certain aspects of concussion identification or diagnosis. They exhibited less adequate knowledge on the field-side management of players suspected of having a concussion and a low level of knowledge with respect to concussion-related RTP guidelines. In addition, concussion knowledge did not appear to be related to RTP attitudes. While current concussion education initiatives appear to have been partially successful, additional methods of facilitating attitudinal and behavioural changes need to be considered.
References
1. Hollis SJ, Stevenson MR, Mcintosh AS, et al. Incidence, risk, and protective factors of mild traumatic brain injury in a cohort of Australian non-professional male rugby players. Am J Sports Med 2009;37(12):2328-2332. [http://dx.doi.org/10.1177/0363546509341032] [ Links ]
2. Shuttleworth-Edwards AB, Noakes TD, Radloff SE, et al. The comparative incidence of reported concussions presenting for follow-up management in South African Rugby Union. Clin J Sports Med 2008;18(5):403-409. [http://dx.doi.org/10.1097/JSM.0b013e3181895910] [ Links ]
3. Viljoen W, Patricios J. Boksmart - implementing a National Rugby Safety Programme. Br J Sports Med 2012;46(10):692-693. [http://dx.doi.org/10.1136/bjsports-2012-091278] [ Links ]
4. Patricios JS, Kohler RMN, Collins RM. Sports-related concussion relevant to the South African rugby environment: A review. S Afr J Sports Med 2010;22(4):88-94. [ Links ]
5. Fuller CW, Raftery M, Readhead C, et al. Impact of the International Rugby Board's experimental law variations on the incidence and nature of match injuries in southern hemisphere professional rugby union. S Afr Med J 2009;99(4);232-237. [ Links ]
6. Haseler CM, Carmont MR, England M. The epidemiology of injuries in English youth community rugby union. Br J Sports Med 2010;44(15):1093-1099. [http://dx.doi.org/10.1136/bjsm.2010.074021] [ Links ]
7. Bailes JE. Sport-related concussion: What do we know in 2009 - A neurosurgeon's perspective. J Int Neuropsych Soc 2009;15(4);509-511. [http://dx.doi.org/10.1017/S1355617709090936] [ Links ]
8. Harmon KG, Drezner JA, Gammons M, et al. American Medical Society for Sports Medicine position statement: Concussion in sport. Br J Sports Med 2013;47(1):15-26. [http://dx.doi.org/10.113/bjsports-2012-091941] [ Links ]
9. McCrory P, Meeuwisse WH, Aubry M, et al. Consensus statement on concussion in sport: The 4th International Conference on concussion in sport held in Zurich, November 2012. Br J Sports Med 2013;47(5):250-258. [http://dx.doi.org/10.1136/bjsports-2013-092313] [ Links ]
10. International Rugby Board. International Rugby Board Strategic Plan 2010 - 2020. Dublin: International Rugby Board, 2010. [ Links ]
11. Hollis SJ, Stevenson MR, McIntosh AS, et al. Compliance with return-to-play regulations following concussion in Australian schoolboy and community rugby union players. Br J Sports Med 2012;46(10):735-740. [http://dx.doi.org/10.1136/bjsm.2011.085332] [ Links ]
12. Sye G, Sullivan SJ, McCrory P. High school rugby players' understanding of concussion and return to play guidelines. Br J Sports Med 2006;40(12):1003-1005. [http://dx.doi.org/10.1136/bjsm.2005.020511] [ Links ]
13. Sullivan SJ, Burne L, Choie S, et al. Understanding of sport concussion by parents of young rugby players: A pilot study. Clin J Sports Med 2009;19(3):228-230. [http://dx.doi.org/10.1097/JSM.0b013e318a41e43] [ Links ]
14. White PE, Newton JD, Makdissi M, et al. Knowledge about sports-related concussion: Is the message getting through to coaches and trainers? Br J Sports Med 2014;48(2):119-124. [http://dx.doi.org/10.1136/bjsports-2013-092785] [ Links ]
15. Johnson VE, Stewart JE, Begbie FD, et al. Inflammation and white matter degeneration persists for years after a single traumatic brain injury. Brain 2013;136(1):28-42. [http://dx.doi.org/10.1093/brain/aws322] [ Links ]
16. McKee AC, Stein TA, Nowinski CJ, et al. The spectrum of disease in chronic traumatic encephalopathy. Brain 2013;136(1):43-64. [http://dx.doi.org/10.1093/brain/aws307] [ Links ]
17. Jansen van Rensburg M. Concussion knowledge and practice among role players in primary school rugby in the North West Province. Unpublished Master's Dissertation. Bloemfontein: University of the Free State, 2013. [ Links ]
18. Brislin RW. Back-translation for cross-cultural research. J Cross-Cultural Res 1970;1(3):185-216. [ Links ]
19. Howell DC. Statistical Methods for Psychology. 8th ed. Belmont: Thomson Wadsworth, 2013. [ Links ]
20. IBM Corporation. IBM Statistics for Windows, Version 21.0. New York: IBM, 2012. [ Links ]
21. Kroshus E, Daneshvar DH, Baugh CM, et al. NCAA concussion education in ice hockey: An ineffective mandate. Br J Sports Med 2014;48(2):135-140. [http://dx.doi.org/10.1136/bjsports-2013-092498] [ Links ]
22. Provvidenza C, Engebretsen L, Tator C, et al. From consensus to action: Knowledge transfer, education and influencing policy on sports concussion. Br J Sports Med 2013;47(5):332-338. [http://dx.doi.org/10.1136/bjsports-2012-092099] [ Links ]
23. Barkoukis V, Lazarus L, Tsorbatzoudis H, Rodafinos A. Motivational and sportspersonship profiles of elite athletes in relation to doping behaviour. Psychol Sport Exerc 2011;12(3):205-212. [http://dx.doi.org/10.1016/j.psychsport.2010.10.003] [ Links ]
Corresponding author: SP Walker (walkersp@ufs.ac.za)


{kind=link}
{kind=link}