










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Journal of Sports Medicine
versão On-line ISSN 2078-516X
versão impressa ISSN 1015-5163
SA J. Sports Med. vol.26 no.2 Bloemfontein 2014
http://dx.doi.org/10.7196/SAJSM.513
ORIGINAL RESEARCH
Effect of caffeine ingestion on fluid balance during exercise in the heat and during recovery
Y ZhangI; S J CarterV; R E SchumackerII; Y H NeggersIII; M D Curtner-SmithVI; M T RichardsonI; J M GreenIV; P A BishopVI
IPhD; Department of Kinesiology, University of Alabama, Tuscaloosa, USA
IIPhD; Department of Educational Studies in Psychology, Research Methodology, and Counseling, University of Alabama, Tuscaloosa, USA
IIIPhD; Department of Human Nutrition, University of Alabama, Tuscaloosa, USA
IVPhD; Department of Health, Physical Education, and Recreation, University of North Alabama, Florence, USA
VMSc; Department of Kinesiology, University of Alabama, Tuscaloosa, USA
VIEdD; Department of Kinesiology, University of Alabama, Tuscaloosa, USA
ABSTRACT
BACKGROUND: The effect of ingestion of a common stimulant, caffeine, on fluid balance during exercise and recovery is not fully known.
OBJECTIVES: To determine the effect of caffeine on fluid balance during exercise in the heat and during a 3-hour recovery period thereafter.
METHODS: In a randomised, controlled design, caffeine-naive participants (N=8) pedalled on a bike to achieve 2.5% baseline body mass loss in a hot environment in four separate conditions: with (C+) or without (C-) caffeine ingestion (6 mg/kg of body mass) prior to exercise, followed by (W+) or without (W-) 100% fluid replenishment (water) of the body mass loss during a 3-hour recovery period (yielding C+W+, C+W-, C-W+ and C-W-, respectively).
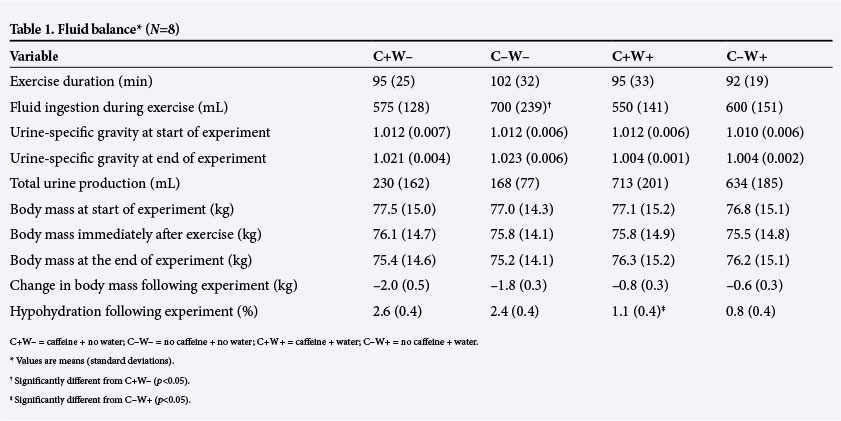
RESULTS: Mean (standard deviation) urine production was not different (p>0.05) regardless of rehydration status: 230 (162) mL (C+W-) v. 168 (77) mL (C-W-); and 713 (201) mL (C+W+) v. 634 (185) mL (C-W+). For the 3-hour recovery, caffeine ingestion caused higher hypohydration during rehydration conditions (p=0.02), but practically the mean difference in the loss of body mass was only 0.2 kg.
CONCLUSION: In practical terms, there was no evidence that caffeine ingestion in moderation would impair fluid balance during prolonged exercise in the heat or during 3 hours of recovery.
Current military doctrine places operational forces in unique situations in which soldiers are often engaged in sustained activities to achieve mission objectives. Since modern military operations are both physically and cognitively demanding, and recovery can often be inadequate, there has been an increased interest in caffeine as an effective dietary supplement to counter performance deficits in military settings.[1] The use of caffeine to extend operational effectiveness in military settings is likely to be encouraged.[2]
Athletes have been advised to abstain from caffeine because of its diuretic effect.[3] A review by Maughan and Griffin[4] suggests that acute ingestion of caffeine (e.g. >250 mg) results in a short-term stimulation of urine production. Meanwhile, caffeinated beverages have been reported to increase urine production during post-exercise rehydration.[5] Opposing this viewpoint, Armstrong[6] concluded that the diuretic effect of caffeine is overstated and further may be minimised for habitual caffeine consumers. In support of this view, Armstrong et al.[7]provided strong evidence for no caffeine-induced diuresis (<500 mg/24 hours) in males undergoing daily activities with no strenuous physical training.
Possibilities of detrimental fluid imbalances are unlikely since caffeine consumption is generally moderate and accompanied by adequate access to fluid, making rehydration non-problematic. For soldiers in combat, the risk of dehydration is higher due to prolonged operations and limited fluid availability in challenging environments, which may lead to serious health-related consequences and affect mission success. To provide more accurate information on prescribing caffeine consumption for operational forces in hot environments, this study was designed to evaluate the influence of moderate caffeine ingestion on fluid balance during exercise and recovery. We hypothesised that fluid balance would not be affected despite caffeine ingestion. Repeated prolonged operations in hot environments with restricted fluid availability represent a real-life military scenario. The findings thus have important implications for military forces engaging in sustained operations in the heat, and the results can be extended for athletes competing in adventure sports, ultradistance, and multiday sport events, and occupational workers who often consume coffee or caffeinated beverages.
Methods
Subjects
Eight healthy male university students volunteered for the study. All participants were physically active (e.g. exercised >4 days/ week). Mean (standard deviation (SD)) age, height and body mass were 23 (4) years, 178 (4) cm and 77 (15) kg, respectively. The physical characteristics are similar to the 50th percentile means in the US Army's anthropometric database.[8] A questionnaire was administered to determine average daily caffeine consumption. Only those who regularly consumed <50 mg of caffeine per day were recruited in order to create an extreme-end pattern, since a caffeine-naive population is believed to be more responsive to the effects of caffeine ingestion on fluid balance.[6] The study was approved by the local Medical Ethics Committee. Prior to beginning the study, participants were briefed on potential risks, and they signed a written informed consent form, completed a medical history questionnaire, and were acclimated to the biking exercise in the heat.
Procedure and design
A randomised, repeated-measures design was used. Each participant completed four trials: (i) exercise with caffeine (C+), (ii) exercise with no caffeine (C-), (iii) recovery-phase rehydration with tap water equal to 100% of the body mass loss (adjusted by fluid ingestion, see below) during the exercise phase (W+), and (iv) no rehydration during the recovery phase (W-), thus yielding C+W+, C-W+, C+W- and C-W-. Each trial consisted of two phases: (i) exercise-heat exposure (adjusted by fluid ingestion during exercise: 2.5% baseline body mass loss = body mass at the beginning of exercise - body mass at the end of exercise + total volume of fluid ingested during exercise = 100% fluid replenishment during recovery), immediately followed by (ii) a 3-hour recovery in a temperate environment.
For a given participant, each trial was performed at the same time of day on the same day of week so that fatigue and circadian influences on hormonal secretion were minimised. Participants were instructed to refrain from any caffeinated product or alcohol for a minimum 24-hour period prior to testing.
Participants were instructed to drink a bottle of fixed volume (~500 mL) of water before sleep prior to the experiment day and another bottle of fixed volume (~500 mL) of water 2 hours before reporting to the lab to maintain a state of euhydration. On arrival at the laboratory, participants emptied their bladder and provided a urine sample, and body mass was measured (with dry polyester shorts only) (accuracy ~0.1 kg; Detecto Scales Inc, USA). To confirm the hydration status, urine specific gravity was determined with a refractometer (SUR-NE, Atago Inc, USA); a urine specific gravity <1.020 indicated euhydration.[9] If participants measured >1.020, they were asked to come back a week later.
For the caffeine trials, 10 minutes prior to the exercise phase participants consumed caffeine capsules equal to 6 mg/kg of baseline body mass. This dosage has been suggested to be effective in enhancing physical endurance in caffeine-naive and habitual users.[2] Then participants entered an environmental chamber (dry bulb 42oC, wet bulb 31oC, globe 40oC, relative humidity ~40%) and dehydrated to 2.5% baseline body mass loss through cycle ergometry (824E, Monark, Sweden). They were asked to cycle at a pace maintaining Borg's rating of perceived exertion at 12 - 13, which is classified as moderate intensity.[10]
Participants were allowed to drink bottled tap water within a fixed volume equivalent to 400 mL/hour to simulate limited fluid availability during military operations. The bottle was refilled every 60 minutes by the investigators. Total fluid ingestion during this phase was recorded. This drinking pattern was similar to the volume that would adequately replace body water loss during a 4-hour military march in a temperate environment.[11] Body mass (weighed with towel-dried polyester shorts only) was checked routinely. Once the desired body mass loss was attained, participants were removed from the chamber.
Three hours of recovery immediately followed the exercise phase. The mean ambient temperature during recovery was 21.0 (0.5)°C and relative humidity was 45 (4)%. Participants were instructed not to eat and to maintain a light metabolic status (e.g. reading a book, browsing the internet) throughout this period.
For the two trials with fluid replenishment during the 3-hour recovery phase, a volume of tap water equivalent to 100% of the body mass loss was ingested during the first 2 hours of the recovery phase. Rehydration was performed as a metered fluid ingestion (25% of volume ingested every 30 minutes for 2 hours), aiming for greater hydration efficiency.[12] This rehydration also enhances ecological validity where soldiers are more likely to replace water conservatively in case of limited fluid availability. Following the 3-hour recovery, participants were weighed again (with dry polyester shorts only).
Statistical analysis
Since it is known that water ingestion exerts a mild diuretic effect,[13] all data analyses were performed for the main effect of caffeine ingestion within the rehydration or non-rehydration trials. Pairwise t-tests were used to compare experimental variables. Water loss (i.e. sweating and respiration) during the 3-hour recovery phase was calculated as follows: body mass (immediately after exercise phase) + 100% fluid replenishment (for W trials) - body mass (end of experimental trial) - total urine production.
The percentage (distribution) of fluid replenishment (for W trials) represented the amount of ingested fluid during recovery that was either retained in the body, or had been lost in the form of urine or by means of sweating and respiration at the end of the 3-hour recovery phase. For example, water retention ratio was calculated as follows: (body mass (end of experimental trial) - body mass (immediately after exercise phase)) / 100% fluid replenishment χ 100%.
To determine the responders and non-responders to caffeine treatment, individual data (total urine production) were also compared by computing the least mean difference, yielding a p<0.05 at a power of 80% using the mean observed SD. All data were reported as means (SDs). Differences were considered to be significant at a p<0.05 level.
Results
Mean (SD) caffeine ingestion was 463 (89) mg and 459 (84) mg (range 350 - 600 mg), for C+W- and C+W+, respectively. No participant urinated during the exercise phase, nor defecated or vomited during the entire experimental period.
Urine production is given in Table 1. No detectable difference was observed following caffeine ingestion (p>0.05). Comparing the C+ with C- trials, there was no difference (p>0.05) in body mass or urine specific gravity between the start of the exercise phase and the end of the experimental trials (Table 1). For the W- trials, fluid ingestion during the exercise phase was significantly different (p=0.03). For the W+ trials, caffeine ingestion caused a significant difference (p=0.02) in hypohydration (Table 1).
Fig. 1 shows the relative fluid distribution following the 3-hour rehydration phase. Mean (SD) water loss was no different for C+W+ (0.7 (0.4) kg) v. C-W+ (0.5 (0.3) kg) (p=0.08). However, water retained in the body was significantly lower in C+W+ (0.5 (0.4) kg) v. C-W+ (0.7 (0.3) kg) (p=0.006).
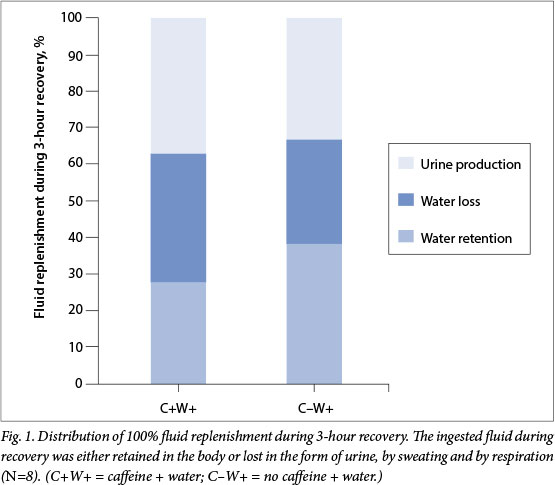
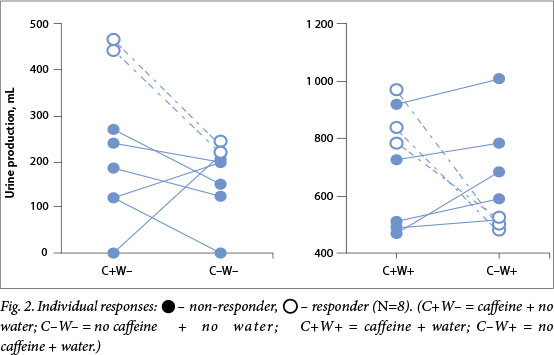
Accordingly, the water retention ratio was greater in C-W+ (38 (12)%) v. C+W+ (27 (16)%) (p=0.01). Individual analysis (Fig. 2) detected that two participants were sensitive to caffeine treatment for the no fluid replenishment conditions, and three participants were sensitive to caffeine treatment for the 100% fluid replenishment conditions.
Discussion
The objective of the study was to determine the impact of caffeine on fluid balance during exercise and recovery. Urine production was not different despite caffeine ingestion when no fluid replenishment was present; moreover, even with 100% fluid replenishment (water) during recovery, which is considered to be diuretic and suppressive of fluid-regulating hormones,[13] there were no treatment differences after a 3-hour recovery. Current results provide additional supportive evidence that caffeine would not compromise fluid balance during and after exercise.[7,14-16]
Early literature has suggested that caffeine ingestion exceeding a threshold of 250 - 300 mg could result in an acute increase in urine production.[4] Our results suggested that a mean dose of 460 mg caffeine (6 mg/kg of body mass) - enough to enhance physical and cognitive performance[2] - did not alter urine production. This supports previously reported data. In a study with a caffeine dose similar to that of our study (5 mg/kg ofbody mass; mean 553 mg), participants exercising at 70 - 75% maximal oxygen uptake to exhaustion did not experience extra urine production compared with non-caffeine conditions.[15] Likewise, following cycling exercise, a moderate dose of 320 mg of caffeinated drinks did not induce additional acute body water loss compared with no caffeine.[16] The influence of exercise on the diuretic effect of caffeine is further evidenced by a study that showed that a large dose of caffeine (8.7 mg/kg of body mass; mean 586 mg) exerted a diuretic effect at rest but not during exercise.[17] This suggests that exercise is a mediating factor on caffeine-induced diuresis in healthy young males.
The mean duration for the dehydration exercise phase was 1.5 hours. The effective window of time for the diuretic effect of caffeine totalled 4.5 hours in this study. A data-collection period <6 hours is often considered to cover an acute response to caffeine, and previous research has questioned whether or not such an acute response could be generalised to real-life applications.[18] While we could not totally rule out that body water loss (e.g. due to further urine production) may still occur at 6 hours, 12 hours, or after longer time periods after caffeine ingestion, it is our opinion that the current protocol duration would representatively depict a clear picture of the effect of caffeine on fluid balance under the test conditions. First, it is known that the half-life of caffeine is 2.5 - 4.5 hours in young individuals,[19] and neither exercise nor additional thermal stress should affect its pharmacokinetics.[20] The current 4.5-hour data collection was long enough for caffeine to exert diuretic effect. Second, the literature generally suggests that the diuretic effect of caffeine starts quickly and slows later.[21] We believe that if there were a strong diuretic effect of caffeine, such an effect should override the effect of exercise during this 4.5-hour data-collection period, which did not occur in our results. Furthermore, studies with either a 16-hour[14] or 24-hour[7] data-collection period with a moderate dose of caffeine (6 mg/kg of body mass) did not reveal any further diuretic effect during free-living conditions. Exercise alone, or in combination with heat, could sufficiently defend total body fluid regulation even with moderate caffeine ingestion.
Data suggested that hypohydration was significantly higher with caffeine ingestion during rehydration trials. Statistically, the 1.1 (0.4)% of dehydration for C+W+ was higher (p<0.05) compared with 0.8 (0.4)% for C-W+; biologically, however, the mean difference in body mass loss was only 0.2 kg between the two rehydration trials. We consider this statistical difference to have resulted from the difference in water loss. We rigorously controlled the 3-hour recovery phase; however, the water loss for C+W+ (0.7 (0.4) kg) tended to be higher (p=0.08) than in C-W+ (0.5 (0.3) kg), which is inconsistent with the calculated water loss of 0.4 (0.3) kg for C+W- and 0.4 (0.2) kg for C-W-. Considering that urine production was similar between the two rehydration trials, the difference in water loss explained the higher water retention ratio found in C-W+.
Caffeine has known thermoregulatory effects. For example, it has been reported that 200 mg ingested caffeine increased metabolic rate by an average of 7% up to 3 hours after consumption.[22] It is possible that in some trials, participants (e.g. C+W+) were hotter (rectal temperature was continuously monitored for safety purposes but was not recorded for data analysis in the study) and metabolically more active for longer as a result of the thermoregulatory effect of caffeine; consequently the participants continued to sweat after the body mass was taken (at the end of the exercise phase), resulting in the differences seen in water loss and potentially impacting the water retention. This statistical significance leads to a conclusion that caffeine ingestion would increase hypohydration and fluid requirements during the rehydration conditions; however, such biological difference was minimal (~200 mL) and probably would not affect overall health and performance in practical terms. In addition, these participants were selected because they did not routinely ingest large quantities of caffeine, and thus should represent a worst-case condition.
For a broader view, we also analysed individual responses (total urine production) to the caffeine treatment (Fig. 2). There was some evidence within our study's caffeine-naive population to show that some individuals were less tolerant to caffeine. This interindividual inconsistency was probably due to the metabolism of caffeine, which is influenced by lifestyle factors and human genetic variation. Caffeine is metabolised in the liver by the hepatic enzyme system; the main enzyme in this process is cytochrome P450 1A2 (CYP1A2).[23] Drug intake, body composition, smoking and other lifestyle factors can affect hepatic CYP1A2 activity by different magnitudes.[23] Additionally, there is substantial evidence that hepatic CYP1A2 has a high rate of genetic variation, which could lead to a high degree of variability in the metabolism of caffeine. [24] These observations support our hypothesis, and it should also be noted that whereas the means were no different, individual responses were present and the impact on hydration status could be case by case.
Conclusion
Our study simulated an environmental challenge that military forces may encounter in hot climates and has the potential for generalisation to the military community. We found moderate caffeine ingestion (mean 460 mg) did not alter urine production during and after exercise. In practical terms, caffeine ingestion did not impact the fluid balance after exercise-heat exposure. These findings would imply that the use of caffeine in moderation (e.g. 3 - 4 cups of regular, brewed coffee, 150 mg caffeine per 150 mL) preceding exercise would not place healthy young individuals at higher risk of hypohydration. In light of the positive effects of caffeine on physical and cognitive performance, there is no reason for restricting regular coffee consumption for modern military operations in the heat.
Acknowledgements. We thank the study participants.
References
1. McLellan TM, Kamimori GH, Voss DM, et al. Caffeine maintains vigilance and improves run times during night operations for Special Forces. Aviat Space Environ Med 2005;76(7):647-654. [ Links ]
2. Committee on Military Nutrition Research, Food and Nutrition Board, Institute of Medicine. Caffeine for the sustainment of mental task performance: Formulations for military operations. Washington, USA: National Academy Press, 2001:79-96. [ Links ]
3. Sinclair C, Geiger J. Caffeine use in sports. A pharmacological review. J Sports Med Phys Fitness 2000;40(1):71-79. [ Links ]
4. Maughan RJ, Griffin J. Caffeine ingestion and fluid balance: A review. J Hum Nutr Diet 2003;16(6):411-420. [ Links ]
5. Gonzalez-Alonso J, Heaps CL, Coyle EF. Rehydration after exercise with common beverages and water. Int J Sports Med 1992;13(5):399-406. [ Links ]
6. Armstrong LE. Caffeine, body fluid-electrolyte balance, and exercise performance. Int J Sport Nutr Exerc Metab 2002;12(2):189-206. [ Links ]
7. Armstrong LE, Pumerantz AC, Roti MW, et al. Fluid, electrolyte, and renal indices of hydration during 11 days of controlled caffeine consumption. Int J Sport Nutr Exerc Metab 2005;15(3):252-265. [ Links ]
8. Gordon CC, Churchill T, Clauser CE, McConville JT. Anthropometric survey of US army personnel: Methods and summary statistics, 1988. Natick: DTIC Document, 1989:62. [ Links ]
9. Armstrong LE, Soto JA, Hacker FT Jr, et al. Urinary indices during dehydration, exercise, and rehydration. Int J Sport Nutr 1998;8(4):345-355. [ Links ]
10. Borg GA. Psychophysical bases of perceived exertion. Med Sci Sports Exerc 1982;14(5):377-381. [ Links ]
11. Nolte H, Noakes TD, Van Vuuren B. Ad libitum fluid replacement in military personnel during a 4-h route march. Med Sci Sports Exerc 2010;42(9):1675-1680. [http://dx.doi.org/10.1249/MSS.0b013e3181d6f9d0] [ Links ]
12. Jones EJ, Bishop PA, Green JM, et al. Effects of metered versus bolus water consumption on urine production and rehydration. Int J Sport Nutr Exerc Metab 2010;20(2):139-144. [ Links ]
13. Melin B, Koulmann N, Jimenez C, et al. Comparison of passive heat or exercise-induced dehydration on renal water and electrolyte excretion: The hormonal involvement. Eur J Appl Physiol 2001;85(3-4):250-258. [http://dx.doi.org/10.1007/s004210100448] [ Links ]
14. Dias JC, Roti MW, Pumerantz AC, et al. Rehydration after exercise dehydration in heat: Effects of caffeine intake. J Sport Rehabil 2005;14(4):294-300. [ Links ]
15. Falk B, Burstein R, Rosenblum J, et al. Effects of caffeine ingestion on body fluid balance and thermoregulation during exercise. Can J Physiol Pharmacol 1990;68(7):889-892. [ Links ]
16. Kovacs EM, Stegen J, Brouns F. Effect of caffeinated drinks on substrate metabolism, caffeine excretion, and performance. J Appl Physiol 1998;85(2):709-715. [ Links ]
17. Wemple R, Lamb D, McKeever K. Caffeine v. caffeine-free sports drinks: Effects on urine production at rest and during prolonged exercise. Int J Sports Med 1997;18(1):40-46. [ Links ]
18. Armstrong LE, Casa DJ, Maresh CM, et al. Caffeine, fluid-electrolyte balance, temperature regulation, and exercise-heat tolerance. Exerc Sport Sci Rev 2007;35(3):135-140. [http://dx.doi.org/10.1097/jes.0b013e3180a02cc1] [ Links ]
19. Massey LK. Caffeine and the elderly. Drug Aging 1998;13(1):43-50. [ Links ]
20. McLean C, Graham TE. Effects of exercise and thermal stress on caffeine pharmacokinetics in men and eumenorrheic women. J Appl Physiol 2002;93(4):1471-1478. [http://dx.doi.rg/10.1152/japplphysiol.00762.2000] [ Links ]
21. Neuháuser-Berthold M, Beine S, Verwied SC, et al. Coffee consumption and total body water homeostasis as measured by fluid balance and bioelectrical impedance analysis. Ann Nutr Metab 1997;41(1):29-36. [ Links ]
22. Koot P, Deurenberg P. Comparison of changes in energy expenditure and body temperatures after caffeine consumption. Ann Nutr Metab 1995;39(3):135-142. [ Links ]
23. Magkos F, Kavouras SA. Caffeine use in sports, pharmacokinetics in man, and cellular mechanisms of action. Crit Rev Food Sci Nutr 2005;45(7-8):535-562. [http://dx.doi.org/10.1080/1040-830491379245] [ Links ]
24. Daly AK. Genetic polymorphisms affecting drug metabolism: Recent advances and clinical aspects. Adv Pharmacol 2012;63:137-167. [http://dx.doi.org/10.1016/B978-0-12-398339-8.00004-5] [ Links ]
 Correspondence:
Correspondence:
Y Zhang
dr.zhang.yang@qq.com


{kind=link}