










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Sports Medicine
On-line version ISSN 2078-516X
Print version ISSN 1015-5163
SA J. Sports Med. vol.26 n.1 Bloemfontein 2014
http://dx.doi.org/10.7196/SAJSM.482
ORIGINAL RESEARCH
Common acute and chronic musculoskeletal injuries among female adolescent field hockey players in KwaZulu-Natal, South Africa
T J EllapenI; K BowyerII; H J van HeerdenIII
IPhD; Department of Sport Science, School of Physiotherapy, Sport Science and Optometry, University of KwaZulu-Natal, Durban, South Africa
IIBSps (Hons) (Biokinetics); Department of Sport Science, School of Physiotherapy, Sport Science and Optometry, University of KwaZulu-Natal, Durban, South Africa
IIIDPhil; Department of Sport Science, School of Physiotherapy, Sport Science and Optometry, University of KwaZulu-Natal, Durban, South Africa
ABSTRACT
OBJECTIVE: To document the prevalence and nature of musculoskeletal injuries among female adolescent hockey players over a 12-month period (1 November 2011 - 31 October 2012).
METHODS: Data were collected from 148 high school players who belonged to the KwaZulu-Natal Hockey League via voluntary, parental-informed consent. Players completed a self-report musculoskeletal questionnaire probing the prevalence and nature of acute and chronic injuries. Probability was set at p<0.05.
RESULTS: Ninety-four players sustained acute musculoskeletal injuries in the 12-month study period, indicating the knee (23%) and lower back (18%) to be the most prevalent sites of injury (p<0.001). The mechanisms producing the acute injuries were rapid rotational movement (36%) and physical trauma (63%) (p<0.05). The hip/lower back was the most prevalent anatomical site of chronic musculoskeletal injury (p<0.001). The intrinsic factors predisposing players to chronic hip/lower-back injury were hip flexion contractures and posture (p<0.05).
CONCLUSION: Hockey players experience a high prevalence of acute musculoskeletal knee injuries and chronic hip/lower-back injuries. The hockey fraternity should be educated about the various ways in which to prevent injury by complying with appropriate training regimes, alterations in technique and stretching exercises.
Hockey has become a popular international sport at girls' high schools, resulting in the formation of many school leagues.[1] In South Africa, netball is the most popular sport for girls at schools, followed by hockey and swimming.[2] Hockey is a dynamic and competitive sport that frequently produces musculoskeletal injuries, which can be classified into acute and chronic.[1,3] However, there is limited research in field hockey injuries. Acute musculoskeletal upper-extremity injuries include acromioclavicular ligament sprains and dislocations, scaphoid fractures and game keeper's thumb, while widespread facial injuries are black eye, tooth dislocation and fractures, bone fractures and blindness.[3,4] Dick et al.[3]reported that the majority of field hockey musculoskeletal injuries are to the lower extremities and include lateral ankle sprains, meniscal tears, tibiofemoral ligament sprains, tibia and fibula fractures, and hip flexor, adductor, quadriceps and hamstring strains. The predisposing mechanisms of acute hockey musculoskeletal injures are physical trauma (collision with the ball, stick and other players) and rapid rotational movements.[3,5,6] Field hockey players aged 10 - 19 years sustain a high prevalence of musculoskeletal injuries.[1] Sherker and Cassell[1] and Lindgren and Maguire[6] reported that young female players sustain an average of 5.0 injuries per player, in contrast to 3.1 injuries per male player.
Chronic musculoskeletal injuries are localised to the lower back and shoulder, with the predisposing mechanism undetermined.[3] Murtaugh[4] hypothesised that the semi-crouched posture adopted by hockey players is the culprit of chronic hip/lower-back injuries.
This was later supported by a similar postulation by Ellapen et al.[7] among elite players. Intrinsic factors predisposing players to chronic musculoskeletal injuries are undetermined. There has only been one study that examined the relationship between postural alignment and chronic musculoskeletal injuries among elite hockey players.[7] There is also controversy regarding which hockey playing position is most vulnerable to musculoskeletal injuries. Murtaugh'41 reported that midfielders experience the most injuries, while Ellapen et al.[7] contended that strikers are most vulnerable to injury.
We examined the relationships between hip flexor contractures, postural analyses, chronic musculoskeletal injuries, anatomical site of injury and the vulnerability of positional play.
Methods
One hundred and forty-eight female hockey players participated in a retrospective musculoskeletal injury investigation by voluntary, parental-informed consent. The average amount of hockey experience was 8.4 years (standard deviation (SD) ±2.3). Ethical approval was obtained from the School of Health Sciences Research Committee, University of KwaZulu-Natal (SHSEC026/12). The players belonged to the KwaZulu-Natal (KZN) Hockey School League, which extends from the urban eThekwini schools to the peri-urban and rural Umgungu-ndlovu District schools, thus providing a cross-sectional overview of the nature of common musculoskeletal hockey injuries. There were seven schools participating in this league. Each school fielded two teams of14 players. The sample was 75.5% representative of the total number of league players, which is higher than the 30% statistical rule of thumb pertaining to the minimum percentage of subjects participating in a study, yielding power of significance.[8] In terms of inclusion criteria, players had to be registered female pupils of one of the seven schools that participated in the league, and aged 13 - 18 years.
The study addressed: demographic details (age, body mass and stature), training regime, anatomical site of musculoskeletal pain, severity of pain, type of pain and predisposing mechanism of injury.
Each player's history of acute and chronic hockey musculoskeletal injuries was obtained with a self-report questionnaire adapted from Ellapen et al.[7] and Kee and Seo.[9] Players were requested to indicate only hockey musculoskeletal injuries, and not musculoskeletal injuries contracted from other sports or recreational activities. Acute musculoskeletal injury was defined as a sensation of distress or agony that prevented a player from physical activity for a minimum period of 24 hours due to a specific predisposing mechanism of injury (adapted from Van Heerden[10]). Pain was surveyed because it is a discernible symptom of musculoskeletal injury. Chronic musculoskeletal injuries were characterised by insidious, persistent musculoskeletal pain, without the identification of a specific predisposing mechanism of injury, that endured for a minimum of 6 months. Players were requested to report separately on the two types of injury.
The questionnaire was divided into four parts: anatomical site of the musculoskeletal pain; severity of the associated pain according to the Kee and Seo[9] pain-rating scale; type of hockey musculoskeletal injury symptoms (dull aching, discomfort, sharp, pins and needles, numbness, burning and radiating); and the predisposing mechanism ofthe acute musculoskeletal injuries.[9] Hagglund et al.[11]reported that the fundamental problem concerning international epidemiological sport investigations is the inconsistent definition of musculoskeletal injury. They proposed that the prevalence of musculoskeletal injury can be established if the following is documented: anatomical site of musculoskeletal pain; type of musculoskeletal pain sustained; and severity of pain, measured by a validated pain-rating scale.[11] The questionnaire was translated from English into isiZulu and Afrikaans. Each player was interviewed, during which time they completed the questionnaire. The interviewer was a graduate student who was thoroughly grounded in the research protocol and fluent in English, Afrikaans and isiZulu.
In addition to the musculoskeletal injury questionnaire, postural analyses and hip flexion contracture (Thomas test) were recorded. The postural analyses (Kendall et al.[12] postural profile protocol) were conducted to determine any association between static vertebral misalignment and hip/lower-back musculoskeletal injury. The Thomas test (Kendall et al.[l2]protocol) was performed to determine whether there was a significant relationship between hip flexor contracture and chronic lower-back musculoskeletal injury.
Postural analyses
Players stood against a posture profile chart in anatomical position in both the frontal and sagittal planes. The plumb line represented the line of centre, dividing the body equally into right and left when the player stood in the frontal plane. The spinous process of the vertebrae was marked to indicate lateral deviation from the plumb line in this position, thereby identifying the presence of scoliosis - lateral curvature of the spine, which may be due to neuromuscular, degenerative, congenital or idiopathic causes.[12] Similarly, the line of centre divided the body anteriorly and posteriorly with the player standing in the sagittal plane. The line of centre passes through the auditory meatus, acromion process, anterior sacro-iliac crest (ASIS), behind the patella and in front of the lateral malleolus (when analysing posture in the sagittal plane). Forward displacement ofthe acromion process and excessive flexion of the thoracic vertebrae in the sagittal plane was used to indicate kyphosis - excessive curvature of the thoracic vertebrae due to neuromuscular, degenerative, congenital, trauma or idiopathic causes.[12] Anterior deviation of the ASIS away from the line of centre in the sagittal plane was used to indicate anterior pelvic tilt, which places compressive stress on the posterior elements of the spine.[12] The postural profiles were statistically correlated to chronic musculoskeletal injury.
Thomas test
The player lay supine on a plinth with their knees bent and the lower limb hanging over the edge of the plinth, and their posterior thighs lying against the surface of the plinth. The greater trochanter and lateral femoral condyle of the ipsilateral leg were identified, and a line was drawn between these two landmarks. The first clinician aligned the stationary arm of the goniometer onto the greater trochanter and the line drawn of the ipsilateral thigh. The second clinician passively flexed the contra-lateral hip, bringing the knee to the chest (with the contra-lateral hip and knee flexed). The movable arm of the goniometer was then aligned to the drawn line of the ipsilateral thigh as the contra-lateral hip was flexed. The angle created by the intersection of the stationary and movable lines was measured. Three readings were taken for each player by the same clinician (to ensure test/re-test reliability) and analysed with respect to chronic hip/lower-back musculoskeletal injury. The hip flexion angle is indicative of hip flexion contracture.
Statistical analyses
The cohort was described using modes, means, frequencies and percentages. Data were analysed by inferential statistical analysis using χ2 tests and two-tailed t-tests adjusted for unequal variance (p<0.05) Levene's test was used to assess homogeneity variance, and indicated unequal variance (p<0.05).
Results
The 148 players had a mean±SD age of 15.4±0.4 years, body mass of 54.7±4.4 kg and stature of 1.58±0.01 m. The cohort included 117 white (79%), 22 black (15%), 6 coloured (4%) and 3 Indian (2%) participants. The mean±SD number of years of playing experience was 7.8±0.7.
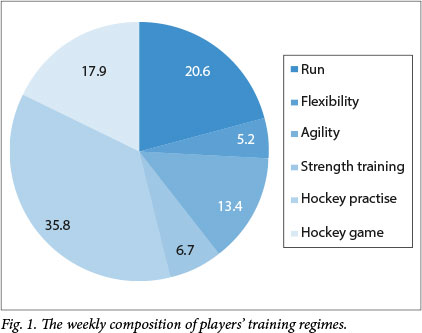
Players practised an of average 7.8±2.5 months/year and 2.9±1.0 days/week. Hockey exposure included practise, training sessions and game time. The composition of the players' weekly training regimes (Fig. 1) included 2.5±1.7 days/week of cross-training.
Of the players, 64% experienced acute musculoskeletal injuries (p<0.001), the most prevalent sites being the knee (23%), lower back (18%) and ankle (15%) (p<0.001) (Table 2). These three injury sites accounted for 56% of all acute musculoskeletal injuries.
The Kee and Seo[9] pain-rating scale, ranging from 1 to 5, was used to determine the severity of musculoskeletal pain experienced. A score of 3 (moderate pain intensity) was rated the most prevalent (44%), followed by a score of 4 (severe pain intensity) (43%), 2 (mild intensity pain) (4%), 5 (worst pain ever experienced) (2%) and 1 (no pain) (2%) (p<0.001). The most commonly reported symptoms of acute musculoskeletal injury were sharp (38%), discomfort (21%), dull aching (17%), burning (4%), radiating (2%), numbness (2%), pins and needles (2%) and swelling (1%) (p<0.001). The combination of the anatomical site of musculoskeletal pain, severity of the musculoskeletal pain and the identification of the type of pain sensation experienced indicated the prevalence of hockey musculoskeletal injuries.
The predisposing mechanisms of acute hockey musculoskeletal injuries were rapid rotational movement (37%) and direct physical trauma (63%) (p<0.05). Physical trauma was further categorised into: struck with a ball (44%), struck with a stick (20%), and colliding with another player (36%).
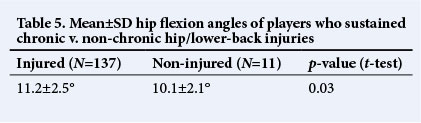
Regarding chronic injuries, 137 players experienced persistent, mild pain (pain rating score of2) in their hip/lower back without remembering any specific event predisposing to injury. Having identified an accumulative 387 chronic injuries in 137 players, a comparative analysis between those with and without injuries was done with regards to their posture and hip flexor contracture (Table 5).
Discussion
The results are discussed as follows: demographic details; training regime; acute musculoskeletal injuries; and chronic musculoskeletal injuries. Acute musculoskeletal injuries incorporate the anatomical site of pain, severity of associated pain, mechanism ofinjury, type ofpain and injury patterns at the various player positions. Chronic musculoskeletal injuries include postural analyses and hip flexion angles.
Comparative analyses of the demographic details of the injured v. non-injured players indicated no significant differences, hence these were not predisposing risk factors to injury. Similarly, the comparative analyses of the number of hours trained revealed no statistically significant differences (p>0.05) between the injured and non-injured players, indicating that training did not predispose players to injury.
The lower extremity experienced the most injury (n 119), which confers with previous literature[1,5] indicating the lower back, hip, knee, thigh, tibia/fibula and ankle. Our cohort's most vulnerable acute anatomical site was the knee, which differs from the findings of Naicker et al.[13] and Ellapen et al.,[7]who reported the most vulnerable site to be the ankle. Players who sustained acute knee injuries cited rapid rotational movement and physical trauma to be the predisposing mechanisms of injury, corresponding with the findings of Murtaugh.[4] The author reported that rapid rotational movement increases the risk of medial collateral ligament and anterior cruciate ligaments sprains, which de-stabilise the knee joint.[4] Dick et al.[3] reported that physical trauma from being struck with the ball and/or stick on the tibia and/ or fibula produces varus and valgus forces which contribute to knee instability, propagating severe ligamentous knee injury.
The second most common acute musculoskeletal injury was to the lower back. Players reported that physical trauma from colliding with other players and being struck with the ball and/or stick were the predisposing mechanisms of injury, corresponding with the findings of Dick et al.[3] The ankle was the third most prominent site of acute musculoskeletal injury, which also confers with previous literature.[7,13] The players who sustained ankle injuries reported that the predisposing mechanism was rapid rotational movement. Naicker et al.[13] postulated that rapid rotational movements when playing hockey move the ankle into plantar flexion and inversion, which exceed the plastic properties of the lateral ligaments, thereby producing tearing. Marieb[14] described the arthrology of the talocrucal joint to be hinged in nature, affording limited stability by the medial and lateral ligaments during plantar flexion. However, the medial ligament restraints have proven to be more effectively resistant than the lateral ligaments, yielding fewer reports of eversion ankle sprains than inversion sprains.[4,5]
Midfielders were most vulnerable to acute musculoskeletal injuries, corresponding with Murtaugh's[4] findings. Midfielders often engage in rapid rotational movement in an attempt to manoeuvre around their opponents to gain the advantage, which increases the risk of knee and ankle injuries.[4,7,13] Midfielders have the highest work rate among players, initiating offensive and defensive strategic manoeuvres.[4]
The hip/lower back was categorised as the most susceptible anatomical site of chronic musculoskeletal injury. Murtaugh[4] and Ellapen et al.[7]postulated that the semi-crouched position adopted by hockey players during the game causes excessive spinal loading on the lumbar vertebrae, which negatively affects the hip and lower back; however, the pathomechanics thereof is undetermined.
We postulate that the prolonged hip flexion when playing hockey produces an anterior pelvic tilt (as observed in the sagittal postural analysis). This changes the normal, resting length tension relationship of the agonists (hip flexors) and antagonists (gluteal muscles), thereby producing asymmetrical force couple between the hip flexors and the gluteal muscle. The abnormal length tension relationship between the hip flexors and gluteal muscles has been corroborated by the significant difference between the hip flexion angles of players who sustained hip/ lower-back musculoskeletal injury and non-injured (hip/lower back) players (p<0.05). This abnormal force couple between the hip flexors and the gluteal muscles produced an asymmetrical muscle imbalance. Prentice[15] reports that prolonged hip flexion facilitates anterior pelvic tilt, which produces an asymmetrical force couple between the hip flexors and gluteal muscles leading to painful muscle spasms/strains.
Conclusion
Hockey players in our cohort experienced a high prevalence of acute knee, lower-back and ankle musculoskeletal injuries, consistent with previous findings. [4,7,13] Chronic lower-back injuries have been associated with hip flexor contractures. A primary limitation of our study was the recall bias of the retrospective reporting of musculoskeletal injury and training volumes. Other limitations include the lack of identification of lumbar lordosis and differentiation between structural and functional scoliosis, which should be investigated in future research. However, the novel inclusion of the Thomas test and postural analyses added value to evidence for the intrinsic nature of chronic hip/lower-back injuries. Future studies are needed to validate the findings of our study and to better understand the mechanisms by which intrinsic factors predispose hockey players to musculoskeletal injuries. These findings can best be exploited if hockey coaches, players and parents are made aware of them and are encouraged to seek professional help to lessen the high prevalence of acute and chronic injuries by engaging in rehabilitative and preventive exercises. The hockey fraternity should be educated on the various ways to prevent injury by complying with appropriate training regimes, alterations in technique, periodisation of training programmes and stretching exercises.
References
1. Sherker S, Cassell EA. Review of Field Hockey Injuries and Countermeasures for Prevention. Melbourne, Australia: Monash University Accident Research Centre, 2002. [ Links ]
2. Venter RE, Terblanche E, Fourie L, Ferreira S. Physical and physiological profiles of Boland netball players. South African Journal of Sports Medicine 2005;17(2):3-7. [ Links ]
3. Dick R, Hootman JM, Agel MA, et al. Descriptive epidemiology of collegiate women's field hockey injuries. J Athl Train 2007;42(2):211-220. [ Links ]
4. Murtaugh K. Injury patterns among female hockey players. Med Sci Sports Exerc 2001;33(2):201-207. [ Links ]
5. Rose CP. Injuries in women's field hockey: A four-year survey. Phys Sports Med 1981;9(30):97-100. [ Links ]
6. Lindgren S, Maguire K. Survey of field hockey injuries. Sports Sci Med Quarter 1985;1(30):7-12. [ Links ]
7. Ellapen TJ, Abrahams S, Desai FA, Narsigan S, Van Heerden HJ. Prevalence of musculoskeletal pain among South African female senior national hockey players. Postepy Rehabilitacji 2011;23(2):27-31. [ Links ]
8. Terre-Blanch M, Durrheim K, Painter D. Research in Practice. Cape Town: University of Cape Town Press, 2008:50. [ Links ]
9. Kee D, Seo SR. Musculoskeletal disorders among nursing personnel in Korea. Int J Ind Erg 2007;37:207-212. [ Links ]
10. Van Heerden HJ. Pre-participation Evaluation and Identification of Aetiological Risk Factors in Epidemiology of Sports Injuries Among Youths. Doctor of Philosophy thesis. Pretoria: University of Pretoria, 1996. [ Links ]
11. Hagglund M, Walden M, Bahr R, et al. Methods for epidemiological study of injuries to professional football players: Developing the UEFA model. Br J Sports Med 2005;39:340-346. [http://dx.doi.org/10.1136/bjsm.2005.018267] [ Links ]
12. Kendall FP, Mccreary EK, Provance PG, Rodgers MM, Romani WA. Muscles: Testing and Function with Posture and Pain. 5th ed. Philadelphia, USA: Lippincott Williams & Wilkins, 2001:49-83. [ Links ]
13. Naicker M, Mclean M, Esterhuizen TM, et al. Poor peak dorsiflexor torque associated with incidence of ankle injury in elite field female hockey players. Sci Med Sport 2007;10(6):363-371. [http://dx.doi.org/10.1016/j.jsams.2006.11.007] [ Links ]
14. Marieb E. Human Anatomy and Physiology. 7th ed. San Francisco, USA: Benjamin Cummings Publishing Company, 2004:252-272. [ Links ]
15. Prentice WE. Rehabilitation Techniques for Sports Medicine and Athletic. Champaign, IL, USA: Human Kinetics, 2004:486-500. [ Links ]
 Correspondence:
Correspondence:
T J Ellapen
tellapen1@yahoo.com


{kind=link}
{kind=link}
{kind=link}
{kind=link}