










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Sports Medicine
On-line version ISSN 2078-516X
Print version ISSN 1015-5163
SA J. Sports Med. vol.26 n.3 Bloemfontein 2014
http://dx.doi.org/10.7196/SAJSM.553
REVIEW
Dietary supplements containing prohibited substances: A review (Part 2)
P van der Bijl
BSc Hons (Chem), BSc Hons (Pharmacol), BChD, PhD, DSc; Emeritus Professor and Former Head, Department of Pharmacology, Faculty of Medicine and Health Sciences, Stellenbosch University, Tygerberg, Cape Town, South Africa; and Invited Foreign Professor, Department of Pharmacology, Pirigov's Russian National Research Medical University, Moscow, Russia
ABSTRACT
The role of prohormones, 'classic' and 'designer' steroids, clenbuterol, peptide hormones and newer molecules causing concern in dietary supplements is discussed. Apart from their potential adverse effects on athletes' health, their non-achievement of increased strength and muscle size, trace quantities present in contaminated dietary supplements can lead to failed doping tests. The methodologies used for the identification and determination of prohibited substances in very low concentrations, mainly liquid chromatography and mass spectrometry, are also addressed. Of concern is the anticipation that the number of dietary supplements containing (not yet) prohibited designer steroids and other performance-enhancing newer chemical entities will increase. Athletes, coaches and sports doctors should therefore be provided with information regarding dietary supplements and be advised to minimise risks for non-intentional ingestion of forbidden substances by using safe products listed on databases, such as those obtainable in The Netherlands and Germany.
In Part 1[1] the focus was on the presence of stimulants in dietary supplements, while the current article deals with 'classic' and 'designer' steroids, clenbuterol, peptide hormones and newer molecules that cause concern in sports nutrition due to their accidental intake as contaminants.
Prohormones
It has been shown in a previous study that ~15% of dietary supplements comprising mainly vitamins, minerals, proteins and creatine contained undisclosed anabolic androgenic steroids.[2] These steroids were mainly prohormones, referring to androgenic precursors that are enzymatically activated in vivo to the anabolic steroid testosterone and its derivatives. In the aforementioned study, it was assumed that these prohormones were probably the result of contamination before or during manufacturing processes. Nevertheless, the quantities of prohormone detected in these supplements could have resulted in infringements of doping regulations. Prohormones are viewed by many consumers as natural compounds to promote strength and muscle mass, change body composition and improve general feelings of wellness with fewer adverse effects than testosterone itself or other synthetic androgenic steroids.[3] Furthermore, prohormones are perceived and commercially promoted as legal alternatives to testosterone, with comparable anabolic effects. However, prohormones are listed as prohibited substances on the World AntiDoping Agency (WADA) list and are illegal to sell or import in many countries.
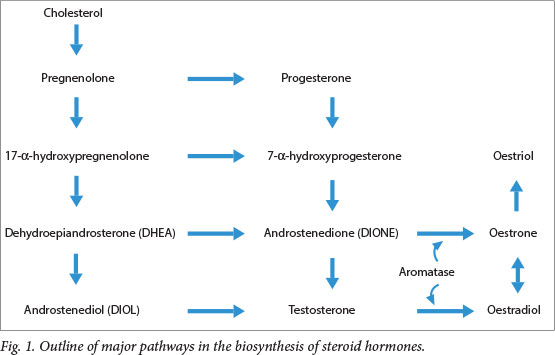
Cholesterol is metabolised by multiple enzyme systems into testosterone via a number of androgenic intermediates (prohormones), including dihydroepiandrosterone (DHEA) (Fig. 1). The biosynthetic pathway via DHEA leads to the production of androstenedione (DIONE) and androstenediol (DIOL). These intermediates can also be converted to the oestrogens, which may cause gynaecomastia and hepatic dysfunction. To counteract these adverse effects, some athletes use prohormones out of the competition season in cycles lasting 4-12 weeks, either alone or in a stacking manner, i.e. taking multiple compounds with different oestrogenic potential simultaneously. Alternatively, users may follow a pyramid mode, taking the highest doses in midcycle. Additionally, selective oestrogen receptor modulators or aromatase inhibitors (Fig. 1) may be taken to attenuate oestrogenic effects, and androgenic herbal products taken to diminish the low period between cycles.[3,4] However, two well-conducted clinical studies have not shown DHEA, DIONE or DIOL to produce any advantageous anabolic or ergogenic effects at all, but have confirmed the risk of adverse effects. In particular, in one of the studies, LDL-cholesterol/HDL-cholesterol ratios were increased by 11%, significantly elevating the risk for cardiovascular disease and reducing luteinising hormone levels, which may decrease testicular and adrenal testosterone production.[3] Other prohormones, e.g. those of the much-used/abused anabolic steroid 19-nortestosterone (nandrolone), have also appeared on the market.[5] One of these prohormones, norandrostendione, administered as a single dose, has been shown to lead to detectable urinary quantities of the main metabolite (19-norandrosterone) of the parent steroid nandrolone for a period >10 days.[5]
Classic anabolic steroids
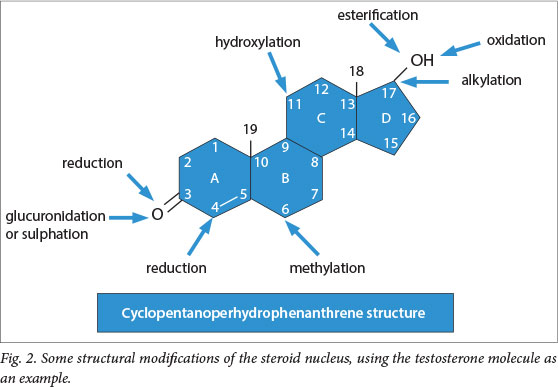
Steroid structures have perhydrocyclopenta-nophenanthrene nuclei comprising four rings (A, B, C and D), as represented by the structure of testosterone (Fig. 2). Loci where modifications occur as well as examples of typical reactions, resulting in structural modifications to the steroid nucleus, are also shown. Furthermore, steroids can be classified into six groups according to the number of carbon atoms, i.e. gonanes (C17), estranes (C18) (e.g. oestradiol and oestrone), androstanes (C19) (e.g. testosterone and androstenedione), pregnanes (C21) (e.g. progesterone and cortisol), cholanes (C24) (e.g. cholic acid and desoxycholic acid) and cholestanes (C27) (e.g. cholesterol). With the exception of the cholanes, steroids are precursors or natural hormones that, depending on their in vivo functions, can be divided into oestrogens, androgens, glucocorticoids and mineralocorticoids. The steroid category of compounds includes the classic anabolic steroids, e.g. metandienone, stanozol, boldenone, oxandrolone, dehydro-chloromethyl-testosterone, etc., which have been found in high amounts (>1 mg/g) in certain dietary supplements and vitamin preparations that are freely available on the market. These steroid ingredients were either listed on package labels under some other chemical/non-approved name or not disclosed at all. Concentrations of these steroids in the supplements were of such orders that even within the limits of recommended supplement intake, supratherapeutic doses of these substances would be ingested. Many athletes and other individuals in the population at large, including women, adolescents and children, regularly consume dietary supplements in quantities beyond the safe daily recommended doses, and therefore adverse effects in these groups of users could be severe. In men, acne, testicular atrophy, prostate enlargement, decreased spermatogenesis, infertility, impotence and changes in libido may occur.[6] Furthermore, gynaecomastia, which may require surgical intervention, can also occur; some male users of steroids concurrently use tamoxifen or other agents to prevent or treat this condition. In women using steroids, acne, potentially irreversible masculinisation, clitoris enlargement, menstrual irregularities and changes in libido may result. In both sexes, psychiatric effects, e.g. aggression ('roid' rage), psychoses, manic episodes, panic disorders, depression, etc. have been documented. Long-term steroid use has also been associated with dependency and a withdrawal syndrome associated with suicidal thoughts, an increased incidence of tumours and premature mortality.[6] Of particular concern are the effects of steroids on cholesterol and lipid metabolism, hypercalcaemia, electrolyte and fluid disturbances, hypertension and thrombotic events, e.g. emboli, myocardial infarction and cerebrovascular accidents, the latter two conditions possibly resulting from an increase in platelet aggregation and erythrogenesis. In adolescents and children, virilisation and premature closure of the epiphyseal plates, which may result in stunted growth, have been described. Most of the classic anabolic steroids are methylated in the 17-position of the D-ring of the perhydro-cyclopentanophenanthrene nucleus (Fig. 2), a molecular feature that is associated with high hepatoxicity and carcinogenicity.[5]
While the commercial sources of these steroids on the world market are not always known, it appears as if many of them are sourced from Chinese bulk manufacturers and are intentionally incorporated into dietary supplements by unscrupulous companies.[5]
Designer steroids
These steroid molecules were synthesised some 5 decades ago and evaluated in preclinical studies for their anabolic and androgenic effects.[7] They are not listed as components of any currently available pharmaceuticals for clinical use, are not on the WADA list of prohibited substances and are manufactured exclusively for the dietary supplement black market. Examples of such agents, to name but a few, are prostanozol, methasterone and andostatrienedione, and to date more than 40 such designer steroid molecules have been detected in laboratories.[7] Little is known regarding their pharmacological actions and safety profiles in humans. They are either listed under some other chemical/non-approved name or are not disclosed at all on dietary supplement labels. Should metabolites of these designer steroids be detected in an athlete's urine, doping infringement charges would probably ensue.
Clenbuterol
Many athletes who claim that they suffer from asthma or exercise-induced asthma use metered-dose inhaled β2-agonists for alleviating their symptoms of bronchoconstriction. While the inhalational β2-agonists such as terbutaline, albuterol and salmeterol are permitted for use by athletes by the WADA, oral and injectable forms of these pharmaceuticals are not. However, some of these β2-agonists, e.g. clenbuterol, are considered anabolic substances by some sports-governing agencies. Hitherto, two cases have been described in which dietary supplements contained therapeutic and supratherapeutic doses of 30 µg/tablet and 2 mg/capsule of clenbuterol, respectively.[8] In the supratherapeutic preparation, which contained 100 times the therapeutic dose of clenbuterol, the presence of this β2-agonist was not disclosed on the package label.
Peptide hormones
Over-the-counter dietary supplements are frequently promoted by manufacturers as being able to increase human growth hormone levels in the body. However, a review has shown that while human growth hormone does increase lean body mass, it has no beneficial effect on strength or exercise capacity in trained athletes.[9] However, use of human growth hormones has been associated with higher rates of soft-tissue oedema, arthralgias and carpal tunnel syndrome. Furthermore, dietary supplements advertised as having anabolic, fat-reducing and anticatabolic properties, and containing the prohibited growth hormone-releasing peptide-2 (GHRP-2), were detected a few years ago. The presence of such substances may lead to inadvertent doping infringements. While GHRP-2 itself is not specifically barred by the WADA for use by athletes, it is a releasing factor that belongs to a prohibited substance group on their list.[7]
Other newer molecules
A selective androgen receptor modulator and agonists of the peroxisome proliferator-activated receptor δ, which produce anabolic effects and enhance endurance, respectively, have been found on the black market.[7]
It has also come to the attention of the WADA that another substance for increasing endurance, GW501516, has been available for some time on the black market, through the internet and elsewhere. Anti-doping authorities have already seen its use by athletes, as there have been a number of positive cases. This developmental drug has not been approved for clinical use anywhere in the world and has been withdrawn from further investigation by pharmaceutical companies due to its serious toxicity profile.[10]
Identification and determination of prohibited substances
While a wide variety ofanalytical techniques have been used in the past to detect prohibited drugs in biological fluids, rapid improvements in mass spectrometry (MS) have allowed accredited laboratories to develop specific and comprehensive screening methods that are able to detect amounts of drugs and/or their metabolites in quantities as low as 1 mg/L in urine.[4] Over many years, gas chromatography (GC) has proven itself in laboratories to be a useful technique for separating and identifying individual components in mixtures of chemical compounds on various chromatographic columns in terms of their retention characteristics (relative to an internal standard compound), as well as for quantifying them. A variety of detectors, e.g. flame ionisation detectors, thermal conductivity detectors and electron capture detectors have been used for this purpose. However, for the successful application of this technique, it is a prerequisite that for compounds to be separated, they are volatile, usually after the necessary derivatisation steps. Samples may also have to be hydrolysed to release steroid metabolites from their glucuronic acid conjugates, usually by means of the enzyme β2-glucuronidase, which may result in the generation of related steroidal compounds or incomplete deconjugation. For the purpose of volatilisation, the mixtures to be analysed are often trimethylsilylated (TMS) prior to injection onto GC columns. The more volatile TMS ethers of the individual components are then distributed between gaseous and solid phases, separated and detected. By feeding gaseous effluents from a GC into an MS, further improvement in identification and quantitation of compounds in mixtures can be expected. However, this technique of GC/MS is not so eminently suitable for routine clinical analysis, but has better applications as a screening tool of prohibited compounds in dietary supplements or urinary metabolites because of the high labour intensiveness, high cost and relatively poor sensitivity. The poor sensitivity is of relevance when samples are analysed for compounds which have low thermal stabilities, e.g. steroids such as trenbolone and gestrinone.[4]
In recent years, another chromatographic tool, i.e. liquid chroma-tography (LC) coupled to ultraviolet or diode-array detectors, has become increasingly important in drug-assaying laboratories. However, similar to GC, this method is not sensitive enough to detect trace levels of compounds and is not well suited for the identification of new substances with unknown chemical and physical properties. Coupled with MS, it provides specificity, precision and high sensitivity, allowing the detection of very low quantities of polar and non-polar compounds, a requirement being that the methodology be extensively validated. LC/MS has high throughput capabilities, requires small sample volumes, minimal sample preparation and thermal stability is usually not a factor. Furthermore, if required, a number of components can be identified and quantified in a single analysis within the dynamic calibration range of the instrumentation, which can span four orders of magnitude. Additionally, because of the absence of hydrolysis or derivatisation steps, LC/MS can be used to measure concentration ratios for steroids between conjugated and free forms, thereby lowering the risk of false positive or misleading outcomes.
The use of ultra-high performance LC has further improved chromatographic resolution, thereby lowering the possibility of missing potentially important co-eluting analytes, and critical pairs of isomers may be separated and detected. Coupled with high acquisition rate mass analysers such as triple quadrupole MS in tandem with LC/MS(/MS), exceptionally powerful techniques have evolved in the detection of steroids with marginal GC properties, for example.[11-13] Methodologies such as these have enabled the identification of characteristic product ions of common steroid structures and nuclei.[11] These powerful analytical tools provide a means of detecting a wide variety of unknown steroids based on common chemical structural properties, new metabolites, as well as new designer steroids (likely to be added to dietary supplements) made to circumvent anti-doping controls.
Conclusion
Dietary supplement use among athletes to enhance performance is proliferating as more individuals strive to obtain a chemical competitive edge. As a result, the concomitant use of dietary supplements containing performance-enhancing substances that fall in the categories outlined in the current review can also be expected to rise. This is despite ever-increasing, sophisticated analytical methodology techniques being used to assay dietary supplement and urine samples in doping laboratories. The reasons for this include: a variety of these chemical entities, many of them on the prohibited drug list of the WADA, are being produced commercially in factories around the world; aggressive marketing strategies are being employed by companies; and these supplements can be easily ordered, for example via the internet. It can also be anticipated that there will be an increase in the number of supplements containing designer steroids and other newer molecules. Chromatographic techniques combined with MS, leading to identification of molecular fragments and product ions, will assist in determining these substances. To prevent accidental doping, information regarding dietary supplements must be provided to athletes, coaches and sports doctors at all levels of competition. In South Africa, this situation is complicated by the fact that the system of Acts and Bills lacks specificity regarding nutritional supplements, including the listing of prohibited substances on package labels.[14,15] The risks of accidental doping via dietary supplement ingestion can be minimised by using safe products listed on databases, e.g. such as those available in The Netherlands and Germany.[5] Finally, athletes must be reminded that if they test positive for a prohibited substance not disclosed on the package label of a supplement, it would constitute a doping violation, with all the consequences thereof.
References
1. Van der Bijl P. Dietary supplements containing prohibited substances: A review (Part 1). South African Journal of Sports Medicine 2014;26(2):59-61. [http://dx.doi.org/10.7196/SAJSM.552] [ Links ]
2. Geyer H, Parr MK, Mareck U, Reinhart U, Schrader Y, Schänzer W Analysis of non-hormonal dietary supplements for anabolic-androgenic steroids: Results of an international study. Int J Sports Med 2004;25(2):124-129. [http://dx.doi.org/10.1055/s-2004-819955] [ Links ]
3. King DS, Baskerville R, Hellsten Y, et al. A - Z of dietary supplements: Dietary supplements, sports nutrition foods and ergogenic aids for health and performance, Part 34. Br J Sports Med 2012;46(9):689-690. [http//dx.doi.org/10.1136/bjsports-2012-091314] [ Links ]
4. Gosetti F, Mazzucco E, Gennaro MC, Marengo E. Ultra high performance liquid chromatography tandem mass spectrometry determination and profiling of prohibited steroids in human biological matrices: A review. J Chromatogr B Analyt Technol Biomed Life Sci 2013;927:22-36. [http://dx.doi.org/10.1016/j.jchromb.2012.12.003] [ Links ]
5. Geyer H, Parr MK, Koehler K, Mareck U, Schänzer W, Thevis M. Dietary supplements cross-contaminated and faked with doping substances. J Mass Spectrom 2008;43(7):892-902. [http:dx.doi.org/10.1002/jms.1452] [ Links ]
6. Ambrose P. Drug use in sports: A veritable arena for pharmacists. J Am Pharm Assoc 2004:44(4):501-514. [ Links ]
7. Geyer H, Braun H, Burke LM, Stear SJ, Castell LM. A-Z of dietary supplements: Dietary supplements, sports nutrition foods and ergogenic aids for health and performance, Part 22. Br J Sports Med 2011;45(9):752-754. [http://dx.doi.org/10.1136/bjsports-2011-090180] [ Links ]
8. Parr MK, Koehler K, Geyer H, Guddat S, Schänzer W. Clenbuterol marketed as dietary supplement. Biomed Chromatogr 2008;22(3):298-300. [http://dx.doi.org/10.1002/bmc.928] [ Links ]
9. Liu H, Bravata DM, Olkin I, et al. Systematic review: The effects of growth hormone on athletic performance. Ann Intern Med 2008;148(10):747-758. [ Links ]
10. WADA issues alert on GW501516. http://playtrue.wada-ama.org/news/wada-issues-alert-on-gw501516/ (accessed 15 May 2014). [ Links ]
11. Catlin DH, Sekera MH, Ahrens BD, Starcevic B, Chang YC, Hatton CK. Tetrahydrogestrinone: Discovery, synthesis, and detection in urine. Rapid Commun Mass Spectrom 2004;18(12):1245-1249. [http://dx.doi.org/10.1002/rcm.1495] [ Links ]
12. Thevis M, Geyer H, Mareck U, Schänzer W. Screening for unknown synthetic steroids in human urine by liquid chromatography-tandem mass spectrometry. J Mass Spectrom 2005;40(7):955-962. [http://dx.doi.org/10.1002/jms.873] [ Links ]
13. Pozo OJ, Van Eenoo P, Deventer K, Delbeke FT. Development and validation of a qualitative screening method for the detection of exogenous anabolic steroids in urine by liquid chromatography-tandem mass spectrometry. Anal Bioanal Chem 2007;389(4):1209-1224. [http://dx.doi.org/10.1007/s00216-007-1530-6] [ Links ]
14. Gabriels G, Lambert M, Smith P. Information on nutritional supplement labels: Time for legislation? S Afr J Clin Nutr 2012;25(1):22-26. [ Links ]
15. Gabriels G, Lambert M, Smith P, Hiss D. Will the new Consumer Protection Act prevent harm to nutritional supplement users? S Afr Med J 2011;101(8):543-545. [ Links ]
Corresponding author: P van der Bijl (pietervanderbijlcpt@gmail.com)

