










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSAMJ: South African Medical Journal
versão On-line ISSN 2078-5135
versão impressa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.114 no.4 Pretoria Abr. 2024
http://dx.doi.org/10.7196/SAMJ.2024.v114i4.1646
RESEARCH
Diagnosis and presenting features of autoimmune hepatitis at a central referral hospital in South Africa
Y MaharajI; V G NaidooII, III
IMB ChB; Division of Internal Medicine, College of Health Sciences, Nelson R Mandela School of Medicine, University of KwaZulu-Natal, Durban, South Africa
IIFCP (SA), Cert Gastroenterology (Phys); Department of Gastroenterology, Nelson R Mandela School of Medicine, University of KwaZulu-Natal, Durban, South Africa
IIIFCP (SA), Cert Gastroenterology (Phys); Gastrointestinal Cancer Research Group, Nelson R Mandela School of Medicine, University of KwaZulu-Natal, Durban, South Africa
ABSTRACT
BACKGROUND: Autoimmune hepatitis (AIH) has scarcely been reported on in patients of black African descent. Similarly, few studies have focused on the relationship between AIH and HIV infection
OBJECTIVE: To describe the presenting features of AIH from a single referral centre in a sub-Saharan African setting. We also compare the clinical and biochemical features of people with HIV to people without HIV
METHODS: This study was a retrospective chart review. Patients were included if they fulfilled criteria for the International AIH Group simplified score for probable or definite AIH, were >18 years old at inclusion, and attended the adult gastroenterology clinic at a central referral hospital in South Africa for the period 1 January 2015 to 31 December 2020 on at least two occasions
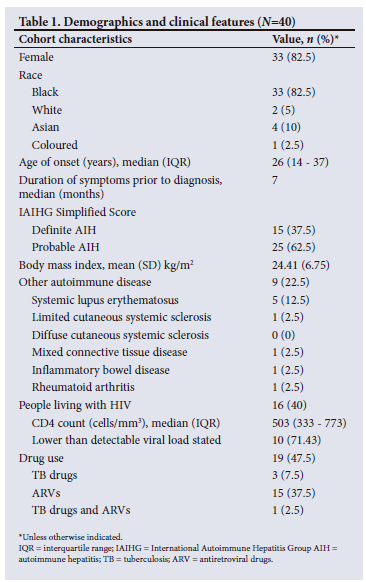
RESULTS: Forty cases were included, of which 33 (82.5%) were female and 33 (82.5%) were black African. Median age at diagnosis was 26 years. A diagnosis of a coexistent autoimmune disease was made in 22.5% of patients, with systemic lupus erythematosus being the most common (12.5%). There were 16 people living with HIV, all of whom were female (p=0.03), with a significantly older age of disease onset compared with people without HIV (median age 38 v. 17.5 years, p<0.001
CONCLUSION: AIH is a disease most commonly affecting young females. Female sex and older age of onset is associated with AIH in people living with HIV
Autoimmune hepatitis (AIH) is a chronic inflammatory condition of the liver, with a reported annual incidence rate of 0.5 - 2.2 per 100 000 population.[1] The female-to-male ratio is approximately 4:1 in type 1 AIH and 10:1 for type 2 AIH.[2] It can affect people of any age group and of all ethnic backgrounds.[3,4] Clinical presentation may range from asymptomatic to fulminant hepatic failure. Diagnosis was aided with the development of the 1999 International Autoimmune Hepatitis Group (IAIHG) scoring system, and the subsequent 2008 simplified score intended for routine clinical practice.[5]
Studies reporting on the presenting features of AIH in patients of black African descent are exceedingly rare.[6] In addition, the coexistence of AIH and HIV infection has been rarely reported in the literature. People living with HIV often have other more common reasons for developing liver injury, such as medication, opportunistic infections, steatosis/steatohepatitis, alcoholic or viral hepatitis and AIDS cholangiopathy.[7] Therefore, an autoimmune process may not be considered early in the differential for such patients, or the patient expires prior to the completion of diagnostic testing.[8] To our knowledge, direct comparisons between people living with HIV and those living without HIV within the same population have not previously been reported on.
This study aims to describe the presenting features of AIH from a single referral centre in a sub-Saharan African setting. We also compare the clinical and biochemical features of people with HIV to people without HIV in this cohort.
Methods
The study was conducted at a central referral hospital in South Africa (SA).
Patients were included if they met the following criteria:
(i) Diagnosis of AIH based on the IAIHG simplified scoring criteria with a score >7 for definite, and >6 for probable.
(ii) Attended the adult gastroenterology clinic for the period 1 January 2015 to 31 December 2020 on at least two occasions.
(iii) >18 years old at inclusion.
Case capture
Electronic outpatient hospital records were searched using ICD 10 codes for AIH (K75.4) and cirrhosis (K74). In addition, the terms primary biliary cholangitis (K74.3) and primary sclerosing cholangitis (K83.0) were searched to identify any possible cases with overlap syndromes, as well as drug-induced liver injury (K71) to identify any cases fulfilling criteria for AIH, but for which a drug(s) obscured the diagnosis. Diagnostic evaluation for AIH was conducted by retrospectively employing the IAIHG simplified score to each case based on available electronic biochemical, immunological and histological data.
Incident cases (AIH diagnosis after 1 January 2015) and prevalent cases (AIH diagnosis before 1 January 2015 plus a minimum of two outpatient visits after 1 January 2015) were included. Information was collected using a bespoke data collection tool - a Word (Microsoft, USA) document designed to facilitate capture of patient demographic and clinical data. Each case was cross-checked to minimise inconsistencies and errors in data capturing.
Statistics
Data were analysed using Excel (Microsoft, USA) and SPSS (IBM, USA). Continuous variables were expressed as means and standard deviations, or medians and interquartile ranges (IQR). Chi-square and Fisher's exact tests were used for categorical data comparisons. The t-test or Mann-Whitney U test was used to compare groups. P was significant at <0.05.
Ethical approval
Ethics approval was obtained from the relevant Biomedical Research Ethics committee (ref. no. BREC/00003867/2022) and conforms to the provisions of the Declaration of Helsinki.
Results
Overall cohort
A total of 660 records were retrieved, and 58 patients were identified as having a possible diagnosis of AIH. Of these, 18 cases were subsequently excluded as they did not meet the IAIHG simplified score due to incomplete/missing data. A final cohort of 40 patients was established. Demographic and clinical information of patients are represented in Table 1.
Clinical features
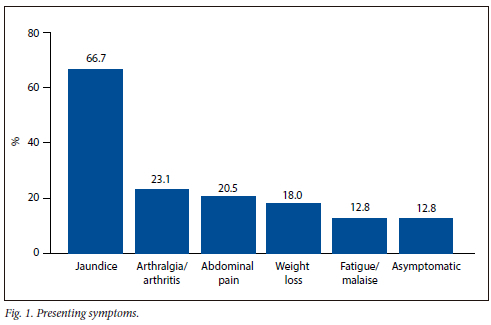
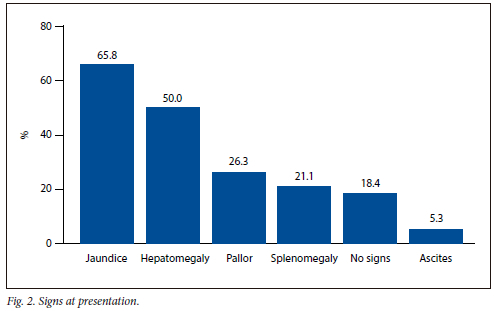
There were 33 (82.5%) female and 33 (82.5%) black African patients. The median age at diagnosis was 26 years. Symptoms (Fig. 1) were present in 34 (87.18%) patients, with a median duration of symptoms prior to diagnosis being 7 months. The correct diagnosis was identified in approximately half (48.28%) of patients at 6 months following the onset of symptoms. Jaundice (65.79%) and hepatomegaly (50%) were the most common clinical features on presentation (Fig. 2). Cirrhosis was present in half (50%) of patients as detected on imaging studies or on histology. Portal hypertension was diagnosed either clinically or based on imaging features and was present in 13 (32.5%) of patients. A diagnosis of a coexistent autoimmune disease was made in 22.5% of patients, with systemic lupus erythematosus (SLE) being the most common (12.5%). Almost half (47.5%) of all patients were on potentially hepatotoxic drugs at the time of presentation.
Laboratory features
All patients included in the study had an abnormal liver function test on presentation (Table 2). Transaminase enzymes were markedly elevated in most patients, with a median alanine transaminase (ALT) of 225.5 U/L (IQR 100 - 456.5 U/L) and aspartate transaminase (AST) of 277.5 U/L (IQR 140 - 753.5 U/L). Similarly, cholestatic enzymes were elevated to varying levels with a median alkaline phosphatase (ALP) of 264 U/L (IQR 190 - 486.5 U/L) and gamma-glutamyl transferase (GGT) of 234 U/L (IQR 112 - 594.5 U/L). The median total bilirubin was 36.5 umol/L (IQR 18.25 - 82.5 umol/L). Albumin was marginally reduced in most patients with a mean value of 34.02 g/L. The international normalised ratio (INR) was elevated to a level >1.5 in 11 (27.5%) patients at the time of presentation. All patients tested for IgG levels had values >1.1, above the upper limit of normal with a mean (standard deviation) of 36.66 (11.46) g/L. Thirty-nine (97.5%) patients had all three antibody tests, standard for suspected AIH, done. One patient had an anti-liver-kidney microsomal (anti-LKM) antibody test omitted but was classified as type 1 AIH due to a positive ANF with a titre >1:80 and a positive smooth muscle antibody. From these results it was determined that 36 (90%) patients could be classified as type 1 AIH, 2 (5%) patients as type 2 AIH and 2 (5%) as seronegative AIH.
Tests for hepatitis B surface antigen (HBsAg) and hepatitis C antibody (HCV Ab) were negative in all patients.
Histology
Thirty-eight (95%) patients had a liver biopsy. Two patients did not have a liver biopsy, one due to an initial prolonged INR who was treated for presumed AIH and demonstrated a good response to corticosteroid therapy, and the other due to patient refusal. Histology results were classified as typical of AIH if stated as such by the pathologist or if the description of the pattern met criteria stipulated by the IAIHG in the simplified criteria for the diagnosis of autoimmune hepatitis. Of these, 14 (36.84%) patients had typical features and 22 (57.89%) patients had features compatible with AIH, with only 2 (5.26%) patients having a suboptimal biopsy owing to there being inadequate representative tissue on either sample for any meaningful conclusions to be drawn. Interface hepatitis (80.56%) and a lymphoplasmacytic infiltrate (80%) were the most common histological findings. Hallmark features such as emperipolesis and rosette formation were exceedingly rare. Both patients with seronegative AIH had typical features on liver biopsy. All patients living with HIV had a liver biopsy, with 9 having typical findings for AIH, 6 having compatible features, and 1 with a suboptimal biopsy.
Diagnosis
The IAIHG simplified scoring system was applied retrospectively to all patients. Fifteen (37.5%) patients were classified as definite AIH, and 25 (62.5%) patients as probable AIH.
Subgroup comparison
People with HIV and people without HIV
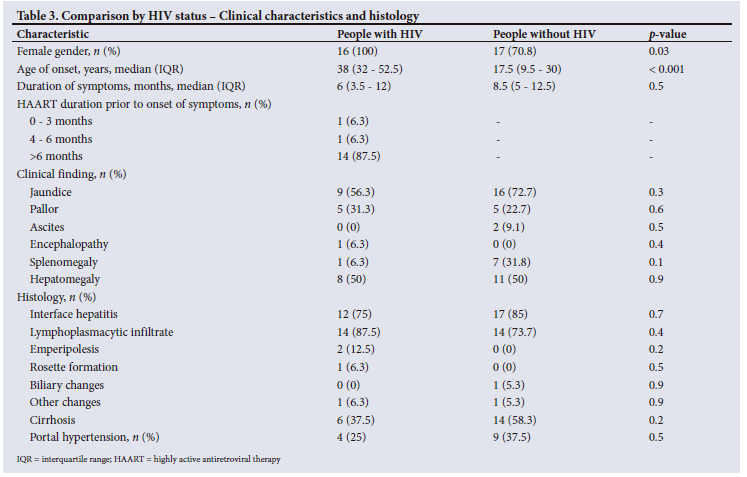
Sixteen (40%) patients were living with HIV at the time of their AIH diagnosis (Tables 3 and 4). All patients living with HIV were female, with a significantly older age of disease onset as compared with patients without HIV (median age 38 v. 17.5 years, p<0.001). In addition, all patients living with HIV were already on antiretroviral drugs at the time of AIH diagnosis. The median duration of antiretroviral (ARV) therapy prior to onset of symptoms of AIH was 4 years (IQR 2 - 5 years), with only two patients (12.5%) presenting within 6 months. The median CD4 count was 503 cells/mm3 (IQR 333 - 773 cells/mm3). Among the 14 patients who had a viral load result, only 4 had a detectable viral load.
Jaundice was a less common presenting feature in patients living with HIV (56.3% v. 72.7%), but this was not statistically significant (p=0.3). Cirrhosis and portal hypertension were noted in 58.3% and 37.5%, respectively, of patients without HIV, as compared with 37.5% and 25% in patients with HIV. There were no significant differences identified in the clinical and histological findings between the two groups.
Transaminase and IgG levels were consistently lower in patients living with HIV. Gamma-glutamyl transferase levels were elevated to a greater degree in patients living with HIV, with the difference between the two groups reaching statistical significance. Antinuclear factor (ANF) and anti-smooth muscle antibody (ASMA) were positive in 11 (68.75%) and 10 (62.5%) patients living with HIV, respectively.
Discussion
Autoimmune hepatitis is a disease that affects people of all ages, genders and ethnic groups.[3,4] However, like with many autoimmune conditions, a female preponderance is well established.[2] In this study, a female predominance was noted, with similar ratios demonstrated in population studies in various nations across the globe.[9] The median age at diagnosis was 26 years (IQR 14 - 37 years). This is in stark contrast to population studies from Europe, Asia and the Americas, where age of onset is often reported to be in middle-aged or post-menopausal women.[9] However, a London-based study comparing the median age of onset between black and white patients with AIH demonstrated a statistically significant difference between the two groups, with black patients presenting at a younger age (median 38 years v. 45 years).[10] Nonspecific symptoms were uncommon, ranging from 12.82% to 23.08%. An epidemiological study of AIH in the USA revealed marginally higher rates of similar nonspecific symptoms of 23 - 44%.[11]
Cirrhosis was detectable at or shortly after diagnosis in 50% of patients in the current study, reflecting the chronicity of the disease. This is similar to a SA study examining the characteristics of AIH in a paediatric population in which cirrhosis was detected in 56% of cases.[12] Lower rates of cirrhosis have been reported in other studies with 6.4 - 35.4% of patients having cirrhosis observed at diagnosis in East Asian countries and in many European countries such as the Netherlands, Denmark and Sweden (12, 28.3 and 30%, respectively).[13-18] Marginally lower rates have been reported in other developed nations such as Italy (23%), the UK (25%), Canada (33.9%) and the USA (43.6%).[11,19-21] In contrast, cirrhosis was a frequent finding in Southeast Asia, with cohorts from Pakistan and India reporting frequencies of 84.1% and 71.2%, respectively.[22,23] Approximately half (48.48%) of black patients in the present study had evidence of cirrhosis. A study published in 2001 reported cirrhosis as being a far more common finding on initial liver biopsy among African American patients with AIH compared with white Americans (85 v. 38%).[24] With very few patients from other race groups in this cohort, no meaningful comparison could be made.
In keeping with other reports, this study demonstrated type 1 AIH as being the most common (90%), with type 2 AIH being rare (5%).[25,26] In contrast to the local paediatric study that demonstrated a high proportion (40%) of seronegative AIH patients, we found this group to be relatively rare (5%).[12]
The presence of concomitant autoimmune conditions was a common occurrence in this cohort (22.5%). However, most of these patients were diagnosed with systemic autoimmune conditions such as SLE, as compared with a predominance of organ-specific autoimmune conditions such as autoimmune thyroid disease reported elsewhere.[27-31]
Given the number of people living with HIV identified in the study, a comparison was made between this group of patients and people without HIV. To our knowledge, this is the first head-to-head comparison of this nature reported in the literature. In keeping with published literature, a female predominance was noted. The median CD4 count of 503 cells/mm3 was very similar to the median of 557 cells x 106/L published in a 2019 case series, which reported 13 people with HIV diagnosed with AIH.[32] Only 4 patients had a detectable viral load, and 2 cases had unreported viral loads. This is consistent with a 2019 systematic review of the published literature on AIH in patients with HIV infection that demonstrated most patients as having suppressed viral loads (7 out of 35 had detectable viral loads, and 2 cases had unreported viral loads). Similarly, all patients were already on highly active antiretroviral therapy (HAART) at the time of their AIH diagnosis. Other autoimmune conditions coexisted in 17.1% of patients in the systematic review, with this cohort demonstrating a comparable percentage (18.75%), all of whom had SLE.[33] Cirrhosis and portal hypertension were more frequently encountered in patients without HIV, but the differences were not statistically significant given the small number of patients for comparison in each group. There was a trend toward lower transaminase levels observed in patients with HIV, and although not statistically significant, a proposed explanation for this finding is a less robust immune response in this patient group. The degree of elevation of transaminases was comparable between this study and the 2019 case series (median ALT 138.5 U/L v. 177 U/L, AST 211 U/L v. 178 U/L). Regarding the consistently higher GGT levels among patients with HIV, it is unclear whether this represents a unique feature of AIH in this subgroup or whether this was a result of some external influence such as being drug related. All patients had elevated IgG levels in comparison with the 85% reported in the 2019 case series.[32] Interestingly, there were no other significant differences between people with HIV and people without HIV, which may be explained by the lack of severe immunodeficiency noted in the former group.
People living with HIV often have other more common reasons for developing liver injury, such as medication, opportunistic infections, steatohepatitis, alcoholic or viral hepatitis and AIDS cholangiopathy, hence a liver biopsy remains a useful diagnostic procedure in this setting.[7] The occurrence of AIH following the initiation of HAART, with recovery of CD4 cell count, may suggest a manifestation of immune reconstitution, or may be recognition of a previously subclinical disease process. However, the argument for this association is not supported by this study, as most patients had been on HAART for >6 months prior to the onset of AIH symptoms. This finding is similar to that of the 2019 case series, in which 11 of the 13 people living with HIV had been initiated on ARVs at the time of diagnosis of HIV infection, with a median duration of ARV therapy to AIH diagnosis of 6 years.[32] Additionally, despite the differing pathogenetic mechanisms between the two disease processes, with HIV infection resulting in progressive depletion and AIH the hyper-reactivity of T-lymphocytes, it has been shown that HIV has the potential to initiate an autoimmune process through polyclonal stimulation of B cells.[34] The mechanisms by which AIH emerges in HIV infection remain poorly understood. Nonetheless, further research is needed to unravel the relationship between these two conditions, and thus improve the approach to managing both conditions simultaneously.
The limitations of this study include its small sample size, missing data and it being limited to a single facility, as well as to patients who had sought medical treatment only within the public sector.
Conclusion
The results of this study indicate that, in a predominantly black African population, AIH mainly affects younger adult females. The presence of other autoimmune diseases, particularly SLE, was not uncommon. A comparison between people with HIV and people without HIV with concomitant AIH demonstrated a significantly older age of onset and a female predominance for AIH occurrence in the former group. GGT levels were higher among people living with HIV, although the reason for this remains unclear. Further research into AIH and HIV is required to elucidate the clinical, immunological and pathological features in this group of patients.
Declaration. This study was undertaken to fulfil the requirement of the research project component of a MMed degree by YM.
Acknowledgements. None.
Author contributions. The study concept and design were carried out by YM and VGN. Acquisition, analysis and interpretation of the data, as well as drafting of the work was carried out by YM. Critical revision of the manuscript for important intellectual content was performed by VGN. Final approval of the manuscript was carried out by YM and VGN. Statistical analysis was performed by Ms Cathy Connolly.
Funding. None.
Conflicts of interest. None.
References
1. Wang Q, Yang F, Miao Q, Krawitt EL, Gershwin ME, Ma X. The clinical phenotypes of autoimmune hepatitis: A comprehensive review. J Autoimmun 2016;66:98-107. https://doi.org/10.1016/j.jaut.2015.10.006 [ Links ]
2. Czaja AJ, Donaldson PT. Gender effects and synergisms with histocompatibility leukocyte antigens in type 1 autoimmune hepatitis. Am J Gastroenterol 2002;97(8):2051-2057. https://doi.org/10.1111/j.1572-0241.2002.05921.x [ Links ]
3. Krawitt EL. Autoimmune hepatitis. N Engl J Med 2006;354(1):54-66. https://doi.org/10.1056/nejmra050408 [ Links ]
4. Van Gerven NM, de Boer YS, Mulder CJ, van Nieuwkerk CM, Bouma G. Autoimmune hepatitis. World J Gastroenterol 2016;22(19):4651-4661. https://doi.org/10.3748/wjg.v22.i19.4651 [ Links ]
5. Hennes EM, Zeniya M, Czaja AJ, et al. Simplified criteria for the diagnosis of autoimmune hepatitis. Hepatology 2008;48(1):169-176. https://doi.org/10.1002/hep.22322 [ Links ]
6. Jemilohun A, Ola T. Autoimmune liver diseases in native Black Africans: Extremely rare or inadequately investigated diseases? J Adv Med Medic Res 2017;24(7):1-14. https://doi.org/10.9734/jammr/2017/36681 [ Links ]
7. Sonderup MW, Wainwright H, Hall P, Hairwadzi H, Spearman CW. A clinicopathological cohort study of liver pathology in 301 patients with human immunodeficiency virus/acquired immune deficiency syndrome. Hepatology 2015;61(5):1721-1729. https://doi.org/10.1002/hep.27710 [ Links ]
8. Parekh S, Spiritos Z, Reynolds P, Parekh S, Perricone A, Quigley B. HIV and autoimmune hepatitis: A case series and literature review. J Biomedical Sci 2017;6(2):1-4. https://doi.org/10.4172/2254-609x.100057 [ Links ]
9. Enomoto H, Nishiguchi S. Similarities and differences in autoimmune hepatitis epidemiology between east and west: Autoimmune hepatitis in East Asia, Southeast Asia, and South Asia. Inflamm Intest Dis 2017;1(4):150-158. https://doi.org/10.1159/000454879 [ Links ]
10. De Boer YS, Gerussi A, van den Brand FF, et al Association between black race and presentation and liver-related outcomes of patients with autoimmune hepatitis. Clin Gastroenterol Hepatol 2019;17(8):1616-1624. https://doi.org/10.1016/j.cgh.2018.11.028 [ Links ]
11. Tunio NA, Mansoor E, Sheriff MZ, Cooper GS, Sclair SN, Cohen SM. Epidemiology of autoimmune hepatitis (AIH) in the United States between 2014 and 2019: A population-based national study. J Clin Gastroenterol 2021;55(10):903-910. https://doi.org/10.1097/mcg.0000000000001449 [ Links ]
12. Yassin S, De Lacy R, Pillay K, Goddard E. Characteristics and outcomes of autoimmune hepatitis from a tertiary paediatric centre, Cape Town, South Africa. J Trop Pediatr 2020;66(4):448-457. https://doi.org/10.1093/tropej/fmz088 [ Links ]
13. Abe M, Mashiba T, Zeniya M, Yamamoto K, Onji M, Tsubouchi H. Present status of autoimmune hepatitis in Japan: A nationwide survey. J Gastroenterol 2011;46(9):1136-1141. https://doi.org/10.1007/s00535-011-0421-y [ Links ]
14. Kim BH, Kim YJ, Jeong SH, et al. Clinical features of autoimmune hepatitis and comparison of two diagnostic criteria in Korea: A nationwide, multicenter study. J Gastroenterol Hepatol 2013;28(1):128-134. https://doi.org/10.1111/j.1440-1746.2012.07292.x [ Links ]
15. Koay LB, Lin CY, Tsai SL, et al Type 1 autoimmune hepatitis in Taiwan: Diagnosis using the revised criteria of the International Autoimmune Hepatitis Group. Dig Dis Sci 2006;51(11):1978-1984. https://doi.org/10.1007/s10620-005-9068-y [ Links ]
16. Van Gerven NM, Verwer BJ, Witte BI, et al Epidemiology and clinical characteristics of autoimmune hepatitis in the Netherlands. Scand J Gastroenterol 2014;49(10):1245-1254. https://doi.org/10.3109/00365521.2014.946083 [ Links ]
17. Gr0nbœk L, Vilstrup H, Jepsen P. Autoimmune hepatitis in Denmark: Incidence, prevalence, prognosis, and causes of death. A nationwide registry-based cohort study. J Hepatol 2014;60(3):612-617. https://doi.org/10.1016/j.jhep.2013.10.020 [ Links ]
18. Werner M, Prytz H, Ohlsson B, et al. Epidemiology and the initial presentation of autoimmune hepatitis in Sweden: A nationwide study. Scand J Gastroenterol 2008;43(10):1232-1240. https://doi.org/10.1080/00365520802130183 [ Links ]
19. Muratori P, Granito A, Quarneti C, et al Autoimmune hepatitis in Italy: The Bologna experience. J Hepatol 2009;50(6):1210-1218. https://doi.org/10.1016/j.jhep.2009.01.020 [ Links ]
20. Gordon V, Adhikary R, Appleby V, et al. Diagnosis, presentation and initial severity of autoimmune hepatitis (AIH) in patients attending 28 hospitals in the UK. Liver Int 2018;38(9):1686-1695. https://doi.org/10.1111/liv.13724 [ Links ]
21. Feld JJ, Dinh H, Arenovich T, Marcus VA, Wanless IR, Heathcote EJ. Autoimmune hepatitis: Effect of symptoms and cirrhosis on natural history and outcome. Hepatology 2005;42(1):53-62. https://doi.org/10.1002/hep.20732 [ Links ]
22. Hassan N, Siddiqui AR, Abbas Z, et al Clinical profile and HLA typing of autoimmune hepatitis From Pakistan. Hepat Mon 2013;13(12):e13598. https://doi.org/10.5812/hepatmon.13598 [ Links ]
23. Amarapurkar D, Dharod M, Amarapurkar A. Autoimmune hepatitis in India: Single tertiary referral centre experience. Trop Gastroenterol 2015;36(1):36-45. https://doi.org/10.7869/tg.243 [ Links ]
24. Lim KN, Casanova RL, Boyer TD, Bruno CJ. Autoimmune hepatitis in African Americans: Presenting features and response to therapy. Am J Gastroenterol 2001;96(12):3390-3394. https://doi.org/10.1111/j.1572-0241.2001.05272.x [ Links ]
25. Johnson PJ, McFarlane IG. Meeting report: International Autoimmune Hepatitis Group. Hepatology 1993;18(4):998-1005. https://doi.org/10.1002/hep.1840180435 [ Links ]
26. Feld JJ, Heathcote EJ. Epidemiology of autoimmune liver disease. J Gastroenterol Hepatol 2003;18(10):1118-1128. https://doi.org/10.1046/j.1440-1746.2003.03165.x [ Links ]
27. Guo L, Zhou L, Zhang N, Deng B, Wang B. Extrahepatic autoimmune diseases in patients with autoimmune liver diseases: A phenomenon neglected by gastroenterologists. Gastroenterol Res Pract 2017;2017:1-7. https://doi.org/10.1155/2017/2376231 [ Links ]
28. Teufel A, Weinmann A, Kahaly GJ, et al. Concurrent autoimmune diseases in patients with autoimmune hepatitis. J Clin Gastroenterol 2010;44(3):208-213. https://doi.org/10.1097/mcg.0b013e3181c74e0d [ Links ]
29. Fogel R, Comerford M, Chilukuri P, Orman E, Chalasani N, Lammert C. Extrahepatic autoimmune diseases are prevalent in autoimmune hepatitis patients and their first-degree relatives: Survey study. Interact J Med Res 2018;7(2):e18. https://doi.org/10.2196/ijmr.9625 [ Links ]
30. Wong GW, Yeong T, Lawrence D, Yeoman AD, Verma S, Heneghan MA. Concurrent extrahepatic autoimmunity in autoimmune hepatitis: Implications for diagnosis, clinical course and long-term outcomes. Liver Int 2017;37(3):449-457. https://doi.org/10.1111/liv.13236 [ Links ]
31. Muratori P, Fabbri A, Lalanne C, Lenzi M, Muratori L. Autoimmune liver disease and concomitant extrahepatic autoimmune disease. Eur J Gastroenterol Hepatol 2015;27(10):1175-1179. https://doi.org/10.1097/meg.0000000000000424 [ Links ]
32. Chaiteerakij R, Sanpawat A, Avihingsanon A, Treeprasertsuk S. Autoimmune hepatitis in human immunodeficiency virus-infected patients: A case series and review of the literature. World J Gastroenterol 2019;25(35):5388-5402. https://doi.org/10.3748/wjg.v25.i35.5388 [ Links ]
33. Mubder M, Azab M, Jayaraj M, et al. Autoimmune hepatitis in patients with human immunodeficiency virus infection: A systematic review of the published literature. Medicine 2019;98(37):e17094. https://doi.org/10.1097/md.0000000000017094 [ Links ]
34. Root-Bernstein R. Antigenic complementarity between HIV and other AIDS-associated infections results in idiotype-antiidiotype antibody complexes that cross react with lymphocyte proteins. Vaccine 2005;23(17-18):2160-2163. https://doi.org/10.1016/j.vaccine.2005.01.049 [ Links ]
 Correspondence:
Correspondence:
Y Maharaj
yasheenm@webmail.co.za
Accepted 4 March 2024


{kind=link}
{kind=link}
{kind=link}