










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSAMJ: South African Medical Journal
versão On-line ISSN 2078-5135
versão impressa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.114 no.4 Pretoria Abr. 2024
http://dx.doi.org/10.7196/SAMJ.2024.v114i4.1531
RESEARCH
Towards developing new private sector obstetric care and contracting models in South Africa: Insights from public hospitals using private general practitioners to provide caesarean deliveries
G C SolankiI, II, III; T DohertyIV, V; V BrijlalVI; E DaviaudVII; S FawcusVIII
IBChD, DrPH; Health Systems Research Unit, South African Medical Research Council, Cape Town, South Africa
IIBChD, DrPH; Health Economics Unit, School of Public Health and Family Medicine, Faculty of Health Sciences, University of Cape Town, South Africa
IIIBChD, DrPH; NMG Consultants and Actuaries, Cape Town, South Africa
IVMPH, PhD; Health Systems Research Unit, South African Medical Research Council, Cape Town, South Africa
VMPH, PhD; Department of Paediatrics and Child Health, Faculty of Health Sciences, University of Cape Town, South Africa
VIBCom (Law, Economics), MSc (Economics); Clinton Health Access Initiative, Pretoria, South Africa
VIIMSc (Economics, Health Economics); Health Systems Research Unit, South African Medical Research Council, Cape Town, South Africa
VIIIMB BCh, FRCOG; Department of Obstetrics and Gynaecology, Faculty of Health Sciences, University of Cape Town, South Africa
ABSTRACT
Maternal healthcare in South Africa faces huge private and public health systems challenges. A key challenge for policy makers is how to address the inappropriate patterns of obstetric care in the private sector and how to mobilise private sector resources to serve the broader population dependent on the public sector, without replicating those patterns of inappropriate care. Developing and implementing new obstetric care models that address these challenges and lend themselves to public private engagements could play a vital role in efforts to improve obstetric care in the country. Drawing on insights from research we carried out on the care and contracting models used by five rural district hospitals in the Western Cape Province to contract private general practitioners to provide caesarean delivery services, this article outlines a potential alternative private sector obstetric care model with the aim of stimulating discussion by all relevant stakeholders on the development of new obstetric models for improving obstetric care in the country.
While South Africa (SA)'s total health spend of 8% - 9% of gross domestic product is comparable to other upper middle-income countries, expenditure is highly inequitably spread across the public and private sectorsand heavily skewed towards the private sector. In 2017, the per capita expenditure per year was estimated to be ZAR5 500 for those dependent on the public health system and ZAR20 000 for those who were able to afford private health insurance cover or pay out of pocket for private sector care.[1] This has resulted in huge disparities between the two sectors. The public sector is characterised by a relatively low per-capita spend, weak infrastructure and governance and an inability to deliver accessible quality care to all who depend upon it. The private sector is characterised by a high per-capita spend and has a strong infrastructure, but is inefficient, fragmented and poorly regulated.[2] There is a highly skewed distribution of providers towards the private sector, and the models of care for the two sectors are widely divergent with the public sector relying largely on 'team-based' models of care while the private sector is dominated by 'individual provider' models of care.[3] This is particularly evident in the area of maternal and child care and caesarean deliveries - a major public health concern in South Africa (SA).[4,5] In the public sector, caesarean delivery rates (28.1%) are in line with patterns seen in other low-and-middle-income countries,[6] but the case fatality rate (CFR) for caesarean deliveries is three times higher than for vaginal delivery, and 27% of the caesarean delivery-related CFR is associated with haemorrhage.[4] A review of avoidable factors suggests that in regional hospitals this could be due to delays in performing caesarean deliveries for obstetric emergencies due to overburdened services, whereas in district hospitals it could be due to lack of appropriate skills to perform caesarean deliveries safely and deal with surgical complications.[4]
In the private sector, caesarean delivery rates of between 74%[7] and 76.9%[8] are among the highest in the world, reflecting high levels of inappropriate caesarean deliveries. While requiring further research to confirm definitively, the practice/care models (individual specialist driven), remuneration models (fee for service), medicolegal framework (individual) and lack of monitoring regulation have been offered as possible drivers of the high rates.[9] A research brief of the Council for Medical Schemes, the regulatory body for private health insurances in SA, concluded that 'urgent steps must be taken to reduce what is likely to be high levels of medically unnecessary caesarean delivery rates in the medical schemes population'.[8]
Key challenges for policy makers in SA are how to address the inappropriate patterns of obstetric care in the private sector and how to mobilise private sector resources to serve the broader population dependent on the public sector without replicating those patterns of inappropriate care. The high levels of inappropriate care and the highly fragmented nature of the SA private sector make it difficult to develop and implement such partnerships in the current environment. Successfully developing and implementing new integrated obstetric care models that address the issue of inappropriate care and lend themselves to public private engagements (PPEs) could play an important role in addressing this challenge.[10] The development of such models could provide building blocks for obstetric care for the proposed National Health Insurance (NHI),[11] which is envisaged as being the strategic purchaser of healthcare services from both the public and private sectors for the entire SA population.
Efforts to improve obstetric care are particularly important because caesarean delivery is a commonly performed surgical procedure, and there is growing local concern about the appropriateness and safety of obstetric care in both the public and private sectors. Development of models for obstetric care could also inform strategies for other medical and surgical disciplines where similar patterns of underservicing in the public sector and overservicing in the private sector may occur. However, the evidence to support the development of such models is limited - a recent scoping review of financial and regulatory interventions to reduce unnecessary caesarean section concluded that the available evidence on the effects of financial and regulatory strategies intended to reduce unnecessary caesarean delivery rates is inconclusive, and more rigorous studies are needed.[12] We carried out research to examine the care and contracting models used by five rural district hospitals in the Western Cape Province to contract private general practitioners (GPs) to provide caesarean delivery services.[13-15] Drawing on insights from the research, this article outlines a potential alternative model for private sector obstetric care with the aim of stimulating discussion by all relevant stakeholders on the development of new obstetric models in SA.
Prior research
The methods and findings of the research that informed this practice article are described in detail elsewhere,[13-15] and we summarise here only the key findings and insights from the research and the thought process in using those insights for proposing an alternative model of private obstetric care.
We undertook descriptive health systems research utilising a mixed-methods study design to describe contracting models adopted by rural district hospitals to contract private GPs for caesarean deliveries. The setting for this research was the Western Cape Province where public-private contracting for caesarean delivery services was already in operation, owing to human resource shortages in rural district hospitals. Five rural district hospitals within one rural district were chosen following engagement with provincial managers and obstetric clinical managers. All had existing contracting arrangements with private GPs. Delivery data from the delivery and theatre registers were collected for the period from 1 April 2021 to 31 March 2022 to capture the profile of deliveries and maternal outcomes of the five hospitals, and 27 semi-structured qualitative interviews were conducted with district managers, hospital-employed doctors and midwives and private GPs to explore their experiences of the contracting arrangements.
All five district hospitals implemented a 'public sector' service model for obstetric care. Pregnant women received their antenatal care via a local primary health clinic, unless triaged as high risk and referred for antenatal care and delivery in a hospital. As none of the hospitals have primary care clinics in their catchment areas that perform vaginal deliveries other than for emergencies during daytime hours, women are admitted to the maternity ward of a local district hospital upon going into labour. The maternity ward is staffed by nurses and midwives, supported by medical officers. Medical officers assess the risks of the expectant mother and make an assessment, based on public sector protocols, as to whether the birth should be via normal vaginal delivery or by caesarean delivery at the district hospital, or whether the level of risk warrants referral to a regional hospital where more specialised expertise is available.
The hospitals varied in the level of GP use (from 100% to 10% of caesarean deliveries)[15] and the contracting models (full-time public employment, and three private in-sourcing models - via locum agencies, sessional contracts and tender contracts) used to secure the services of doctors to assist with obstetric care. Across the study hospitals, the average number of deliveries ranged from 34 to 144 per month, and the caesarean delivery rates ranged from 13.5% to 25.2% - in line with caesarean delivery rates reported at public health facilities in SA, and well below rates of between 74%[7] and 76.9%[8] reported for the private sector. The caesarean delivery rates across the hospitals were not related to the contracting models used, and were not higher in hospitals that made greater use of private GPs - a finding that suggests that private-public partnerships can provide safe and appropriate caesarean delivery care if they are structured appropriately, as was the case at the five study hospitals. The implications of scaling up these models within district hospitals is explored in our previously published articles.[13-15]
The research examined contracting models adopted by rural district hospitals to contract private GPs for caesarean deliveries. In order to be able to use the insights from this research, which was conducted in a specific rural setting, to inform the development of an alternative private obstetric care model for SA as proposed in this article (and to inform the development of alternative models more broadly in other settings), we identified the key underlying features that we believe were critical to the delivery of appropriate care at the five hospitals. Six such key features were identified: (i) a 'risk-based' service model with midwives performing normal vaginal deliveries and medical officers or private GPs managing complicated vaginal deliveries and performing surgical obstetric procedures; (ii) tight clinical control and governance processes adhering to accepted clinical protocols; (iii) a team-based rather than individual provider model of care; (iv) provider remuneration models based on time rather than the number or type of deliveries; ( v) group rather than individual professional liability arrangements; and (vi) processes to monitor outcomes, evaluate performance and apply remedial measures when required, commonly conducted at regular facility mortality and morbidity meetings and national audits by National Committee on Confidential Enquiries into Maternal Deaths (NCCEMD) and National Perinatal Morbidity and Mortality Committee (NaPeMMCo). Although our previous research was specific to rural district hospitals in the Western Cape, these six key features guided the development of an alternative model for other settings in SA.
Potential alternative model
The obstetric care model currently dominant in the private sector is 'individual' obstetrician/gynaecologist (primary provider) driven. It is characterised by women choosing a primary provider, with antenatal care provided by this specialist or a GP, and the baby delivered in a private hospital by this primary provider, who makes the decisions on mode and timing of delivery and provides the postnatal care. The primary provider, anaesthetist, paediatrician, hospital and any other providers all bill separately on a fee-for-service basis. The primary provider assumes responsibility for professional liability at an individual level (which many providers cover by charging an additional 'birthing fee'). Aside from annual quality reports produced by some hospital groups and a requirement to report all maternal and perinatal deaths, clinical governance processes are weak. Furthermore, private obstetric specialists may decide on their own clinical protocols or guidelines. There are strong incentives for delivering via caesarean delivery in this model - caesarean deliveries can be 'scheduled' at a time convenient for the primary provider and the woman, the time costs are shorter and more predictable than for vaginal deliveries and legal risks are perceived to be lower.'[16]
The Department of Health currently licenses 'birthing centres (BCs) as 'healthcare facilities for childbirth where care is provided in the midwifery and wellness model'. The BCs are required to be 'freestanding' and not within a hospital or part of a hospital.[17] Many of these BCs have struggled, as illustrated by the closure of the Genesis Maternity Clinic in Johannesburg, which operated independently from 2009 until 2015, when it was purchased by one of the major hospital groups. The hospital group announced the closure of the clinic in February 2023, due to 'strategic business decisions' based on the inability to expand the services and ensure long-term sustainability of the unit.[18] Utilisation of these BCs and other midwife-based delivery models has been low for a number of reasons. PhD research[19] exploring private sector obstetric, maternal and unborn caring concerns in Cape Town found that competition between the independent midwives and obstetricians who are practicing in fragmented silos, as is the case in the private fee-for-service paradigm, make the 'teamwork' required difficult. The reluctance of specialists to take on the risk of complicated/ emergency births without a full shared view of the patient history and risk profile has resulted in the BCs not been able to secure the necessary backup of specialist obstetricians in the event of complications arising during childbirth. As a result, women have been reluctant to give birth in a situation where specialist back-up is uncertain. The need to transfer to a hospital in the event of an emergency and the failure of medical aids to cover the full costs of these arrangements have also served as deterrents.
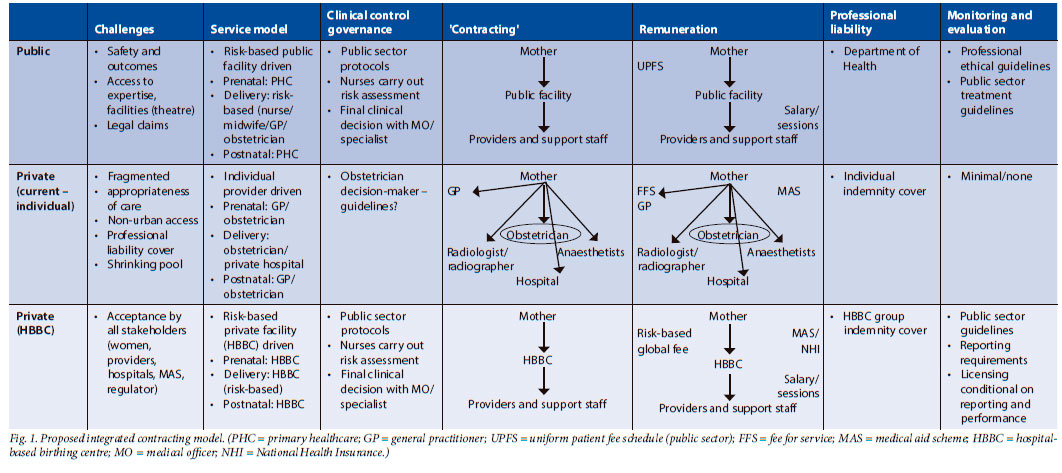
Consideration should be given to developing an alternative model that addresses the concerns related to the BCs and that replicates the public sector care model in the private sector, incorporating the six key features that were identified in our research as key to ensuring appropriate care. This could be done by extending the licensing arrangements of the BCs to allow private hospitals/hospital groups to establish hospital-based birthing centres (HBBCs), and amending the Health Professions Council of SA (HPCSA) ethical rules to allow hospitals to employ or contract with the necessary staff and professionals to provide the full range of services through a risk-based multidisciplinary platform. The key features of the HBBC model are summarised in Fig. 1. For comparison, the current public and dominant 'individual provider' private sector models are also summarised.
The HBBC should operate with a public sectortype multidisciplinary team approach, with nurse/ midwife ward-based care supported by various levels of medical providers (medical officers, registrars doing specialist training and specialist obstetricians) providing back-up where and when needed, according to the risk profile of the mother. The HBBC should be responsible for providing all the pre-atal, delivery and postnatal care. Expectant mothers choosing to give birth through the HBBC model would engage/contract with their HBBC of choice. Upon registration, the expectant mother would undergo a risk assessment (based on public sector protocols) and be placed on a risk-appropriate 'care plan.' A nurse/midwife would be allocated to the expectant mother to oversee/provide care, to ensure continuity of care and comfort to the mother. Low-risk deliveries could take place at the HBBC 'ward', performed by the ward-based nurse/midwife with medical providers providing back-up support. In the event of complications at birth, the mother can be easily transferred to the hospital's high care, theatre and neonatal unit infrastructure.
The HBBCs should be remunerated through a global fee for the full maternal care episode. Different global fees would apply for different care plans based on the assigned risk categories and resources. The care could be financed through private 'out-of-pocket' arrangement or by private health insurance for non-public sector-dependent mothers, and through PPEs for public-sector-dependent mothers. The providers (midwives/medicalofficers/registrars or obstetricians) working at the HBBC should be remunerated on a time basis (full- or part-time employment/per hour/session/monthly), not on a per case or type of delivery basis. The level of remuneration should be commensurate with the level of skill and expertise of the provider. Professional indemnity could be covered by the HBBC on a group basis, and each HBBC should be required to provide reports to a regulated monitoring centre. The HBBCs should be required to be licensed to operate and accredited on an annual basis, with accreditation dependent on performance and compliance with protocols.
The implementation of the HBBC model would require the HPCSA to relax current restrictions on hospitals employing doctors (and specialists). The relaxation of these restrictions would be in alignment with broader policy imperatives such as those emerging from the Competition Commission's Health Market Inquiry[2] and a survey of key stakeholders (although with a limited sample) that indicated support.[20] However, the acceptance and implementation of these kinds of alternative models, which require a move from current individual to team-based models, challenge existing power relations and vested interests and will encounter resistance from some providers. A development strategy based on thorough engagement and 'buy-in' from all stakeholder groups, incremental iterative implementation and offering the alternative model as an additional choice (to providers and mothers), as opposed to simply replacing the current model, would be critical to successful implementation.
The HBBC model could contribute to better maternal and obstetric outcomes in SA via two routes. First, it will offer women an alternative care model in which many of the 'perverse incentives' of the current dominant 'individual provider' model have been removed and which will potentially deliver more appropriate care. Second, it would be more conducive to public-private contracting for obstetric care. The public sector currently does not make use of private sector providers to provide obstetric care for public sector-dependent patients within the private sector. This can be attributed to two main factors. First, the private sector is highly fragmented, and the public sector would need to contract multiple parties (hospital groups, individual providers, radiologists, etc.), making the contracting process complex. [21] Second, the current 'individual provider' private sector care model also makes it difficult for the public sector to exercise control over clinical governance, monitoring and evaluation, and the consequent high level of inappropriate care. Making the HBBC the central - and only - contracting party will simplify and address the concerns about contracting complexity, and create a platform for addressing concerns around clinical governance, monitoring and evaluation and appropriateness of care. The regular audits of maternal perinatal outcomes conducted at facilities and nationally could be co-ordinated at this level and involve all healthcare providers engaged in the care of mothers and newborns in the HBBC.
Conclusion
There are major concerns regarding public and private maternal healthcare in SA. New models for private sector obstetric care that address the inappropriate patterns of care in the sector and allow private sector resources to be mobilised to serve the broader population dependent on the public sector, without replicating those patterns of inappropriate care, could improve obstetric care for all women in the country. Developing, piloting and implementing alternative models of care could also assist in informing the development and implementation of the broader reforms for universal healthcare being envisaged for the country. The potential alternative private sector obstetric care model outlined in this article is aimed at stimulating discussion by all relevant stakeholders on the development of new models for improving obstetric care in the country.
Declaration. None.
Acknowledgements. The authors would like to acknowledge the institutional support to the study authors provided by the South African Medical Research Council (SAMRC), the University of Cape Town and the Clinton Health Access Initiative. We also acknowledge the contributions of Maxie Nel, Ndileka Mbete and Nicole Daniels for reviewing and providing input on the manuscript and to Jud Cornell for her input and assistance in editing the draft.
Author contributions. Conceived and designed the study GS, VB; developed the article: GS, TD, SF, ED; reviewed the article: TD, SF, ED.
Funding. GS is employed on a contractual basis by the SAMRC and NMG Consultants and Actuaries; support in the form of salaries for GS, TD and ED was provided by the SAMRC. TD is employed by the SAMRC. VB is employed by the Clinton Health Access Initiative. None of these institutions had any additional role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Conflicts of interest. None.
References
1. World Bank. World Development Indicators. Jun 18, 2020. https://databank.worldbank.org/home.aspx (accessed 12 March 2024). [ Links ]
2. Competition Commisssion of South Africa. Health Market Inquiry Final Findings and Recommendations Report. 2019. http://www.compcom.co.za/wp-content/uploads/2020/01/Final-Findings-and-recommendations-report-Health-Market-Inquiry.pdf (accessed 12 March 2024). [ Links ]
3. Econex. Health Reform Note 4. Integration of the public and private sectors under a National Health Insurance (NHI) system in SA. July 2010. Stellenbosch: Econex, 2009. [ Links ]
4. National Department of Health. Saving Mothers 2017 - 2019. Seventh report on confidential enquiries into maternal deaths in South Africa. Pretoria: NDoH, 2020. [ Links ]
5. Human Rights Watch. South Africa. 'Stop Making Excuses. Accountability for materntal health care in South Africa. 2011. https://www.hrw.org/report/2011/08/08/stop-making-excuses/accountability-maternal-health-care-south-africa (accessed 12 March 2024). [ Links ]
6. Sobhy S, Arroyo-Manzano D, Murugesu N, et al. Maternal and perinatal mortality and complications associated with caesarean section in low-income and middle-income countries: A systematic review and meta-analysis. Lancet 2019;393(10184):1973-1982. https://doi.org/10.1016/S0140-6736(18)32386-9 [ Links ]
7. Solanki G, Fawcus S, Daviaud E. A cross sectional analytic study of modes of delivery and caesarean section rates in a private health insured South African population. PloS ONE 2019;14(6):e0219020. https://doi.org/10.1371/journal.pone.0219020 [ Links ]
8. Council for Medical Schemes. Epidemiology and trends of caesarean section births in the medical schemes' population, 2015 - 2018. Policy, Research and Monitoring. Research Brief 1 of 2020. February 2020. https://www.medicalschemes.com/files/Research%20Briefs/Caesarean%20section%20births%20-%20Research%20Briei%201%20of%202020.pdf (accessed 12 March 2024). [ Links ]
9. Solanki GC, Cornell JE, Daviaud E, Fawcus S. Caesarean section rates in South Africa: A case study of the health systems challenges for the proposed National Health Insurance. S Afr Med J 2020;110(8):747-750. https://doi.org/10.7196/SAMJ.2020.v110i8.14699. [ Links ]
10. Barber SL, Kumar A, Roubal T, Colombo F, Lorenzoni L. Harnessing the private health sector by using prices as a policy instrument: Lessons learned from South Africa. Health Policy 2018;122(5):558-564. https://doi.org/10.1016/j.healthpol.2018.03.018 [ Links ]
11. South Africa. National Health Insurance Bill. 2019. (B 11-2019). https://www.gov.za/sites/default/files/gcis_document/201908/national-health-insurance-bill-b-11-2019.pdf (accessed 22 January 2022). [ Links ]
12. Opiyo N, Young C, Requejo JH, Erdman J, Bales S, Betrán AP. Reducing unnecessary caesarean sections: Scoping review of financial and regulatory interventions. Reprod Health 2020;17(1):133. https://doi.org/10.1186/s12978-020-00983-y [ Links ]
13. Doherty T, Fawcus S, Daviaud E, Bartmann Y, Solanki G. Experiences of public-private contracting for caesarean delivery in rural district public hospitals: A qualitative interview study. PLOS Glob Pub Health 2023;3(5):e0001335. https://doi.org/10.1371/journal.pgph.0001335 [ Links ]
14. Solanki G, Daviaud E, Fawcus S, Brijlal V, Doherty T. Models using private general practitioners to provide caesarean deliveries at five South African district public hospitals: Insights for public-private contracting for obstetric care in rural areas. Glob Health Act 2023;16(1):2241811. https://doi.org/10.1080/16549716.2023.2241811 [ Links ]
15. Doherty T, Solanki G, Daviaud E, Bartmann Y, Hawkridge A, Fawcus S. Utilisation of private general practitioners to provide caesarean deliveries in five rural district public hospitals in South Africa: A mixed-methods study. BMJ Open 2023;13(3):e067663. https://doi.org/10.1136/bmjopen-2022-067663 [ Links ]
16. Elaraby S, Altieri E, Downe S, et al. Behavioural factors associated with fear of litigation as a driver for the increased use of caesarean sections: A scoping review. BMJ Open 2023;13(4):e070454. https://doi.org/10.1136/bmjopen-2022-070454 [ Links ]
17. KwaZulu-Natal Department of Health. Licensing of Private Health Care Facilities. Public Notice (22/11/2022) Non-payment of annual re-licensing fees. List of licensed facilities. 13 April 2023. https://www.kznhealth.gov.za/Licensing_pvt_health_care_facilities.htm (accessed 12 March 2024). [ Links ]
18. Life Healthcare. Genesis Maternity Clinic Closure. 23 February 2023. https://www.lifehealthcare.co.za/media/3739/webstatement_genesis-closure_feb2023.pdf (accessed 12 March 2024). [ Links ]
19. Daniels NM. Obstetric-risk objects: a multi-site, feminist ethnography of private-sector obstetric, maternal and unborn caring concerns in Cape Town. Doctoral dissertation. University of Cape Town, 2021. https://open.uct.ac.za/handle/11427/35491 (accessed 12 March 2024). [ Links ]
20. Mosam A. Regulating the employment of doctors within the private sector in South Africa. A policy analysis. Research report to Faculty of Health Sciences, University of the Witwatersrand in partial fullfillment for the degree of Master of Public Medicine in field of Public Health. Johannesburg: University of the Witwatersrand, 15 October 2018. https://wiredspace.wits.ac.za/server/api/core/bitstreams/41d756e1-284f-43ba-b24a-6b079df0ca49/content (accessed 12 March 2024). [ Links ]
21. Solanki G, Cornell J, Crisp N, et al. Insights from contracting the private sector for critical care. In: Govender K, George G, Padarath A, Moeti T, eds. South African Health Review 2021. Durban: Health Systems Trust, 2021. https://www.hst.org.za/publications/South%20African%20Health%20Reviews/Chapter8_SAHR21_04022022_OD.pdf (accessed 12 March 2024). [ Links ]
 Correspondence:
Correspondence:
G Solanki
geetesh.solanki@mrc.ac.za
Accepted 29 January 2024


{kind=link}