










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.114 n.3 Pretoria Mar. 2024
http://dx.doi.org/10.7196/SAMJ.2024.v114i3.1315
RESEARCH
Differential management and associations of dyslipidaemia and hypertension by glycaemic status in urban South Africans
N PeerI; L Kotzé-HörstmannII; J HillIII; A-P KengneIV
IMB ChB, PhD; South African Medical Research Council, Cape Town, South Africa
IIPhD; South African Medical Research Council, Cape Town, South Africa
IIIMPH, PhD; South African Medical Research Council, Cape Town, South Africa
IVMD, PhD; South African Medical Research Council, Cape Town, South Africa
ABSTRACT
BACKGROUND: Dyslipidaemia and hypertension care have not been reported in large samples of community-based participants with known diabetes (KD) nor compared with individuals at high risk for diabetes.
OBJECTIVES: To describe the management and associations of dyslipidaemia and hypertension in adults with KD, newly diagnosed diabetes (NDD) and normoglycaemia.
METHODS: This urban population-based cross-sectional study comprised participants with KD, NDD and normoglycaemia. Participants at high risk for diabetes but without KD underwent oral glucose tolerance tests; those who were subsequently classified as NDD or normoglycaemic were included in this study. Data collection comprised administered questionnaires, clinical measurements and biochemical analyses. Multivariable logistic regressions determined the associations with hypertension and dyslipidaemia management in separate models.
RESULTS: Among 618 participants (82% women), aged median 58 years, there were 339 participants with KD, 70 with NDD and 209 with normoglycaemia. Prevalence of hypertension (BP >140/90 mmHg or on treatment) and dyslipidaemia (raised low-density lipoprotein cholesterol >3 mmol/L or on treatment) was highest in KD (89% and 83%) compared with NDD (64% and 74%) and normoglycaemia (66% for both) (p<0.001). Detected or known hypertension was highest in KD (97.4%), followed by NDD (88.9%) and normoglycaemia (80.3%). Among participants with known or detected hypertension, those with KD were most likely to be treated (90.2%) compared with NDD (77.5%) and normoglycaemia (74.5.%). Hypertension control among participants on treatment was highest in KD (69.5%) compared with NDD (51.6%) and normoglycaemia (61.0%). Participants with KD had significantly higher rates of previously detected dyslipidaemia (85.1%) compared with NDD (36.5%) and normoglycaemia (35.5%). KD participants were also more likely to be treated for their previously detected dyslipidaemia (85.4%) and to be controlled when on treatment (56.3%) compared with their counterparts (NDD: 63.2% and 33.3%, normoglycaemia: 61.2% and 43.3%, respectively). Diabetes control was poor; only 20% of those with KD had HbA1c <7%. In the regression models, compared with normoglycaemia, KD was associated with hypertension detection (odds ratio (OR) 6.91, 95% confidence interval (CI) 2.25 - 21.22) and control (OR 2.05, 95% CI 1.04 - 4.02). KD compared with normoglycaemia was associated with dyslipidaemia detection (OR 10.29, 95% CI 5.21 - 20.32) and treatment (OR 3.94, 95% CI 1.68 - 9.27). Sociodemographic and cardiovascular disease risk factors were generally not associated with hypertension or dyslipidaemia management
CONCLUSION: Albeit that diabetes control was poor and required better management, dyslipidaemia and hypertension prevalence were higher and better managed in KD than NDD and normoglycaemia. Different approaches are required to improve glucose control in KD, better identify NDD and monitor and prevent diabetes in high-risk individuals. Also important would be to improve care of hypertension and dyslipidaemia in those without KD.
The burden of type 2 diabetes mellitus (hereafter referred to as diabetes), at 15% among >25-year-old South Africans, is high and rising.[1] This is of concern because of the heavy health burden associated with diabetes, i.e. the macro- and microvascular complications that are frequently debilitating and contribute to high levels of morbidity and mortality in the country.[2] Moreover, in South Africa (SA), diabetes-related morbidity and mortality occur most often in working-age individuals who are also family breadwinners.[3] This poses a serious threat, not only to health but also to economic development, and further exacerbates social inequities. Notably, diabetes is the second leading cause of mortality in the country after tuberculosis, accounting for almost 6% of deaths in 2017.[4] Therefore, optimal diabetes management with effective intervention strategies is crucial to prevent adverse outcomes.
Diabetes is known to commonly cluster with other cardiovascular disease (CVD) risk factors such as dyslipidaemia and hypertension, which exponentially increases the risk of complications and CVDs.[5] Indeed, a combination of even modest elevations in blood pressure (BP), plasma lipids and blood glucose confer substantial excess risk for CVD and death.[6] Furthermore, the presence of diabetes is believed to confer an equivalent risk to already having coronary heart disease, which underlines the seriousness of this condition.[5] This highlights the importance of optimal control of all CVD risk factors, including glucose levels, in individuals with diabetes.
Nonetheless, it is equally important to optimise hypertension and dyslipidaemia care in individuals without known diabetes (KD) but who are at high risk for diabetes and have hypertension or dyslipidaemia. Few, if any, community-based studies in SA have examined the management of cardiometabolic diseases in individuals at high risk for diabetes. To our knowledge, no SA study has described the level of care for hypertension and dyslipidaemia in a large sample of community-based participants with KD and compared this with individuals at high risk for diabetes. Neither have sociodemographic factors nor the care of cardiometabolic comorbidities that may influence the detection, treatment and control of dyslipidaemia and hypertension been assessed. The present study describes the management and associations of dyslipidaemia and hypertension in 25 - 65-year-old participants with KD, newly diagnosed diabetes (NDD) and normoglycaemia.
Methods
Study design and participants
This cross-sectional study comprised 25 - 65-year-old participants (i) without KD recruited for the SA Diabetes Prevention Programme (SA-DPP), and (ii) with KD recruited from the same communities as the latter study. The SA-DPP targeted black and mixed ancestry (Khoisan, white, black and Malay heritage) participants who were at high risk for diabetes and resided in 16 communities in Cape Town, SA. A convenience sample was recruited between 2017 and 2019; the study methodology has been described in detail previously.[7] High-risk participants were identified on screening using the African Diabetes Risk Score (ADRS), a previously validated tool in SA that incorporates age, hypertension and waist circumference.[7] Eligibility for screening was as follows: 25 - 65 years of age, no previous diagnosis of diabetes, not currently pregnant or breastfeeding and not in receipt of cancer or tuberculosis treatment within the past 3 months.
Additionally, individuals from the same communities who self-reported having diabetes (KD) were included specifically for this analysis. Participants with KD underwent similar assessments, excluding the oral glucose tolerance test (OGTT), as those in the SA-DPP.
Data collection
Data were captured electronically on tablets and loaded into an online database. Data collection, conducted by trained fieldworkers, comprised administered questionnaires, clinical examinations and biochemical assessments. The questionnaires included sociodemographic characteristics, medical history and lifestyle behaviours pertaining to alcohol and tobacco use, and sedentary behaviours.
Clinical assessments, conducted using standardised techniques, included anthropometry and BP measurements. Briefly, height (m) and body weight (kg) were assessed using a SECA stadiometer and a SECA digital scale, respectively, while waist (cm) and hip (cm) circumferences were measured using a flexible non-elastic measuring tape in participants who were barefoot and wearing light clothing. Three BP measurements (Omron M6W automated cuff; Omron, Japan) were taken at 2-minute intervals after the participant had been seated for 5 minutes, and the mean BP was calculated using the average of the second and third measurements.
After an overnight fast of at least 10 hours, participants without KD underwent an OGTT. Blood samples were drawn at baseline, followed by the administration of a 75 g glucose load, and drawing of blood samples at 120 minutes for the OGTTs.[8] Blood samples were kept on ice and transported to the laboratory within 6 hours to be processed. Plasma glucose levels were measured by hexokinase method (Beckman AU, South Africa). Glycated haemoglobin (HbA1c) was analysed with high-performance liquid chromatography (Biorad Variant Turbo, South Africa). Serum lipid profiles including low-density lipoprotein cholesterol (LDL-C) were determined using the Beckman Coulter AU 5800 Clinical chemistry analysers (Beckman Coulter Inc., USA).
Definitions
Age was dichotomised into two categories (</>55 years), taking the median age of participants into consideration. Smoking was defined as current daily or occasional use of tobacco products such as cigarettes, cigars and pipes. Alcohol consumption was defined as the intake of any alcohol product within the last 12 months. Sedentary time >7.5 hours (>450 minutes) per week was defined as physical inactivity.[9]
Body mass index (BMI), calculated as weight in kilograms divided by height in metres squared (kg/m2), categorised participants as underweight or normal weight (<25 kg/m2), overweight (25 - 29.9 kg/ m2) and obese (BMI >30 kg/m2).[10] Central obesity was defined as waist circumference >94 cm for men and >80 cm for women,[11] waist-to-hip ratio (WHR) >0.9 for men and >0.85 for women[11] and waist-to-height ratio as >0.5.[12]
Hypertension was defined as systolic BP >140 mmHg and/or diastolic BP >90 mmHg, self-reporting a hypertension diagnosis or being on antihypertension medication.[13] Among participants with hypertension, detection was defined as being previously informed by a doctor or nurse of their high BP status. Hypertension treatment was described as the intake of antihypertensive medication in participants (i) who were aware of their diagnosis or (ii) with hypertension. Hypertension control was defined as BP <140/90 mmHg in participants (i) on antihypertensive medication or (ii) with hypertension.
Diabetes was defined according to the 1998 World Health Organization (WHO) definition of fasting plasma glucose >7.0 mmol/L and/ or 2-hour post-glucose load >11.1 mmol/L or previously diagnosed with diabetes or on medication for the condition.[8] Normoglycaemia was defined as a fasting plasma glucose <6.1 mmol/L and 2-hour post-glucose load <7.8 mmol/L and HbA1c <5.7%. Diabetes control in KD was defined as HbA1c <7.0%.
Dyslipidaemia was defined as LDL-C >3.0 mmol/L, having a previous diagnosis of dyslipidaemia, or taking lipid-lowering drugs, while other components were defined as total cholesterol (TC) >5 mmol/L, high-density lipoprotein cholesterol (HDL-C) <1.2 mmol/L, HDL-C/TC ratio <20% and triglycerides >1.5 mmol/L.[14] Among participants with dyslipidaemia, detection was defined as being previously informed by a doctor or nurse of having high LDL-C levels. Dyslipidaemia treatment was described as taking anti-lipid (statin) medication in participants (i) who were aware of their diagnosis or (ii) with dyslipidaemia. Dyslipidaemia control was defined as LDL-C <3 in participants (i) on statin medication or (ii) with dyslipidaemia. The metabolic syndrome was defined by the harmonised Joint Interim Statement (JIS) criteria.[15]
Statistical analysis
Data analyses were performed in IBM SPSS Statistics for Windows (Version 27.0: IBM Corp., USA). Data were evaluated for normality according to Kolmogorov-Smirnov and Shapiro-Wilk tests. Continuous variables were compared by independent samples Kruskal-Wallis H tests as these variables were overall not normally distributed and accordingly presented as median and 25th - 75th percentiles. Categorical variables were compared using X2 tests and are presented as absolute counts (n) and percentage (%).
Multiple logistic regressions were conducted using a stepwise backward regression approach to determine the associations with detection, treatment and control of dyslipidaemia and hypertension. Treatment was assessed among participants who were detected, and control among those who were treated. The results are presented as odds ratios (ORs) and 95% confidence intervals (CIs). Stepwise backward regression allows the model to iteratively assess the significance of each variable and removes those that do not significantly contribute to the prediction of the outcome, resulting in a more parsimonious model. Models were adjusted for sociodemographic characteristics (age, gender, ethnicity, education, employment status, income and housing type), behavioural risk factors (sedentary time, smoking and alcohol use), obesity and management of other cardiometabolic diseases. This approach ensures that the final model includes the most relevant predictors. P<0.05 was considered statistically significant.
Ethics approval was obtained from the South African Medical Research Council's (SAMRC) Human Research Ethics Committee (ref. no. EC018-7/2015). All participants signed informed consent.
Results
Sociodemographic characteristics
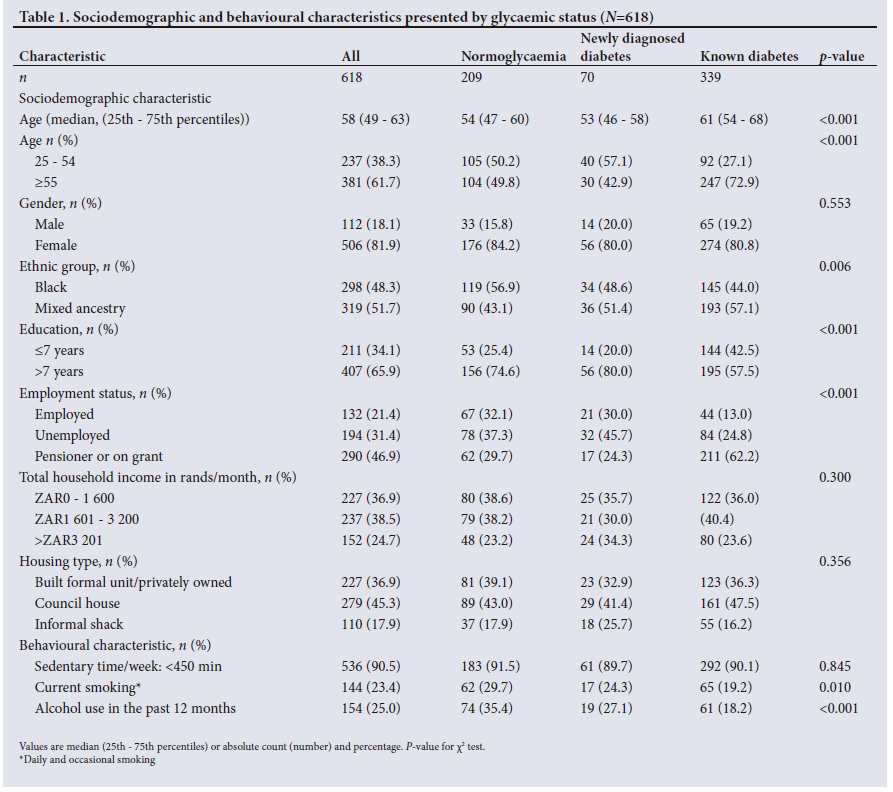
Among 618 participants (82% women), median age 58 years, and with a similar distribution by population group (48% black, 52% mixed ancestry), there were 339 participants with KD, 70 with NDD and 209 with normoglycaemia (Table 1). Participants with KD were significantly older than their counterparts (61 years v. 53 and 54 years, respectively). Overall, only a fifth (21%) of participants were employed, while the largest proportion were pensioners or receiving a social grant (47%); the majority (75%) reported a household income <R3 200/month (about USD187). A quarter of participants had consumed alcohol in the previous 12 months (25%) and a similar proportion (23%) were current smokers. Alcohol and smoking rates were lower in participants with KD (18% and 19%) compared with normoglycaemia (35% and 30%) and NDD (27% and 24%), respectively.
Cardiometabolic characteristics
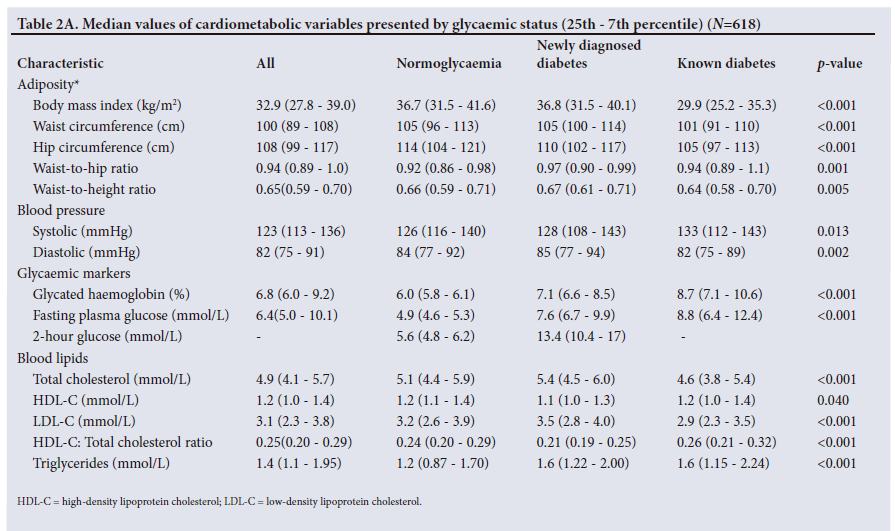
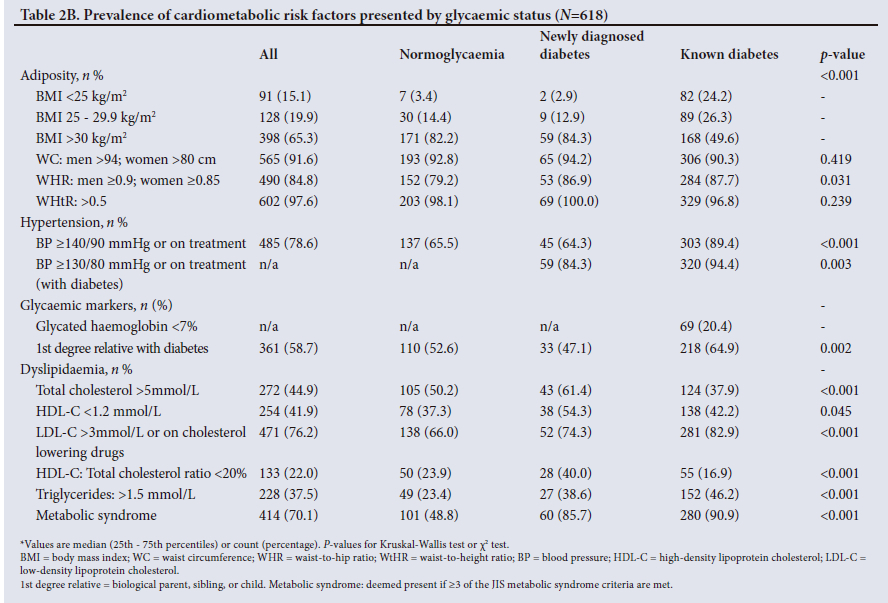
Table 2A describes the median values of the cardiometabolic variables, and Table 2B details the prevalence of cardiometabolic risk factors by glycaemic status. In Table 2B, compared with those with normoglycaemia (82%) and NDD (84%), participants with KD (50%) had significantly lower rates of BMI >30 kg/m2 (p<0.001), which is likely a function of the study inclusion criteria for high-risk participants. Hypertension prevalence was highest in KD (89%) compared with normoglycaemia (66%) and NDD (64%) (p<0.001). KD participants also had higher rates of LDL-C >3 mmol/L or taking lipid treatment and triglycerides (83% and 46%, respectively) than those with normoglycaemia (66% and 23%) and NDD (74% and 39%) (both p<0.001). Unsurprisingly, metabolic syndrome prevalence was highest among those with KD (91%) and NDD (86%) compared with normoglycaemia (49%) (p<0.001). Diabetes control was low in KD, with only 20% achieving HbA1c <7%. Diabetes control was lower in younger compared with older participants with KD (<54 years: 15.5% v. >55 years: 23.1%) (data not shown).
Management of comorbid dyslipidaemia and hypertension
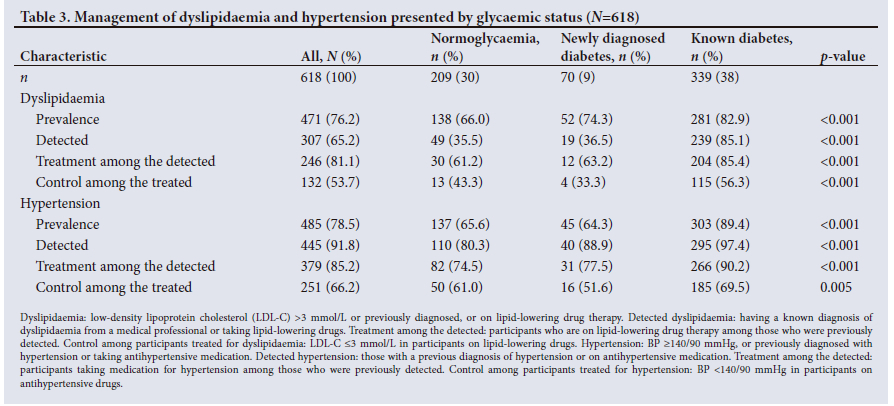
Participants with KD had significantly higher rates of previously detected dyslipidaemia (85.1%) compared with NDD (36.5%) and normoglycaemia (35.5%), as illustrated in Table 3. KD participants were also more likely to be treated for their previously detected dyslipidaemia (85.4%) and to be controlled when on treatment (56.3%) compared with their counterparts (NDD: 63.2% and 33.3%, normoglycaemia: 61.2% and 43.3%, respectively).
As demonstrated in Table 3, detected or known hypertension was highest in KD (97.4%), followed by NDD (88.9%) and normoglycaemia (80.3%). Among participants with known or detected hypertension, those with KD were most likely to be treated (90.2%) compared with NDD (77.5%) and normoglycaemia (74.5.%). Hypertension control among participants on treatment was highest in KD (69.5%) compared with NDD (51.6%) and normoglycaemia (61.0%). Nevertheless, when using the lower BP cut-point of <130/80 mmHg recommended for optimal hypertension control in KD,[13,16] the control rates decreased markedly to 30% among those treated (data not shown).
Factors associated with care of comorbid dyslipidaemia and hypertension
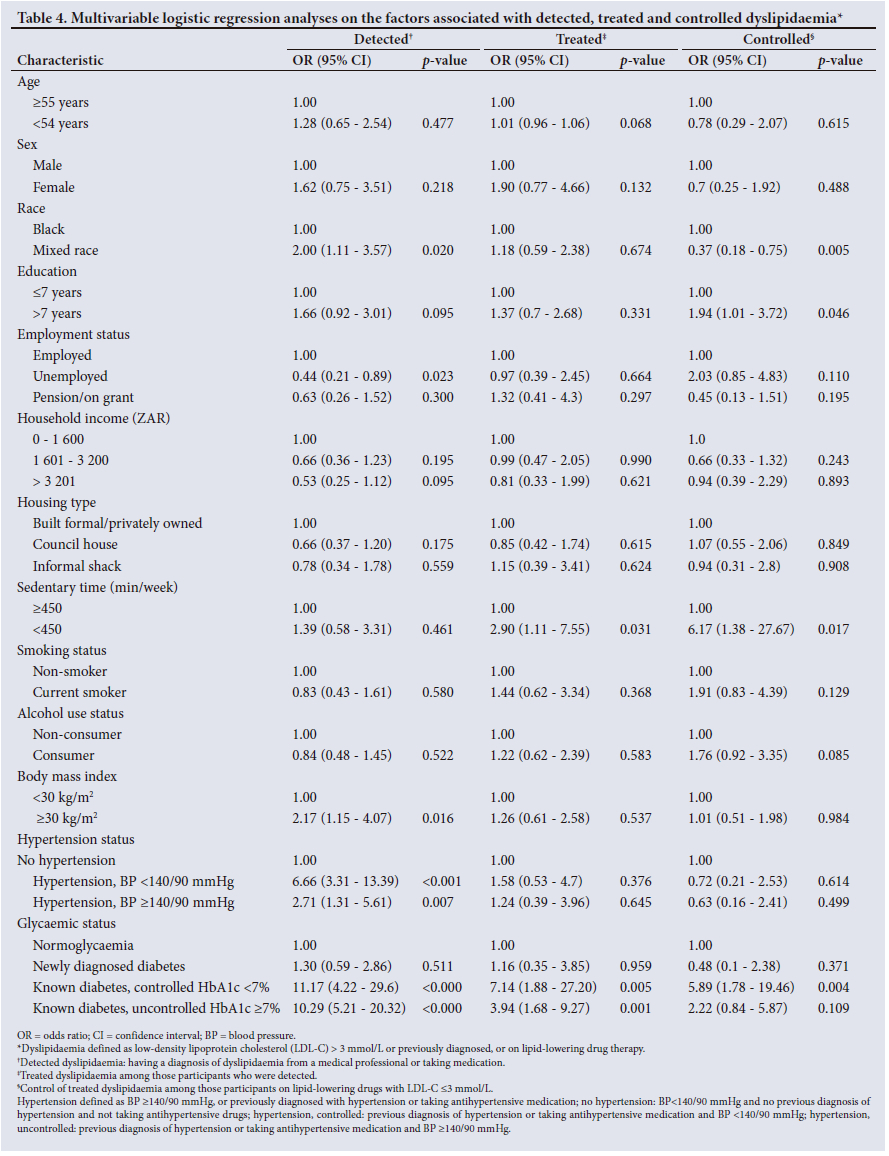
In the multivariable logistic regression analyses, detection of dyslipidaemia was higher in mixed ancestry v. black participants (OR 2.00, 95% CI 1.11 - 3.57), the employed v. unemployed, and with obesity v. non-obese (OR 2.17, 95% CI 1.15 - 4.07) (Table 4). Participants with hypertension, compared with those without, were more likely to have detected dyslipidaemia with the odds greater for controlled (OR 6.66, 95% CI 3.31 - 13.39) v. uncontrolled hypertension (OR 2.71 95% CI 1.31 - 5.61). KD, both controlled and uncontrolled, v. normoglycaemia was associated with detected dyslipidaemia; the greatest odds were for controlled KD (OR 11.17, 95% CI 4.22 - 29.6).
The likelihood of being treated for dyslipidaemia among those who were detected was associated with being less sedentary (OR 2.9, 95% CI 1.11 - 7.55) and having KD, both controlled (OR 7.14, 95% CI: 1.88 - 27.2) and uncontrolled (OR 3.94, 95% CI 1.68 - 9.27) (Table 4). Dyslipidaemia control among those who were treated was lower in mixed ancestry v. black participants (OR 0.37, 95% CI 0.18 - 0.75) and higher in those with >7 years of education (OR 1.94, 95% CI 1.01 - 3.72) and who were less sedentary (OR 6.17, 95% CI 1.38 -27.67). For comorbidities, only controlled KD (OR 5.89, 95% CI 1.78 - 19.46) was associated with controlled dyslipidaemia.
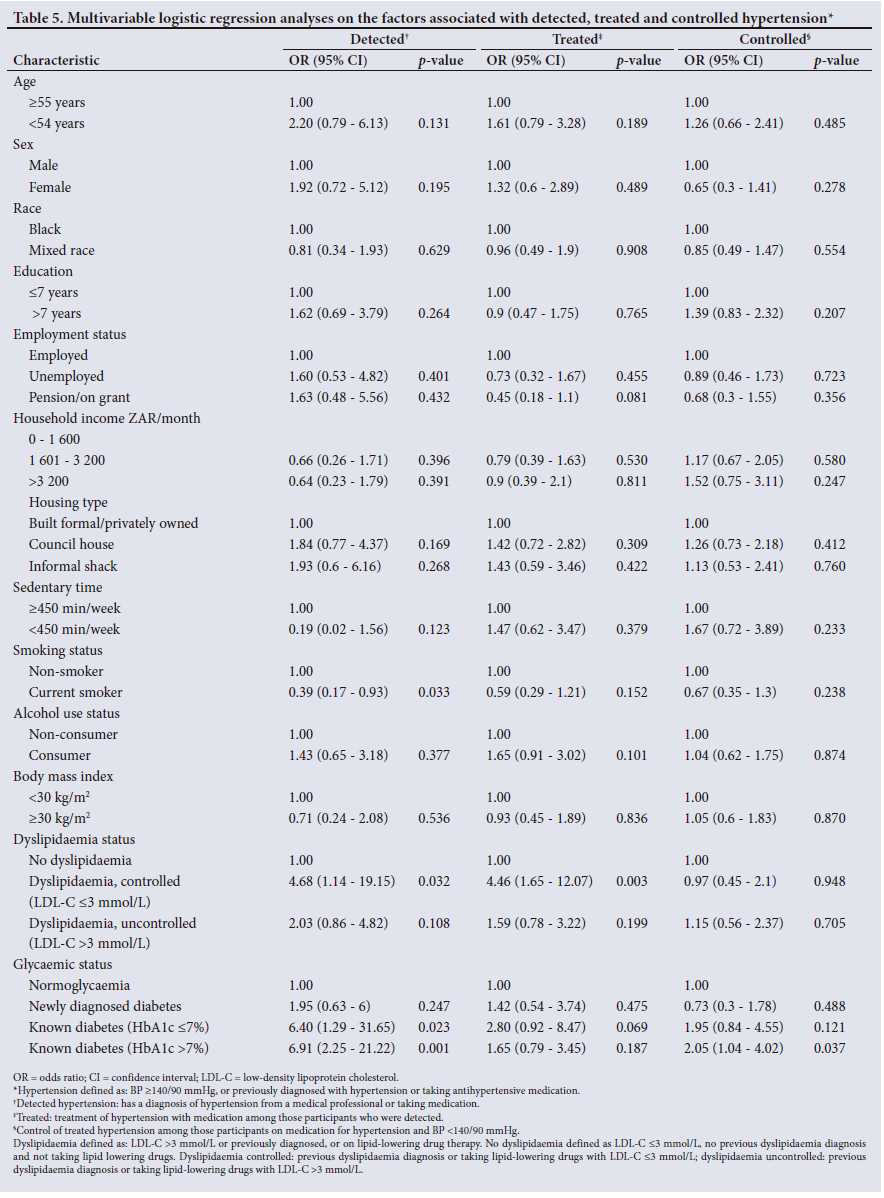
Detection of hypertension was higher in participants with controlled dyslipidaemia compared to those without dyslipidaemia (OR 4.68, 95% CI 1.14 - 19.15), and in KD, both controlled (OR 6.4, 95% CI 1.29 - 31.65) and uncontrolled (OR 6.91, 95% CI 2.25 -21.22) (Table 5). Current smokers v. non-smokers were less likely to have their hypertension detected (OR 0.39, 95% CI 0.17 - 0.93). The likelihood of being treated for hypertension, once detected, was only associated with controlled dyslipidaemia v. no dyslipidaemia (OR 4.46, 95% CI 1.65 - 12.07). Hypertension control among those treated was better in participants with uncontrolled KD (HbA1c >7%) v. normoglycaemia (OR: 2.05, 95% CI 1.04 - 4.02).
Discussion
To our knowledge, this is the first community-based study to describe the management and associations of dyslipidaemia and hypertension by glycaemic status in urban South Africans. This study generally highlights the better management of cardiometabolic comorbidities in the presence of two or more conditions, and if the comorbidity is controlled. Dyslipidaemia detection was more likely in the presence of hypertension and KD, while dyslipidaemia treatment was better with KD, and dyslipidaemia control was associated with controlled KD. Hypertension detection was higher in participants with controlled dyslipidaemia and KD, hypertension treatment was better with controlled dyslipidaemia, while hypertension control was related to uncontrolled KD.
These study findings emphasise the better management of cardiometabolic comorbidities in participants who were likely in regular contact with healthcare services. Participants with KD generally had better management of their dyslipidaemia and hypertension than their counterparts. Although these comparisons were done using general cut-off points for optimal control and not those specific for KD, the better detection and treatment of hypertension and dyslipidaemia in KD compared with their counterparts is unsurprising. The guidelines on diabetes care emphasise the need for greater rigour in the management of hypertension and dyslipidaemia in patients with, rather than without, diabetes. For example, the SA Department of Health primary care guidelines dictate that 10 mg simvastatin should be given to diabetes patients irrespective of their cholesterol level if they have CVD, hypertension, obesity, are >40 years old and/or smoke.[17]
It is concerning that a high proportion (about two-thirds or more) of participants who identified as high risk for diabetes had dyslipidaemia but low rates of detection, treatment and control. Additionally, despite high rates of detection, hypertension treatment and control were suboptimal in these high-risk individuals. A community-based study conducted a decade ago in similar townships in Cape Town reported poor control of diabetes, hypertension and dyslipidaemia and attests to the longstanding nature of this problem.[18-20] While the SA government has acknowledged the need to address the rising burden of CVD risk factors with policies and guidelines related to the control of these risk factors being developed, translating them into effective programmes remains elusive and challenging.[21]
Most disturbing were the low rates of diabetes control, with only one in five KD patients controlled; notably, this was despite their better rates of dyslipidaemia and hypertension control compared with their counterparts. That the majority (three-quarters) of KD participants with treated dyslipidaemia and hypertension had these controlled while diabetes was poorly controlled underscores the difficulty in achieving optimal glucose control and the need for innovative strategies to improve care. Poor glucose control has been reported in other SA studies; only 27% of patients treated for diabetes at 12 primary care clinics in Tshwane had HbA1c <7%,[22] and even fewer patients were controlled in other centres (<11%).[23,24]
Attaining and maintaining optimal diabetes management is a complex process influenced by healthcare systems (e.g. overcrowded facilities), healthcare provider (e.g. inertia in prescribing insulin when required) and patient factors (e.g. non-adherence to medication, diet, etc.),[3] with no single best approach identified for ideal care.[24] However, it is the responsibility of the healthcare system to lead the programme of care for diabetes and other chronic diseases.[24] The low levels of diabetes control in this study underscore the failure of the healthcare system in SA to meet the needs of individuals with diabetes. Despite the high burden of chronic diseases, including multimorbidity, the SA healthcare system is designed to manage mainly acute conditions. The healthcare system needs to adapt to address the challenges linked to the ever-increasing demand for chronic care provision.[25] Improvements in outcomes require adjustments to the process of care; however, the challenge is to identify the appropriate programme to improve the quality and efficiency of diabetes care.
Optimal chronic disease care, particularly for the diabetes patient, requires a holistic approach beyond the care currently provided by the SA healthcare system. This involves a refocusing of the management strategy to a community-based approach rather than the current facility-based model.[26] Patients with diabetes and other cardiometabolic diseases likely require constant education, engagement, encouragement and support to maintain healthy lifestyles. These may be provided using a chronic care model where close linkages exist between the healthcare system and community activities.[25] Such a patient-centred approach with a focus on patient self-efficacy for self-management is crucial for successful behavioural change relating to diet, physical activity, adherence to medication, etc. A different model of care is urgently needed to improve cardiometabolic disease control in this study population, and implementing such a strategy may likely improve their disease outcomes.
Participants with KD had significantly higher triglyceride levels compared with those with normoglycaemia, which likely reflects the dyslipidaemia pattern associated with diabetes, i.e. high triglyceride and low HDL-C levels.[27] However, HDL-C levels in participants with KD were similar to those with normoglycaemia, which may be a function of the significantly higher obesity levels in the latter. The dyslipidaemia pattern linked to obesity is one of atherogenic dyslipidaemia, similar to diabetes, and characterised by high triglycerides and low HDL-C levels.[27] Notably, participants with NDD, who had similar BMI levels to those with normoglycaemia, had the characteristic pattern of atherogenic dyslipidaemia compared with the latter, i.e. higher triglyceride and lower HDL-C levels. Unlike dyslipidaemia, there were no significant differences in the detection, treatment and control of hypertension by population group. Hypertension was widespread in both communities (mixed ancestry: 57 - 58%, black: 41 - 44%),[28] which may account for the similarities in management. Interestingly, although hypertension screening was more likely with KD, this did not translate into higher rates of treatment among those detected with KD compared with their counterparts. Nevertheless, hypertension control among the detected was more likely in participants with KD, albeit uncontrolled and not controlled KD. This is likely a function of the low numbers of controlled KD (n=69) and even fewer participants with controlled hypertension in this group.
The absence of a significant association between sedentary activity and hypertension management is unsurprising, because the former is not considered a predictor of care. Similarly, because of free access to hypertension care in SA in the public health sector, neither was an association between unemployment and hypertension expected. The significant association of uncontrolled diabetes with controlled hypertension is likely a spurious finding and should be explored in studies with larger sample sizes.
Strengths and limitations
The inclusion of a large sample of community-based participants, particularly with diabetes, is a strength of this study, which enabled exploration of cardiometabolic disease care in free-living individuals. The low proportion of men (18%) was unsurprising and is a characteristic of epidemiological studies in SA, likely due to their reluctance to participate. This was a convenience sample, which may reflect self-selection of participants who were more concerned about their health, and hence were better managed for their cardiometabolic diseases, with more frequent contact with healthcare services. Due to small numbers, the study was likely underpowered for some subgroup analyses, particularly in participants with NDD. The BP described was measured at a single visit, which may have led to the overestimation of hypertension. Nevertheless, the SA-DPP participants had their BPs measured during the community-based screening phase where raised BP levels would have identified them as being at high risk and for potential inclusion in this study. The findings of this study are specific for high-risk populations and may not be generalised to low-risk individuals receiving care for a single cardiometabolic disease, e.g. a young hypertensive patient with no other CVD risk factors. The influence of the healthcare service, health provider and patient factors were not explored in this study, which would likely have provided greater insights into the barriers and facilitators of cardiometabolic disease care. However, that was beyond the scope of the current study, and most contributors in this setting are already well established.[3]
Conclusion
Diabetes control was suboptimal, and requires better management in participants with KD. Nevertheless, hypertension and dyslipidaemia were higher and better managed in KD than their counterparts, likely because of their regular contact with healthcare services for their diabetes management. This highlights the need for different strategies, with possibly an emphasis on a community-based chronic care model and patient self-management. This may lead to improvements in glucose control in KD, earlier identification of NDD and closer monitoring and prevention of diabetes in high-risk individuals. It would also be important to improve care of hypertension and dyslipidaemia in those without KD. Otherwise, the inability to improve chronic care provision for cardiometabolic diseases in SA will possibly further compromise sustainable economic development and equitable outcomes as the cardiometabolic disease epidemic escalates in the country.
Availability of data and material
Data used for this study are from baseline evaluation of the ongoing SA-DPP and are not available for sharing until trial completion. Prof. Andre-Pascal Kengne may be contacted on Andre.Kengne@mrc.ac.za for further information.
Declaration. None.
Acknowledgements. The authors thank the SA-DPP investigators, staff and trial participants for their hard work and dedication to the trial.
Author contributions. Manuscript conception: APK, NP; acquisition of data: JH, APK; data cleaning, analysis and preparation of tables and figures: LKH; drafting of the manuscript: NP, LKH; critical revision of the manuscript: JH, APK; approval of the final version: all co-authors.
Funding. The SA-DPP study was funded by the SAMRC through baseline allocation to the Non-Communicable Diseases Research Unit.
Conflicts of interest. None.
References
1. Pheiffer C, Pillay-van Wyk V, Turawa E, et al Prevalence of type 2 diabetes in South Africa: A systematic review and meta-analysis. Int J Environ Res Public Health 2021;18(11):5686. https://doi.org/10.3390/ijerphl8115868 [ Links ]
2. Bradshaw D, Norman R, Pieterse D, Levitt NS. Estimating the burden of disease attributable to diabetes in South Africa in 2000. S Afr Med J 2007*97(8 Pt 2):700-706. [ Links ]
3. Peer N, Baatiema L, Kengne AP. Ischaemic heart disease, stroke, and their cardiometabolic risk factors in Africa: Current challenges and outlook for the future. Expert Rev Cardiovasc Ther 2021;19(2):129-140. https://doi.orgl0.1080/14779072.2021.1855975 [ Links ]
4. Statistics South Africa. Mortality and causes of death in South Africa: Findings from death notification 2017. Pretoria: Stats SA, 2020. [ Links ]
5. Kengne AP, Amoah AG, Mbanya JC. Cardiovascular complications of diabetes mellitus in sub-Saharan Africa. Circulation 2005;112(23):3592-3601. https://doi.orgl0.1161/CIRCULATIONAHA.105.544312 [ Links ]
6. Wilson PW, D'Agostino RB, Parise H, Sullivan L, Meigs JB. Metabolic syndrome as a precursor of cardiovascular disease and type 2 diabetes mellitus. Circulation 2005;112(20):3066-3072. https://doi.orgl0.1161/CIRCULATIONAHA.105.539528. [ Links ]
7. Hill J, Peer N, Jonathan D, et al. Findings from community-based screenings for type 2 diabetes mellitus in at-risk communities in Cape Town, South Africa: A pilot study. Int J Environ Res Public Health 2020;17(8):2876. https://doi.orgl0.3390/ijerphl7082876 [ Links ]
8. World Health Organization. Definition, diagnosis and classification of diabetes mellitus and its complications: Report of a WHO consultation. Geneva: WHO, 1999. https://doi.org10.1002/(SICI)1096-9136(199807)15:7<539::AID-DIA668>3.0.CO;2-S [ Links ]
9. Ku PW, Steptoe A, Liao Y, Hsueh MC, Chen LJ. A cut-off of daily sedentary time and all-cause mortality in adults: Ameta-regression an alysis involving more than 1 million participants. BMC Med 2018; 16(1):74. https://doi.org/10.1186/s12916-018-1062-2 [ Links ]
10. World Health Organization. Obesity: Preventing and managing the global epidemic: Report of a WHO consultation. Geneva: WHO, 2000. [ Links ]
11. World Health Organization. Waist circumference and waist-hip ratio: Report of a WHO expert consultation, Geneva, 8 - 11 December 2008. Geneva: WHO, 2011. [ Links ]
12. Ashwell M, Hsieh SD. Six reasons why the waist-to-height ratio is a rapid and effective global indicator for health risks of obesity and how its use could simplify the international public health message on obesity. Int J Food Sci Nutrition 2005;56(5):303-307. https://doi.org10.1080/09637480500195066 [ Links ]
13. Williams B, Mancia G, Spiering W, et al. 2018 ESC/ESH guidelines for the management of arterial hypertension. Eur Heart J 2018;39(33):3021-3104. https://doi.org10.1093/eurheartj/ehy339 [ Links ]
14. Klug E, Raal FJ, Marais AD, et al. South African dyslipidaemia guideline consensus statement: 2018 update. A joint statement from the South African Heart Association (SA Heart) and the Lipid and Atherosclerosis Society of Southern Africa (LASSA). S Afr Med J 2018;108(11b):973-1000. https://doi.org/10.7196/SAMJ.2018.v108i11.13383 [ Links ]
15. Alberti KG, Eckel RH, Grundy SM, et al. Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009;120(16):1640-1645. https://doi.org10.1161/CIRCULATIONAHA.109.192644 [ Links ]
16. Anwer Z, Sharma RK, Garg VK, Kumar N, Kumari A. Hypertension management in diabetic patients. Eur Rev Med Pharmacol Sci 2011;15(11):1256-1263. [ Links ]
17. National Department of Health. Primary Care 101: Symptom-based integrated approach to the adult in primary care. Pretoria: NDoH, 2014. [ Links ]
18. Peer N, Steyn K, Lombard C, et al. Rising diabetes prevalence among urban-dwelling black South Africans. PloS ONE 2012;7(9):e43336. https://doi.org10.1371/journal.pone.0043336 [ Links ]
19. Peer N, Steyn K, Lombard C, Gwebushe N, Levitt NS. A high burden of hypertension in the urban black population of Cape Town: The cardiovascular risk in black South Africans (CRIBSA) Study. PloS ONE 2013;8(11):e78567. https://doi.org10.1371/journal.pone.0078567 [ Links ]
20. Peer N, Steyn K, Lombard C, Gaziano T, Levitt N. Alarming rise in prevalence of atherogenic dyslipidaemia in the black population of Cape Town: The cardiovascular risk in black South Africans (CRIBSA) study. Eur J Prev Cardiol 2014;21(12):1549-1556. https://doi.org10.1177/2047487313497865.Epub 2013 Jul 23 [ Links ]
21. Puoane T, Tsolekile L, Sanders D, Parker W. Chronic non-communicable diseases. In: South African Health Review 2008. Durban: Health Systems Trust, 2008. http://www.hst.org.za/uploads/files/chap5_08.pdf (accessed 24 July 2012). [ Links ]
22. Webb EM, Rheeder P, van Zyl DG. Diabetes care and complications in primary care in the Tshwane district of South Africa. Primary Care Diabetes 2015;9(2):147-154. https://doi.org10.1016/j.pcd.2014.05.002 [ Links ]
23. Pillay S, Mahomed F, Aldous C. Diabetic patients served at a regional level hospital: What is their clinical picture? J Endocrin Metabol Diabetes. JEMDSA 2015;20(1):60-66. https://doi.org/10.1080/16089677.2015.1030856 [ Links ]
24. Katz I, Schneider H, Shezi Z, et al. Managing type 2 diabetes in Soweto - the South African Chronic Disease Outreach Program experience. Primary Care Diabetes 2009;3(3):157-164. https://doi.org10.1016/j.pcd.2009.06.007 [ Links ]
25. Webb EM, Rheeder P, Wolvaardt JE. The ability of primary healthcare clinics to provide quality diabetes care: An audit. Afr J Prim Health Care Fam Med 2019;11(1):e1-e6. https://doi.org10.4102/phcfm.v11i1.2094 [ Links ]
26. Masupe TK, Ndayi K, Tsolekile L, Delobelle P, Puoane T. Redefining diabetes and the concept of self-management from a patient's perspective: Implications for disease risk factor management. Health Educ Res 2018;33(1):40-54. https://doi.org10.1093/her/cyx077 [ Links ]
27. Stadler JT, Lackner S, Morkl S, et al. Obesity affects HDL metabolism, composition and subclass distribution. Biomedicines 2021;9(3):242. https://doi.org10.3390/biomedicines9030242 [ Links ]
28. Department of Health, South African Medical Research Council. South Africa Demographic and Health Survey 2016: Key Indicator Report. Pretoria: Statistics South Africa, 2017 [ Links ]
 Correspondence:
Correspondence:
N Peer
nasheeta.peer@mrc.ac.za
Accepted 12 December 2023


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}