










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSAMJ: South African Medical Journal
versão On-line ISSN 2078-5135
versão impressa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.114 no.1 Pretoria Jan. 2024
http://dx.doi.org/10.7196/SAMJ.2024.v114i1.16146
RESEARCH
Factors influencing in-hospital mortality for salvage percutaneous transjugular intrahepatic portosystemic shunting in cirrhotic patients with recalcitrant variceal bleeding after failed endoscopic intervention
J E J KrigeI; E G JonasII; M SetshediIII; S J BeningfieldIV; U K KotzeV; M M BernonVI; S BurmeisterVI; J C KloppersVII
IPRCS, PhD; Department of Surgery, Faculty of Health Sciences, University of Cape Town, and Surgical Gastroenterology, Hepatopancreatico-Biliary Unit, Groote Schuur Hospital, Cape Town, South Africa
IIMMed (Surg), PhD; Department of Surgery, Faculty of Health Sciences, University of Cape Town, and Surgical Gastroenterology, Hepatopancreatico-Biliary Unit, Groote Schuur Hospital, Cape Town, South Africa
IIIMB ChB, PhD; Department of Medicine, Faculty of Health Sciences, University of Cape Town and Groote Schuur Hospital, Cape Town, South Africa
IVMB ChB, FF Rad (D) SA; Department of Radiology, Faculty of Health Sciences, University of Cape Town and Groote Schuur Hospital, Cape Town, South Africa
VRN, BA Cur; Department of Surgery, Faculty of Health Sciences, University of Cape Town, and Surgical Gastroenterology, Hepatopancreatico-Biliary Unit, Groote Schuur Hospital, Cape Town, South Africa
VIMB ChB, FCS (SA); Department of Surgery, Faculty of Health Sciences, University of Cape Town, and Surgical Gastroenterology, Hepatopancreatico-Biliary Unit, Groote Schuur Hospital, Cape Town, South Africa
VIIFRCS (Edin), MMed (Surg); Department of Surgery, Faculty of Health Sciences, University of Cape Town, and Surgical Gastroenterology, Hepatopancreatico-Biliary Unit, Groote Schuur Hospital, Cape Town, South Africa
ABSTRACT
BACKGROUND: Endoscopic therapy is the first-line treatment of choice for control of acute variceal bleeding (AVB). In high-risk patients with persistent AVB despite pharmacological treatment and endoscopic intervention, percutaneous transjugular intrahepatic portosystemic shunting (TIPS) provides a minimally invasive salvage method to reduce portal pressure and control bleeding
OBJECTIVES: To evaluate factors influencing in-hospital mortality after salvage TIPS (sTIPS) in patients with exsanguinating variceal bleeding despite medical treatment and endoscopic intervention
METHODS: Clinical and laboratory data were analysed in all patients treated with sTIPS following failed endoscopic therapy for AVB between August 1991 and November 2020. Factors associated with and predictors of death were determined using bivariate analysis and univariate logistic regression analysis
RESULTS: Thirty-four patients (29 men, 5 women), mean age 52 years (range 31 - 80), received sTIPS for uncontrolled (n=11) or refractory (n=23) AVB. The causes of portal hypertension were alcohol-related (n=24) and non-alcohol-related cirrhosis. Salvage TIPS controlled bleeding in 32 patients, with recurrence in 1. Ten patients died in hospital (mean 4.8 days, range 1 - 10) of liver failure (n=4), multiorgan failure (n=3), alcoholic cardiomyopathy (n=2) and uncontrolled gastric variceal bleeding (n=1). On bivariate analysis, factors associated with death were Child-Pugh (C-P) score >10 (p=0.006), sodium Model for End-stage Liver Disease (MELD-Na) score >22 (p<0.001), > 8 units of blood transfused (p<0.001), Sengstaken-Blakemore balloon tube placement (p<0.001), endotracheal intubation (p<0.001), inotropic support (p<0.001) and endoscopically uncontrolled bleeding (p<0.001). Univariate logistic regression analysis showed that the most significant predictors of mortality were inotrope dependency (odds ratio (OR) 134; p<0.001), endotracheal intubation (OR 99; p<0.001), endoscopically uncontrolled bleeding (OR 28; p=0.001), grade 3 ascites (OR 20.9; p=0.012) and C-P grade C (OR 8.8; p=0.011
CONCLUSION: Salvage TIPS controlled variceal bleeding in 94% of patients after failed endoscopic therapy with 29% in-hospital mortality. The most significant predictors of mortality were C-P grade C, grade 3 ascites, inotrope requirement, endotracheal intubation and endoscopically uncontrolled bleeding
Acute variceal bleeding (AVB) is the most serious acute life-threatening complication of portal hypertension, especially in patients with hepatic decompensation.[1] Rapid and sustained control of bleeding is the immediate priority, but despite conventional treatment, including urgent fluid and blood resuscitation, vasoactive drugs, prophylactic antibiotics and endoscopic intervention, treatment fails in up to 10% of patients, who continue to bleed.[2] In this high-risk group, further immediate options include a second attempt at endoscopic intervention and balloon or stent tamponade to temporarily control variceal bleeding. In the past, patients in whom active bleeding persisted despite these treatments required surgical intervention with either a portocaval shunt or gastric devascularisation and oesophageal transection as a salvage operation, which had substantial implications in terms of morbidity and mortality.[3]
Technical advances in interventional radiology have led to the evolution and implementation of transjugular intrahepatic portosystemic shunting (TIPS) as a non-invasive salvage alternative to surgery in patients with uncontrolled variceal bleeding.[4] TIPS provides a percutaneous radiologically created shunt between portal and hepatic veins, which reduces portal vein pressure by diverting blood from the portal to the hepatic and systemic venous system through a low-resistance intrahepatic stent.[5] TIPS is now established as the preferred rescue or salvage procedure for patients who have either uncontrolled or severe recurrent variceal bleeding unresponsive to medical and endoscopic treatment.[6] This study investigated the outcome of salvage TIPS (sTIPS) in patients who had life-threatening variceal bleeding resistant to standard treatments, in order to identify clinical and laboratory risk factors predicting in-hospital death during the index admission.
Methods
The study was a retrospective cohort analysis of adult patients treated in the Surgical Gastroenterology Unit (SGU) at Groote Schuur Hospital and the University of Cape Town Academic Hospital who underwent sTIPS for life-threatening uncontrolled or severe refractory variceal bleeding between August 1991 and November 2020. The study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for reporting observational studies.[7]
Baseline demographic, clinical and endoscopic data and biochemical variables were collected on admission to the unit, and the anonymised and de-identified information was retrieved from a prospectively maintained faculty ethics-approved oesophageal variceal registry (Table 1). In addition, the causes of portal hypertension and infection with hepatitis B or hepatitis C were documented. The Model for End-stage Liver Disease (MELD) score, sodium MELD (MELD-Na) score, and Child-Pugh (C-P) score and grade (A, B or C) were calculated.
Details of the acute bleeding management protocol and the endoscopic interventional techniques used in our unit have been published previously[8-10] An inotrope infusion was used when necessary to maintain a mean arterial pressure >65 mmHg. Urgent diagnostic endoscopy was performed to identify the source of bleeding as soon as the patient was adequately resuscitated. If bleeding oesophageal varices were encountered, injection sclerotherapy (IST) or endoscopic variceal band ligation (EVL) was used.[9] In patients with uncontrollable bleeding, a Sengstaken-Blakemore balloon tube or an oesophageal stent was inserted for tamponade. Endotracheal intubation was used for airway protection when necessary, and further endoscopic procedures were performed within 24 hours.[10] In patients who had uncontrolled variceal bleeding or in those with persistent refractory bleeding despite endoscopic intervention, sTIPS was used as a rescue treatment.
TIPS was performed under general anaesthesia as soon as possible after the diagnosis of active uncontrolled variceal bleeding. Imaging was reviewed to exclude portal, splenic or hepatic vein thrombosis or vascular anomalies, and duplex Doppler ultrasound was repeated before the TIPS to confirm patency.[10] If large-volume ascites was present, pre-procedural paracentesis was performed. An expandable 10 mm uncovered metal Wallstent of variable length from 49 to 90 mm (Boston Scientific, USA) was placed to maintain patency of the radiologically created shunt between the portal and hepatic veins.[10]
Statistical analysis
The primary endpoint of the study was in-hospital mortality. Secondary endpoints were control of variceal bleeding after sTIPS and variceal rebleeding after initial control by sTIPS. The characteristics of the patients are presented as medians (range) or means (standard deviation (SD)), and as numbers (percentages) for categorical data. Fisher's exact test was used for comparing dichotomous variables, and the non-parametric Mann-Whitney rank-sum test for continuous variables. All tests were two-sided. The variables listed in Table 1 were considered as potential prognostic factors associated with mortality and were tested using bivariate analysis. These factors, when significantly correlated with the primary endpoint, were evaluated in a univariate logistic regression analysis to identify independent predictors of survival. A p-value <0.05 was considered statistically significant. Statistical analysis was performed using Stata software version 11 (StataCorp., USA).
Ethical considerations
The study protocol was approved by the Human Research Ethics Committee of the University of Cape Town (ref. no. 120/2019), and the research was conducted in accordance with the Declaration of Helsinki.
Results
A total of 564 patients with variceal bleeding were admitted to the SGU during the study period. In 530 patients (94%), bleeding was controlled by vasoactive medication and endoscopic intervention. In 34 patients (6%), bleeding was uncontrolled or persistent despite endoscopic intervention. These patients underwent urgent TIPS and constitute the study population. Eleven of the 34 patients had endoscopically uncontrolled variceal bleeding and 23 had severe recurrent and refractory bleeding after initial endoscopic control.
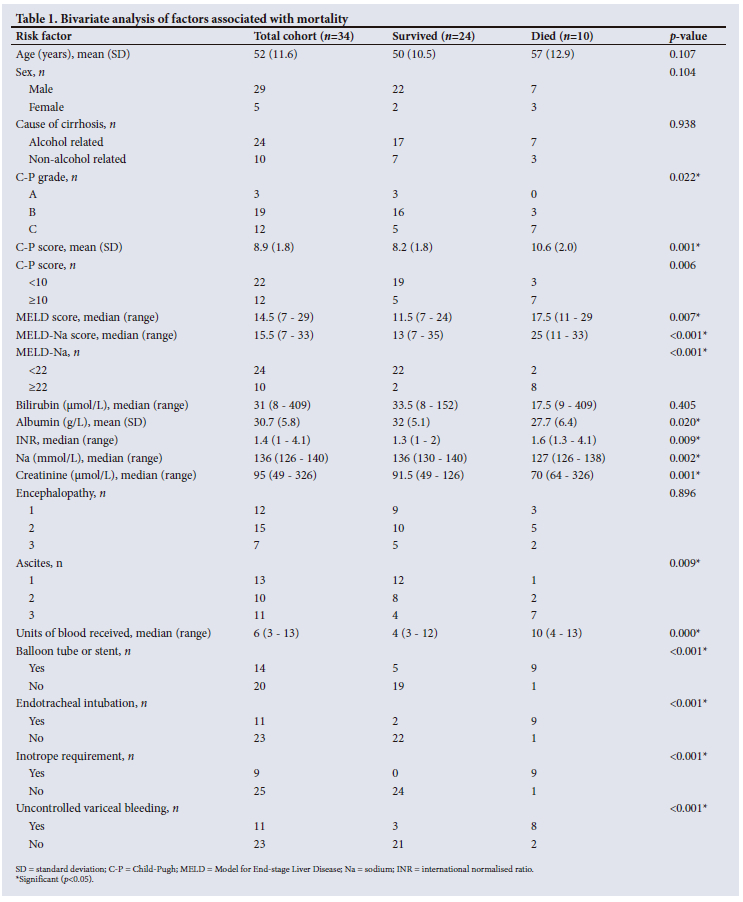
The demographic, clinical and endoscopic data and biochemical variables are summarised in Table 1. The mean age of the 29 men and 5 women was 52 (range 31 - 80) years. The causes of portal hypertension were alcohol (n=24), haemochromatosis (n=2), chronic hepatitis B infection (n=2), chronic hepatitis C infection (n=1), non-alcoholic steatohepatitis (n=2), and drug-induced (n=2) or sarcoid-related (n=1) cirrhosis. Before TIPS, 19 patients had a median of 3 (range 1 - 9) IST sessions, and 20 had a median of 2 (1 - 6) EVL sessions, with a median of 10 bands placed per session. Five patients had both IST and EVL. The median number of units of blood transfused before sTIPS was 6 (3 - 13), and 14 patients required either balloon tamponade (n=12) or placement of a Danis stent (n=2) to temporarily control bleeding. Eleven patients required endotracheal intubation and ventilation, and 9 required inotropic support.
The TIPS was placed successfully in all patients, and bleeding was controlled in 32 of the 34 (94%). Bleeding persisted in 2 patients (6%) despite a patent TIPS on repeat Doppler ultrasound. A further patient developed recurrent bleeding in hospital during the index admission after initial control of bleeding by TIPS. Overall control of bleeding by sTIPS was achieved in 31 of 34 patients (91%).
Ten patients (29%) died in hospital (mean 4.8 days, range 1 -10) of progressive liver failure (n=4), multiorgan failure (n=3), alcoholic cardiomyopathy (n=2) and uncontrolled gastric variceal bleeding (n=1). Mortality in C-P grade A was 0%, in C-P grade B 16% and in C-P grade C 58%. In the patients who died, the mean (SD) C-P score was 10.6 (2.0), the median MELD score 18 (range 11 - 29) and the median MELD-Na score 25 (11 - 33) (Table 1). Nine (75%) of the 12 patients who required balloon tamponade died, while all 9 (100%) who required inotropic support died. Analysis of the two subcategories shows that 8 of 11 patients (73%) who had endoscopically uncontrolled variceal bleeding and required a transfusion of >8 units of blood during the index hospital admission died, while 2 of 23 patients (9%) who had refractory variceal bleeding died.
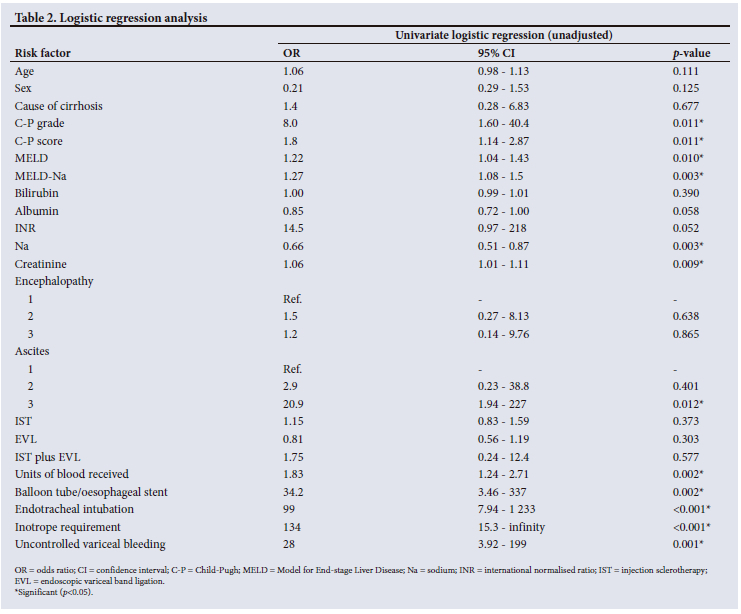
On bivariate analysis, factors associated with death after sTIPS were C-P score >10 (p=0.006), MELD-Na >22 (p<0.001), >8 units of blood transfused (p<0.001), Sengstaken tube placement (p<0.001), endotracheal intubation (p<0.001), inotropic support (p<0.001) and endoscopically uncontrolled bleeding (p<0.001) (Table 1). In an unadjusted univariate logistic regression model, the significant predictors of mortality were need for inotropic support (odds ratio (OR) 134; p<0.001), endotracheal intubation (OR 99; p<0.001), endoscopically uncontrolled bleeding (OR 28; p=0.001), grade 3 ascites (OR 20.9; p=0.012) and C-P grade C (OR 8.8; p=0.011) (Table 2).
Discussion
The common characteristics in this high-risk cohort were uncontrolled or refractory variceal bleeding in the presence of portal hypertension and liver decompensation, active variceal bleeding at the time of endoscopy, and failure of standard medical and endoscopic intervention to control bleeding. The patients required urgent sTIPS placement as a life-saving procedure. A TIPS was inserted successfully in all patients, and overall control of bleeding was achieved in 91% of patients after sTIPS with 71% in-hospital survival. Mortality correlated with C-P grade and was 16% in grade B and 58% in grade C. Factors associated with death on bivariate analysis were C-P score >10, MELD-Na >22, >8 units of blood transfused, Sengstaken tube placement, endotracheal intubation, inotropic support and endoscopically uncontrolled bleeding. The most significant predictors of mortality in an unadjusted univariate logistic regression model were the need for inotropic support, endotracheal intubation, endoscopically uncontrolled bleeding, grade 3 ascites and C-P grade C.
The prognosis of cirrhotic patients in general and after sTIPS in particular depends on residual liver function, the magnitude and duration of the deleterious hepatic and renal consequences of persistent variceal bleeding, the presence of significant comorbidities, and the rapidity and efficacy with which emergency treatment is initiated.[1,11] The mortality rate in our study population should be interpreted in the context of the poor baseline liver function; 56% of the patients were C-P grade B and 35% C-P grade C, and overall median C-P and MELD scores were 9 and 15, respectively. Other studies reporting rescue sTIPS for acute oesophageal variceal bleeding have shown mortality rates ranging from 15% to 75%, which is significantly higher than in patients undergoing elective TIPS.[12-15] Helton et al.[l6] reported a 56% in-hospital mortality rate for patients who were actively bleeding or haemodynamically unstable at the time of the TIPS.
The reported mortality associated with TIPS placement varies widely with differing inclusion criteria, timing of TIPS, and the severity of underlying liver disease. Some reports combine the results of patients actively bleeding during TIPS with those of patients who were stable during the procedure. Patient factors that have been reported to lead to increased mortality after TIPS placement include failure to control bleeding,[17] C-P stage C,[17-21] MELD score >30,[21,22] Acute Physiology and Chronic Health Evaluation (APACHE II) score >20,[12,20] haemodynamic instability at the time of the TIPS procedure,[23] use of inotropes,[12,18,23,24] mechanical ventilation,[18] balloon tamponade,[23] the presence of comorbidities, sepsis,[17,23,24] emergency TIPS, hyperbilirubinaemia,[12,25,26] lactate >12 mmol/L,[22] hyponatraemia[24] and renal failure.[12,17,18,27,28] Most deaths after emergency TIPS are the consequence of hepatic or multiorgan failure and sepsis,[29] and only a minority are due to recurrent variceal bleeding.
The results of this study have important implications for patients with major variceal bleeding that cannot be controlled endoscopically. We found a significant correlation between early mortality after TIPS and the need for endotracheal intubation, balloon tamponade and inotropic support. It is evident from several studies that as multiple unsuccessful endoscopic attempts are made to stop the bleeding, liver function deteriorates, complications supervene, and outcome worsens. Patients with major variceal bleeding are best managed in a tertiary referral unit with a skilled multidisciplinary team. Patients in whom endoscopic intervention fails to control bleeding should be identified early so that sTIPS can be performed before the deleterious consequences of deteriorating liver function and multiorgan failure occur. Other studies have identified the futility of sTIPS in patients with a C-P score >13, MELD score >30 and lactate level >12 mmol/L.[12,30]
The data documented must be interpreted in the light of limitations that include the long duration of the study and the relatively small number of patients, all of whom had uncovered metal stents, which now have been replaced by covered stents. In addition, there may be selection bias, as the unit functions as a tertiary referral centre for high-risk patients. A major strength of the study is the analysis of real-world data from an unselected cohort of patients consecutively treated by the same team using specific endpoints.
Conclusion
This study shows that although sTIPS controlled variceal bleeding in 94% of patients after failed endoscopic intervention, mortality remained high with 29% in-hospital deaths, especially in patients with uncontrolled bleeding. The most significant predictors of mortality were C-P grade C, grade 3 ascites, inotrope requirement, endotracheal intubation and endoscopically uncontrolled bleeding. Further effort is needed to reduce the high mortality and morbidity despite successful sTIPS placement. In order to achieve this goal, early identification of patients unresponsive to medical treatment is crucial so that urgent sTIPS for portal decompression can be initiated without delay.
Declaration. None.
Acknowledgements. None.
Author contributions. Conception and design of the work: JEJK, EGJ, MMB; acquisition, analysis and interpretation of data: JEJK, EGJ, UKK, MS, MMB; drafting the work: JEJK, EGJ, SJB, MMB; critical revision: JEJK, EGJ, SJB, MMB, UKK, MS, SB, CJK; final approval of the version to be published: all authors.
Funding. None.
Conflicts of interest. None.
References
1. Garcia-Tsao G, Abraldes JG, Berzigotti A, Bosch J. Portal hypertensive bleeding in cirrhosis: Risk stratification, diagnosis, and management: 2016 practice guidance by the American Association for the study of liver diseases. Hepatology 2017;65(1):310-335. https://doi.org/10.1002/hep.28906 [ Links ]
2. Tripathi D, Stanley AJ, Hayes PC, et al.; Clinical Services and Standards Committee of the British Society of Gastroenterology. U.K. guidelines on the management of variceal haemorrhage in cirrhotic patients. Gut 2015;64(11):1680-1704. https://doi.org/10.1136/gutjnl-2015-309262 [ Links ]
3. De Franchis R; Baveno VI Faculty. Expanding consensus in portal hypertension: Report of the Baveno VI Consensus Workshop: Stratifying risk and individualizing care for portal hypertension. J Hepatol 2015;63(3):743-752. https://doi.org/10.1016/j.jhep.2015.05.022 [ Links ]
4. Deltenre P, Trépo E, Rudler M, et al. Early transjugular intrahepatic portosystemic shunt in cirrhotic patients with acute variceal bleeding: A systematic review and meta-analysis of controlled trials. Eur J Gastroenterol Hepatol 2015;27(9):e1-9. https://doi.org/10.1097/MEG.0000000000000403 [ Links ]
5. Manning C, Elzubeir A, Alam S. The role of pre-emptive transjugular intrahepatic portosystemic shunt in acute variceal bleeding: A literature review. Ther Adv Chronic Dis 2021;12:2040622321995771. https://doi.org/10.1177/2040622321995771 [ Links ]
6. Loffroy R, Estivalet L, Cherblanc V, et al Transjugular intrahepatic portosystemic shunt for the management of acute variceal hemorrhage. World J Gastroenterol 2013;19(37):6131-6143. https://doi.org/10.3748/wjg.v19.i37.6131 [ Links ]
7. Von Elm E, Altman DG, Egger M, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet 2007;370(9596):1453-1457. https://doi.org/10.1016/S0140-6736(07)61602-X [ Links ]
8. Krige JE, Kotze UK, Bornman PC, Shaw JM, Klipin M. Variceal recurrence, rebleeding and survival after endoscopic injection sclerotherapy in 287 alcoholic cirrhotic patients with bleeding esophageal varices. Ann Surg 2006;244(5):764-770. https://doi.org/10.1097/01.sla.0000231704.45005.4e [ Links ]
9. Krige JEJ, Bornman PC. Endoscopic therapy in the management of esophageal varices: Injection sclerotherapy and variceal ligation. In: Blumgart L, ed. Surgery of the Liver, Biliary Tract and Pancreas. 4th ed. Philadelphia: Saunders, Elsevier, 2007:1579-1593. [ Links ]
10. Krige JEJ, Beningfield SJ. Endoscopic therapy in the management of esophageal varices. In: Fischer J, ed. Mastery of Surgery. 7th ed. Philadelphia: Lippincott Williams & Wilkins, 2019:1384-1398. [ Links ]
11. Tripathi D, Stanley AJ, Hayes PC, et al. Transjugular intrahepatic portosystemic stent-shunt in the management of portal hypertension. Gut 2020;69(7):1173-1192. https://doi.org/10.1136/gutjnl-2019-320221 [ Links ]
12. Horhat A, Bureau C, Thabut D, Rudler M. Transjugular intrahepatic portosystemic shunt in patients with cirrhosis: Indications and posttransjugular intrahepatic portosystemic shunt complications in 2020. United European Gastroenterol J 2021;9(2):203-208. https://doi.org/10.1177/2050640620952637 [ Links ]
13. Banares R, Casado M, Rodríguez-Láiz JM, et al. Urgent transjugular intrahepatic portosystemic shunt for control of acute variceal bleeding. Am J Gastroenterol 1998;93(1):75-79. https://doi.org/10.1111/j.1572-0241.1998.075_c.x [ Links ]
14. Le Moine O, Devière J, Ghysels M, et al. Transjugular intrahepatic portosystemic stent shunt as a rescue treatment after sclerotherapy failure in variceal bleeding. Scand J Gastroenterol Suppl 1994;207:23-28. https://doi.org/10.3109/00365529409104190 [ Links ]
15. Vangeli M, Patch D, Burroughs AK. Salvage TIPS for uncontrolled variceal bleeding. J Hepatol 2002;37(5):703-704. https://doi.org/10.1016/s0168-8278(02)00321-5 [ Links ]
16. Helton WS, Belshaw A, Althaus S, Park S, Coldwell D, Johansen K. Critical appraisal of the angiographic portacaval shunt (TIPS). Am J Surg 1993;165(5):566-571. https://doi.org/10.1016/s0002-9610(05)80436-2 [ Links ]
17. Bouzbib C, Cluzel P, Sultanik P, et al. Prognosis of patients undergoing salvage TIPS is still poor in the preemptive TIPS era. Clin Res Hepatol Gastroenterol 2021;45(6):101593. https://doi.org/10.1016/j.clinre.2020.101593 [ Links ]
18. Tzeng W-S, Wu R-H, Lin C-Y, et al. Prediction of mortality after emergent transjugular intrahepatic portosystemic shunt placement: Use of APACHE II, Child-Pugh and MELD scores in Asian patients with refractory variceal hemorrhage. Korean J Radiol 2009;10(5):481-489. https://doi.org/10.3348/kjr.2009.10.5.481 [ Links ]
19. Heinzow HS, Lenz P, Köhler M, et al. Clinical outcome and predictors of survival after TIPS insertion in patients with liver cirrhosis. World J Gastroenterol 2012;18(37):5211-5218. https://doi.org/10.3748/wjg.v18.i37.5211 [ Links ]
20. Rubin RA, Haskal ZJ, O'Brien CB, Cope C, Brass CA. Transjugular intrahepatic portosystemic shunting: Decreased survival for patients with high APACHE II scores. Am J Gastroenterol 1995;90(4):556-563. [ Links ]
21. Maimone S, Saffioti F, Filomia R, et al Predictors of rebleeding and mortality among patients with refractory variceal bleeding undergoing salvage transjugular intrahepatic portosystemic shunt (TIPS). Dig Dis Sci 2019;64(5):1335-1345. https://doi.org/10.1007/s10620-018-5412-x [ Links ]
22. Walter A, Rudler M, Olivas P, et al; Salvage TIPS Group. Combination ofmodel for end-stage liver disease and lactate predicts death in patients treated with salvage transjugular intrahepatic portosystemic shunt for refractory variceal bleeding. Hepatology 2021;74(4):2085-2101. https://doi.org10.1002/hep.31913 [ Links ]
23. Azoulay D, Castaing D, Majno P, et al. Salvage transjugular intrahepatic portosystemic shunt for uncontrolled variceal bleeding in patients with decompensated cirrhosis. J Hepatol 2001;35(5):590-597. https://doi.org/10.1016/s0168-8278(01)00185-4 [ Links ]
24. Jalan R, John TG, Redhead DN, et al. A comparative study of emergency transjugular intrahepatic portosystemic stent-shunt and esophageal transection in the management of uncontrolled variceal hemorrhage. Am J Gastroenterol 1995;90(11):1932-1937. [ Links ]
25. Chalasani N, Clark WS, Martin LG, et al. Determinants of mortality in patients with advanced cirrhosis after transjugular intrahepatic portosystemic shunting. Gastroenterology 2000;118(1):138-144. https://doi.org/10.1016/s0016-5085(00)70422-7 [ Links ]
26. Rajan DK, Haskal ZJ, Clark TW. Serum bilirubin and early mortality after transjugular intrahepatic portosystemic shunts: Results of a multivariate analysis. J Vasc Interv Radiol 2002;13(2 Pt 1):155-161. https://doi.org/10.1016/s1051-0443(07)61932-0 [ Links ]
27. Malinchoc M, Kamath PS, Gordon FD, Peine CJ, Rank J, ter Borg PC. A model to predict poor survival in patients undergoing transjugular intrahepatic portosystemic shunts. Hepatology 2000;31(4):864-871. https://doi.org/10.1053/he.2000.5852 [ Links ]
28. Brensing KA, Raab P, Textor J, et al. Prospective evaluation of a clinical score for 60-day mortality after transjugular intrahepatic portosystemic stent-shunt: Bonn TIPSS early mortality analysis. Eur J Gastroenterol Hepatol 2002;14(7):723-731. https://doi.org/10.1097/00042737-200207000-00003 [ Links ]
29. Patch D, Nikolopoulou V, McCormick A, et al. Factors related to early mortality after transjugular intrahepatic portosystemic shunt for failed endoscopic therapy in acute variceal bleeding. J Hepatol 1998;28(3):454-460. https://doi.org/10.1016/s0168-8278(98)80320-6 [ Links ]
30. Rajesh S, George T, Philips CA, et al. Transjugular intrahepatic portosystemic shunt in cirrhosis: An exhaustive critical update. World J Gastroenterol 2020;26(37):5561-5596. https://doi.org/10.3748/wjg.v26.i37.5561 [ Links ]
 Correspondence:
Correspondence:
J E J Krige
jej.krige@uct.ac.za
Accepted 8 November 2023


{kind=link}
{kind=link}