










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.114 n.1 Pretoria Jan. 2024
http://dx.doi.org/10.7196/samj.2023.v114i1.1098
RESEARCH
The characteristics of dermatology inpatients seen at the quaternary Inkosi Albert Luthuli Central Hospital in Durban, South Africa, over a 5-year period - 2015 – 2020
L MthembuI; J T MasukaII; K DuzeIII; A MosamIV
IMB ChB; Department of Dermatology, School of Clinical Medicine, College of Health Sciences, Nelson R Mandela School of Medicine, University of KwaZulu-Natal, Durban, South Africa
IIMFPM (UK), FC Derm (SA); Department of Dermatology, School of Clinical Medicine, College of Health Sciences, Nelson R Mandela School of Medicine, University of KwaZulu-Natal, Durban, South Africa
IIIMB ChB, FC Derm (SA); Department of Dermatology, School of Clinical Medicine, College of Health Sciences, Nelson R Mandela School of Medicine, University of KwaZulu-Natal, Durban, South Africa
IVFC Derm (SA), PhD; Department of Dermatology, School of Clinical Medicine, College of Health Sciences, Nelson R Mandela School of Medicine, University of KwaZulu-Natal, Durban, South Africa
ABSTRACT
BACKGROUND: In recent years, dermatology has been offered as an outpatient service, with decreasing inpatient dermatology admissions. However, dermatology consultation services have remained active, offering care to patients admitted for non-cutaneous indications by other specialties
OBJECTIVES: To describe the clinical spectrum and characteristics of inpatient dermatology diseases managed at a quaternary South African (SA) hospital
METHODS: We retrospectively reviewed and analysed electronic records of all dermatology inpatients managed by dermatologists from 2015 to 2020 at Inkosi Albert Luthuli Central Hospital (IALCH) in Durban, South Africa. Demographic and clinical data on the International Classification of Diseases (ICD) 10 dermatology diagnosis and admitting specialty were collected and analysed
RESULTS: A total of 4 867 patients were managed by the IALCH dermatology service during the study period. Females accounted for 2 527 (51.9%), while black African, coloured, Indian/Asian, white and unclassified patients constituted 3 146 (64.6%), 106 (2.2%), 1 129 (23.2%), 431 (8.9%) and 55 (1.1%), respectively. The median (interquartile range) age of the study population was 42.0 (28.0 - 58.0) years. Of 867 patients, 183 (3.8%) were dermatology inpatient admissions, whereas the remainder, 4 684 (96.2%), were seen as consults from other specialties. Most (1 010 (20.7%)) of the dermatology consults were received from plastic and reconstructive surgeons, while bacterial infections, decubitus ulcers and lower limb ulcers were the three most common referred diagnoses overall
CONCLUSION: A broad range of diagnoses is managed through the dermatology inpatient service, particularly as consultations. These services remain essential in the holistic management of patients
Dermatology is an outpatient-centred specialty frequently dealing with non-acute medical conditions.[1] However, dermatologists admit and manage patients who are severely ill and/or have complicated cutaneous diseases.[2] The reasons for dermatology inpatient admission can range from the severity of the disease and comorbid diseases to lack of transport and psychosocial support.[3,4] However, dermatology inpatient services are not only required by primarily dermatology-admitted inpatients, as inpatients in other disciplines also benefit from dermatology consultation services.[5] Dermatology input on the consultation service improves the early and correct diagnosis and appropriate management of cutaneous issues in addition to minimising unnecessary investigations.[5,6]
Previous studies indicate that demographic and clinical indications for inpatient dermatology management differ between study settings and the period of study.[7] In South Africa (SA), a younger population is admitted compared with developed countries such as Australia and the UK.[2,4,8] Furthermore, in Australia, dermatitis or eczema and ulcers were the most frequent indications for admission,[2] whereas in India, immunobullous disorders, connective tissue diseases and infections accounted for the majority of admissions.[1,9] In Spain, surgery was the most common indication for dermatological admissions.[7] In contrast, atopic dermatitis, extensive psoriasis and severe drug reactions accounted for the majority of dermatology admissions in Cape Town, the largest metropolitan area in the Western Cape Province of SA.[4] A slightly different admission profile was observed in Durban, KwaZulu-Natal Province, where drug-induced Steven Johnson syndrome, dermatitis and seborrhoeic dermatitis were among the most common indications for admission.[8] No study on dermatology inpatient consultations has been done in SA. However, it can be expected that different specialties and cutaneous conditions might be observed, as has previously been shown in other settings.
Currently, there is a dearth of information on the characteristics of patients managed by dermatologists in the hospital inpatient service in SA, particularly in KwaZulu-Natal.[9] In this study we set out to describe the clinical spectrum of inpatient dermatology diseases managed at a quaternary SA hospital. We also aimed to describe the age, gender and outcomes of dermatology admissions. In addition, we also characterise the patients managed in the dermatology consultation service. This is important for health services planning and infrastructure provision.[2]
Methods
Study design and setting
We carried out a single-institution, retrospective chart review of all hospital inpatients treated by dermatologists from 2015 to 2020 at Inkosi Albert Luthuli Central Hospital (IALCH) in Durban, KwaZulu-Natal, SA. This is a quaternary referral and teaching hospital. It caters for referrals from the tertiary and other hospitals in the province providing specialist and subspecialist service under four main domains/disciplines, namely surgery, medicine, mother-and-child care and the perioperative services.[10] We included any patient who had at least one admission during the study period meeting one of the following criteria: inpatient admission, or discharge department was dermatology and/or had an inpatient stay with a dermatology International Classification of Diseases (ICD) code, and/or inpatient stay included occupancy of a bed in dermatology with a dermatology ICD code, capturing dermatology inpatients and consultations. All dermatology diagnoses were taken at the ICD hierarchy level 3.
Statistical analysis
Convenience sampling was done for the current study. A data analyst from the IALCH information technology department assisted in extracting the required demographic and clinical data from MEDITECH 6.15 electronic medical records system into an Excel sheet (Microsoft Corp., USA). The following demographic data were collected: patient age, gender, race, referring clinical facility and patient's payer type. Clinical data on the ICD 10 dermatology diagnosis at the hierarchy level 3 for the chosen admission and the associated admitting specialty and/or discipline were also collected. The data were then analysed using the Statistical Package for Social Sciences (SPSS) version 22.0 (IBM Corp., USA). Descriptive statistics such as frequencies and percentages were used to summarise categorical variables, while continuous variables were described using either means and standard deviations or medians and the interquartile range (IQRs), as appropriate. Comparisons of count data were done using the χ2 or Fisher's exact tests as appropriate, whereas comparisons of continuous data were done using the independent Student t-test. All analyses were done at the 0.05 significance level.
Ethical considerations
The study was approved by the IALCH ethics committee and the University of KwaZulu-Natal's Biomedical Research Institutional Review Board (ref. no. BREC/00004454/2022). All patient information was de-identified and patient confidentiality was maintained by using unique study patient identification numbers. No informed consent was obtained from participants as this is a database study.
Results
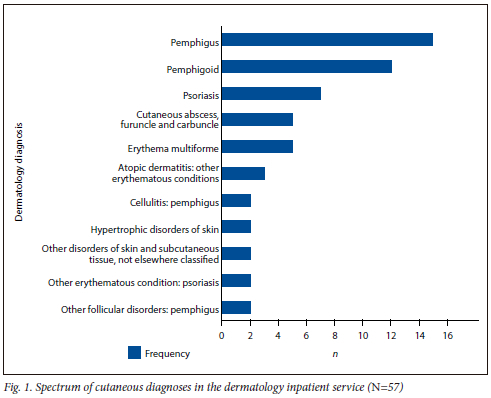
A total of 4 867 patients were managed by the dermatology service during the study period. Of these, 183 (3.8%) were dermatology inpatient admissions whereas the remainder, 4 684 (96.2%), were seen as consults from other specialties. The trends of dermatology inpatient admissions over the study period are shown in Fig 1. The median (IQR) age of the study population was 42.0 (28.0 - 58.0) years. Females accounted for 2 527 (51.9%), while black African, coloured, Indian/Asian, white and unclassified patients constituted 3 146 (64.6%), 106 (2.2%), 1 129 (23.2%), 431 (8.9%) and 55 (1.1%), respectively.
Characteristics of dermatology inpatient admissions
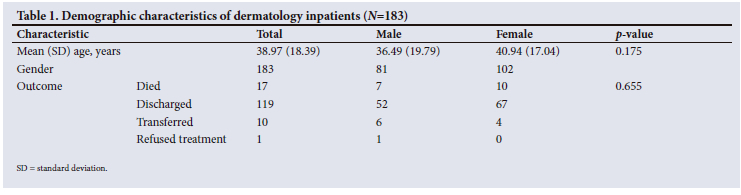
The median (IQR) age of the dermatology inpatients was 37 (23.00 -52.00) years. The median (IQR) number of admissions for the dermatology inpatients was 1.00 (0; 18.00). Most of the admitted patients were females (Table 1). Bullous diseases - pemphigus and pemphigoid -were the most common dermatological diagnoses in those admitted. The spectrum of dermatological conditions managed on the inpatient service is shown in Fig 1.
Characteristics of dermatology consultation service
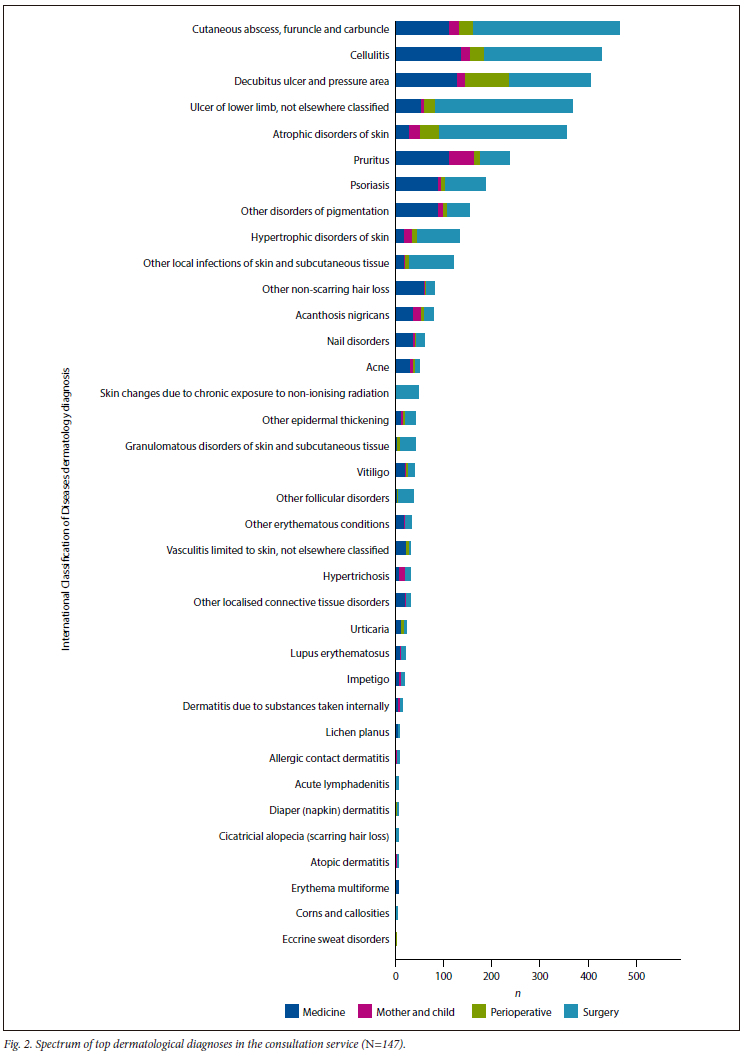
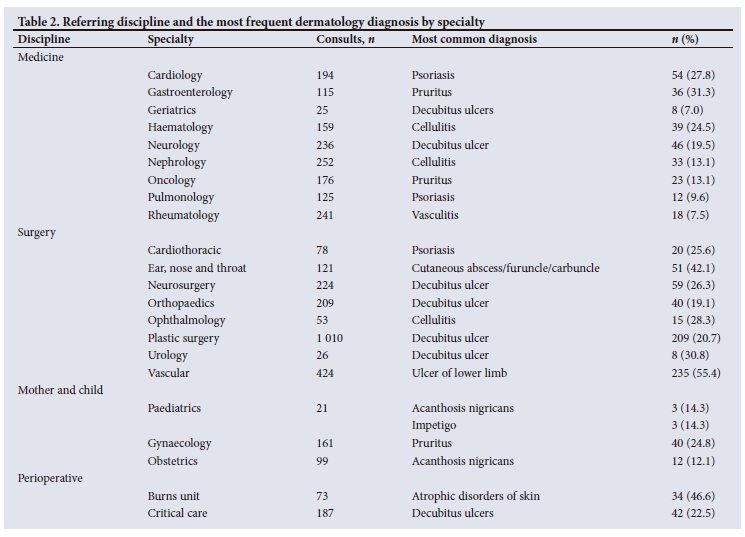
Dermatological consultations were received from a wide range of disciplines, as indicated in Fig. 2. The median (IQR) age of the patients in the consult service was 42.0 (29.0 - 58.0) years, and there was a slight female preponderance at 2 425 (51.8%). Females also predominated in the medical (58.2%) and mother-and-child (97.2%) disciplines, whereas males predominated in the perioperative (34.8%) and surgical (44.7%) disciplines. The most common conditions necessitating consults to dermatology were the cutaneous abscess, furuncle and carbuncles grouping of diagnoses (464 (10.8%)), followed by cellulitis (426 (9.09%)) and decubitus ulcers (403 (8.60%)). The remainder constituted other ICD dermatology diagnoses and/or combinations thereof (Fig. 2). Most of the consults were observed from the surgical discipline, accounting for 2 430 (51.9%), followed by medicine (1 616 (34.6%)), the perioperative discipline (356 (7.6%)) and finally the mother-and-child discipline (282 (6.0%)). The most frequently requesting specialties were plastic surgery (1 010 (21.6%)), nephrology (252 (5.4%)) and rheumatology (241 (5.1%)) (Table 2). Consults were seldom requested from paediatric surgical subspecialties.
Discussion
In this study we describe the clinical spectrum and characteristics of inpatient dermatology diseases managed at a quaternary SA hospital. As expected, >90% of all dermatology inpatient services are offered in the consultation service, with only 3.8% being managed as dermatology inpatients.[11] The median (IQR) age of the study population was 42.0 (28.0 - 58.0) years. Dermatology-admitted inpatients were younger than patients managed in the consultation service, with median ages of 37 years and 42 years, respectively. Females predominated in both the dermatology-admitted inpatient and the consultation services, with 55.7% and 51.8%, respectively. Moreover, females predominated within the medical and mother-and-child disciplines, in contrast with the perioperative and surgical disciplines, where males predominated. Differences were noted for the most prevalent diseases managed within both populations. The top three dermatology diagnoses managed in the inpatient service were pemphigus, bullous pemphigoid and psoriasis, while bacterial infections - abscesses, furuncles, carbuncles, cellulitis and decubitus ulcers - predominated in the consultation service.
In recent years, there has been a paradigm shift toward greater provision of dermatology services in outpatient settings,[12] possibly owing to the advent of effective outpatient treatments and as a cost-reduction measure.[13,14] However, inpatient dermatology services are essential for the correct diagnosis and management of often unattended, previously existing cutaneous conditions seen in patients admitted for other reasons.[12] Within our hospital, consultations from other departments predominate the inpatient workload for our dermatologists, as observed in other countries.[11] Unlike in other studies,[15,16] the discipline of surgery, mostly through the plastic and reconstructive department, had the greatest need for the dermatology consultation service. This may be explained by common diseases encountered or managed by dermatology and plastic surgery, such as cutaneous malignancies and keloids. The less surgically demanding lesions tend to be referred to dermatology, and vice versa, at our facility. Unlike in other studies,[13,14,16] general internal medicine and general surgery were not the main referring disciplines, as these specialties are not present at our facility.
The order of consultations from other specialties was largely similar to that found in other studies, especially for internal medicine subspecialties. Consultations from neurology, nephrology and rheumatology featured prominently for internal medicine consultations, as in other studies.[16] Similar to findings by Storan et al.,[15] the most common cutaneous diseases seen by the hospital dermatology consulting service were skin infections. However, this was noted mostly with surgical specialties. Likewise, it is not surprising that decubitus ulcers dominated for patients referred by geriatrics, neurology, neurosurgery and orthopaedics. Interestingly, psoriasis was the main diagnosis referred to dermatology by cardiology and cardiac surgery departments, possibly indicating the link to metabolic syndrome, especially for the former. The median age of 42 years of patients in the dermatology consultation service is much older than the 32 years observed in a similar study in India.[16] As in other studies, there were more consultations for females than males.[13,14]
The most common cause of admission in our dermatology wards was severe, uncontrolled immunobullous disorders, both the pemphigus and pemphigoid groups of diseases. These findings are similar to those reported in Indian hospitals,[1,9] but they differ from those from Australia and Brazil, where eczema/ dermatitis predominated dermatology admissions.[2,17] These findings also differ from results from Spain, which indicate neoplasms as the main cause of admission, possibly due to the increased focus on dermatological surgery in their service.[7] Furthermore, unlike findings in India and Brazil, we had few infective indications for admission by the dermatology team. Likewise, our current findings also differ from previous observations in our setting, where cutaneous adverse drug reactions such as Stevens-Johnson syndrome and toxic epidermal necrolysis predominated the dermatology admissions during a period when our antiretroviral regimens consisted of non-nucleoside reverse transcriptase inhibitor drugs such as nevirapine and efavirenz.[8] This shows that admission trends may vary depending on other conditions being managed and/ or prevalent in the community at the time. Unlike the findings of Sen et al[1] in India, where the median age of the dermatology admitted inpatients was in the fifth decade, we found a younger inpatient population in our study. In the same study by Sen et al.,[1] males outnumbered females, demonstrating that patient characteristics and dermatology services are different in different countries.[7]
The major strength of this study is the large sample size, taken over 5 years, which gives a broader reflection of the contribution of inpatient dermatology services within a quaternary teaching hospital. We have demonstrated the dermatology consultation services offered to other departments, and the need to recognise the requirement for these services within any hospital set-up.[14] Furthermore, we delineated the diseases warranting dermatology admission and necessitating dermatology consultations from other disciplines. These findings should assist health planners by providing evidence of the utility of dermatology, not only to primarily dermatology-admitted patients, but to other specialties for the provision of holistic care to patients. The continuing downsizing of dermatology services and residency programmes in several hospitals[18,19] shows an underappreciation of the impact of the specialty, especially from the dermatology consultation service offered to other specialties. However, the principal limitation of the current study is its retrospective nature, which causes information bias.
Conclusion
Even though dermatology is mostly considered an outpatient service, many inpatients benefit from dermatology services, especially through its consultation service. Most consultations were received from plastic and reconstructive surgeons, while bacterial infections, decubitus ulcers and lower limb ulcers were the three most common referred diagnoses overall. Dermatology consultations should be promoted as they reduce hospitalisation costs and improve outcomes in patients with concomitant skin diseases admitted by other specialties.[20] This is especially so for patients with cutaneous manifestations of internal diseases not otherwise easily diagnosed by other specialties.[14] This also offers an opportunity to educate and improve dermatology diagnosis for primary referring specialties.[14] This is especially important given that the burden of cutaneous diseases in the hospital is great, and the expertise regarding the recognition and management of these disorders is limited outside the specialty.[21]
Declaration. This study project was led by LM and done in partial fulfilment for her MMed Dermatology degree at the University of KwaZulu-Natal under the main supervision of AM.
Acknowledgements. The authors are grateful for the assistance provided by the IALCH nurses and clerks in conducting this study.
Author contributions. LM and JM conceptualised, designed and collected the data for the study. JM performed statistical analyses. Both LM and JM drafted the manuscript with AM and KD revising the manuscript for clinical validity. All authors read and approved the final version of the manuscript.
Funding. None.
Conflicts of interest. None.
References
1. Sen A, Chowdhury S, Poddar I, Bandyopadhyay D. Inpatient dermatology: Characteristics of patients and admissions in a tertiary level hospital in eastern India. Indian J Dermatol 2016;61(5):561-564. https://doi.org/10.4103%2F0019-5154.190104 [ Links ]
2. Bale J, Chee P. Inpatient dermatology: Pattern of admissions and patients' characteristics in an Australian hospital. Australas J Dermatol 2013;55(3):191-195. https://doi.org/10.1111/ajd.12097 [ Links ]
3. Helbling I, Muston HL, Ferguson JE, McKenna M. Audit of admissions to dermatology beds in Greater Manchester. Clin Exp Dermatol 2002;27(6):519-522. https://doi.org/10.1046/j.1365-2230.2002.01073.x [ Links ]
4. Jessop S, McKenzie R, Milne J, Rapp S, Sobey G. Pattern of admissions to a tertiary dermatology unit in South Africa. Int J Dermatol 2002;41(9):568-570. https://doi.org/10.1046/j.1365-4362.2002.01586.x [ Links ]
5. Joseph J, Truong K, Smith A, Fernandez-Penas P. Dermatology inpatient consultations in a tertiary hospital-a retrospective analysis. Int J Dermatol 2022;61(1):48-53. https://doi.org/10.1111/ijd.15724 [ Links ]
6. Alani A, Sadlier M, Uddin A, Hackett C, Ramsay B, Ahmad K. An analysis of inpatient dermatologic consultations at University Hospital Limerick: Inadequate infrastructure leads to acute skin failure. Ir J Med Sci 2017;186(2):305-307. https://doi.org/10.1007/s11845-016-1424-8 [ Links ]
7. García-Doval I, Feal C, Rosón E, et al. Inpatient dermatology: Characteristics of patients and admissions in a Spanish hospital. J Eur Acad Dermatol Venereol 2002;16(4):334-338. https://doi.org/10.1046/j.1468-3083.2002.00473.x [ Links ]
8. Mazibuko MN. The clinical spectrum and outcome of skin conditions in patients admitted to dermatology wards at King Edward VIII Hospital, Durban. Master's thesis. Durban: University of KwaZulu-Natal, 2016. [ Links ]
9. Gupta V, Gupta S, Kharghoria G, Pathak M, Sharma VK. Profile of dermatology inpatients and admissions over a four year period in a tertiary level government teaching hospital in North India. Indian J Dermatol Venereol Leprol 2022;88(3):342-348. https://doi.org/10.25259/IJDVL_711_20 [ Links ]
10. Inkosi Albert Luthuli Central Hospital. Hospital services. Durban: IALCH, 2022. https://www.ialch.co.za/services/ (accessed 28 December 2022). [ Links ]
11. Cuenca-Barrales C dV-MM, Descalzo-Gallego M, García-Doval I. Inpatient dermatology: Where are we headed? A nationwide population-based study of Spain from 2006 to 2016. J Deutsch Dermatol Ges 2021;19:707-717. https://doi.org/10.1111/ddg.14336 [ Links ]
12. Strowd LC. Inpatient dermatology: A paradigm shift in the management of skin disease in the hospital. Br J Dermatol 219;18(5):966-967. https://doi.org/10.1111/bjd.17778 [ Links ]
13. Mancusi S, Neto Cf. Inpatient dermatological consultations in a university hospital. Clinics 2010;65(9):851-855. https://doi.org/10.1590/S1807-59322010000900007 [ Links ]
14. Sherban A, Keller M. The role of inpatient dermatology consultations. Cutis 2021;108(4):193-196. https://doi.org/10.12788/cutis.0361 [ Links ]
15. Storan ER, Wetter DA, El-Azhary RA, Camilleri MJ, Bridges AG, Davis MD. Experience of a year of adult hospital dermatology consultations. Int J Dermatol 215;54(1):1150-1156. https://doi.org/10.1111/ijd.12555 [ Links ]
16. Vinay K, Thakur V, Choudhary R, Dev A, Chatterjee D, Handa S. A retrospective study to evaluate the impact of inpatient dermatological consultations on diagnostic accuracy in a tertiary care setting. Indian Dermatol Online J 2021;12:417-422. https://doi.org/10.4103/idoj.IDOJ_555_20 [ Links ]
17. De Paula Samorano-Lima L, Quitério LM, Sanches J Jr, Festo Neto C. Inpatient dermatology: Profile of patients and characteristics of admissions to a tertiary dermatology inpatient unit in São Paulo, Brazil. Int J Dermatol 212;53(6):685-691. https://doi.org/10.1111/j.1365-4632.2012.05818.x [ Links ]
18. Pomeranz J. Observations on the present and concerns about the future of dermatology and dermatopathology. Arch Dermatol 2000;136(1):83. https://doi.org/10.1001/archderm.136.L83 [ Links ]
19. Eedy D. Dermatology: A specialty in crisis. Clin Med 2015;15(6):509-510. https://doi.org/10.7861/clinmedicine.15-6-509 [ Links ]
20. Puri P, Wiggins M, Yousif M, et al. Evaluating the potential cost savings from inpatient dermatology consultations. J Eur Acad Dermatol Venereol 2021;35(12):e936-e338. https://doi.org/10.1111/jdv.17595 [ Links ]
21. Madigan LMFL. Where are we now with inpatient consultative dermatology? Assessing the value and evolution of this subspecialty over the past decade. J Am Acad Dermatol 2019;80(6):1804-1808. https://doi.org/10.1016/j.jaad.2019.01.031 [ Links ]
 Correspondence:
Correspondence:
L Mthembu
luandanm@gmail.com
Accepted 5 November 2023


{kind=link}
{kind=link}
{kind=link}