










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.114 n.1 Pretoria Jan. 2024
http://dx.doi.org/10.7196/samj.2024.v114i1.1132
RESEARCH
Pancreatic cancer mortality in South Africa: A case-control study
M L NhlekoI; I EdokaII, III; E MusengeIV
IMSc; Division of Epidemiology and Biostatistics, School of Public Health, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IIPhD; Health Economics and Epidemiology Research Office, Department of Internal Medicine, School of Clinical Medicine, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IIIPhD; School of Public Health, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IVPhD; Division of Epidemiology and Biostatistics, School of Public Health, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
ABSTRACT
BACKGROUND: There are variations in the numbers of pancreatic cancer deaths reported annually in South Africa (SA). Since pancreatic cancer deaths occurred in SA from 1997 to 2016, the number of cases has hugely increased, and reached 23 581 in both sexes. Sex differences are likely to contribute to the variations in the strength of associations between the risk factors and pancreatic cancer mortality
OBJECTIVE: To identify factors associated with an increased risk of pancreatic cancer mortality in SA
METHODS: A matched case-control study with 1:1 matching was conducted using data collected by Statistics SA from 1997 to 2016. Controls were randomly selected to be as similar as possible to the cases, and matched by age, sex and year of death. Conditional logistic regression was used to identify factors associated with pancreatic cancer mortality
RESULTS: This case-control study comprised a final selection of 23 581 cases (12 171 males and 11 410 females) and 23 581 controls (12 171 males and 11 410 females). A significantly increased risk of pancreatic cancer mortality was observed among males who were managers (odds ratio (OR) 2.99; 95% confidence interval (CI) 1.36 - 6.60; p=0.006) and craft and related trade workers (OR 1.89; 95% CI 1.14 - 3.14; p=0.013). Elevated risks of pancreatic cancer mortality were also found among females who were managers (OR 6.13; 95% CI 1.32 - 28.52; p=0.021), professionals (OR 2.12; 95% CI 1.24 - 3.63; p=0.006), clerical support workers (OR 3.78; 95% CI 1.79 -7.98; p=0.001) and elementary occupation workers (OR 1.41; 95% CI 0.99 - 2.00; p=0.059). Smoking was significantly associated with pancreatic cancer mortality in females (OR 1.36; 95% CI 1.02 - 1.82; p=0.039). Working in several occupations was associated with an increased risk of pancreatic cancer mortality in males (OR 1.31; 95% CI 1.01 - 1.71; p=0.045) and females (OR 1.66; 95% CI 1.30 - 2.12; p<0.001
CONCLUSION: Smoking and certain occupations increased the risk of pancreatic cancer mortality. Further research is needed to evaluate the associations between other extrinsic and intrinsic factors and pancreatic cancer mortality
Globally, where pancreatic cancer is defined as all types of cancers originating in the pancreas, it is the twelfth most common malignancy and the seventh leading cause of cancer death in both sexes.[1] Worldwide, there were 458 918 new cases of pancreatic cancer and 432 242 deaths in 2018.[2] In South Africa (SA), pancreatic cancer ranked seventh among all cancer deaths in 2020 in both sexes. Similarly, pancreatic cancer was the seventh leading cause of cancer death among males in SA in 2020, whereas it was the sixth in females. In 2020, a total of 1 982 cancer deaths were estimated to be due to pancreatic cancer in SA, of which 1 006 were males and 976 females.[3] However, there are variations in the numbers of pancreatic cancer deaths reported per year in SA. Since the calculation of the number of pancreatic cancer deaths that occurred in SA from 1997 to 2016, the number of cases has hugely increased, and reached 23 581.
The variations in pancreatic cancer incidence and mortality rates depend on geographical area, which might be attributed to different exposures. Approximately 80 - 85% of pancreatic cancer cases are diagnosed in stage IV, when it is impossible for the patients to benefit from curative surgery.[4] Uncertainties surrounding the causes of pancreatic cancer mortality and morbidity are huge, although epidemiological studies have reported the risk factors. Many risk factors, such as smoking, obesity, diabetes, occupation, alcohol consumption, pesticides, chronic pancreatitis and dietary components, are associated with pancreatic cancer mortality and morbidity.[5-13] In addition to the prevalence of risk factors, sex differences are likely to contribute to the variations in the strength of associations between the risk factors and pancreatic cancer mortality and morbidity. Few studies on pancreas cancer have been conducted in SA.[14,15] To date, no large study has examined the association between the risk factors and pancreatic cancer mortality in SA, although this disease is highly lethal. The high lethality of this cancer highlights the need to identify risk factors, which may be crucial for the prevention of this disease. The purpose of the present study was to identify factors associated with an increased risk of pancreatic cancer mortality in SA.
Methods
Study design and setting
This was a matched case-control study of data collected by Statistics SA (Stats SA) from 1997 to 2016.
Data and sample size
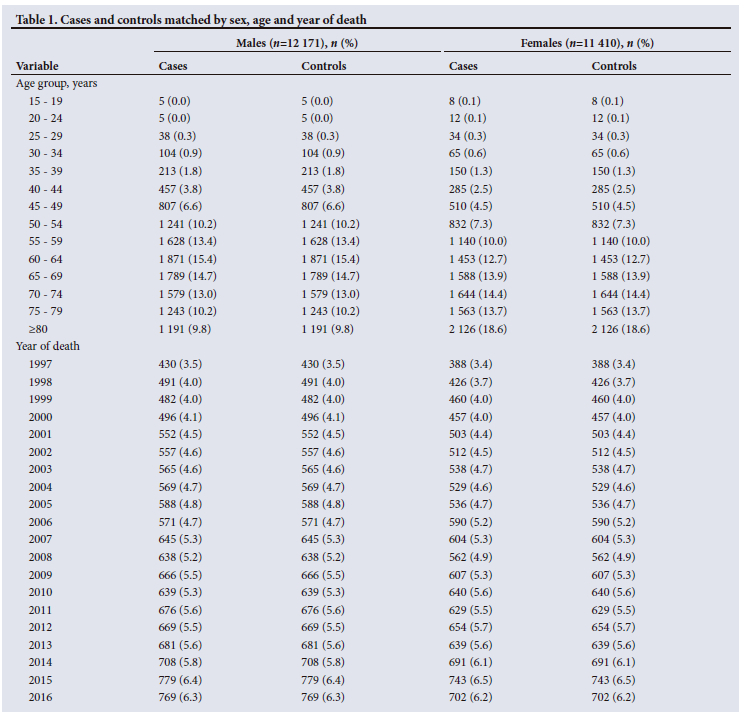
The mortality data were obtained from Stats SA, where the cause of death was based on death certificates. Stats SA is a national statistical service responsible for the compilation of mortality statistics indicated on medical certification of the cause of death registered with the Department of Home Affairs in SA. The underlying cause of death was coded using the 10th International Classification of Diseases codes (ICD-10). The selection of cases was restricted to individuals who died from pancreatic cancer (C25) in SA, whereas non-cancer-related deaths were selected as controls. The controls were randomly selected and matched to cases by age, sex and year of death, with a ratio of 1:1. This case-control study comprised a final selection of 23 581 cases and 23 581 controls. Overall, the balance was well achieved between the two groups in this study, that is, cases (n=12 171) and controls (n=12 171) in males, and cases (n=11 410) and controls (n=11 410) among females (Table 1). Males with a mean standard deviation (SD) age of 63.5 (12.4) years were in the case and control groups, whereas the mean (SD) age of females in these groups was 67.4 (13.0) years. The mortality data from Stats SA also contained important information about the study participants, including marital status, province of death, race, educational level, smoking status and occupation.
Statistical analysis
Data analysis was conducted using Stata software version 17 (StataCorp, USA), stratified by sex. For the descriptive analysis, the categorical variables were described in absolute (n) and relative (%) frequencies. To identify factors associated with pancreatic cancer mortality, a conditional logistic regression model was applied. We used a univariate model to identify the significant predictors for pancreatic cancer mortality. A p-value of <0.05 was considered statistically significant. Afterwards, a multivariate conditional logistic regression model was applied. Results were expressed as adjusted odds ratios (ORs) with 95% confidence intervals (CIs).
Results
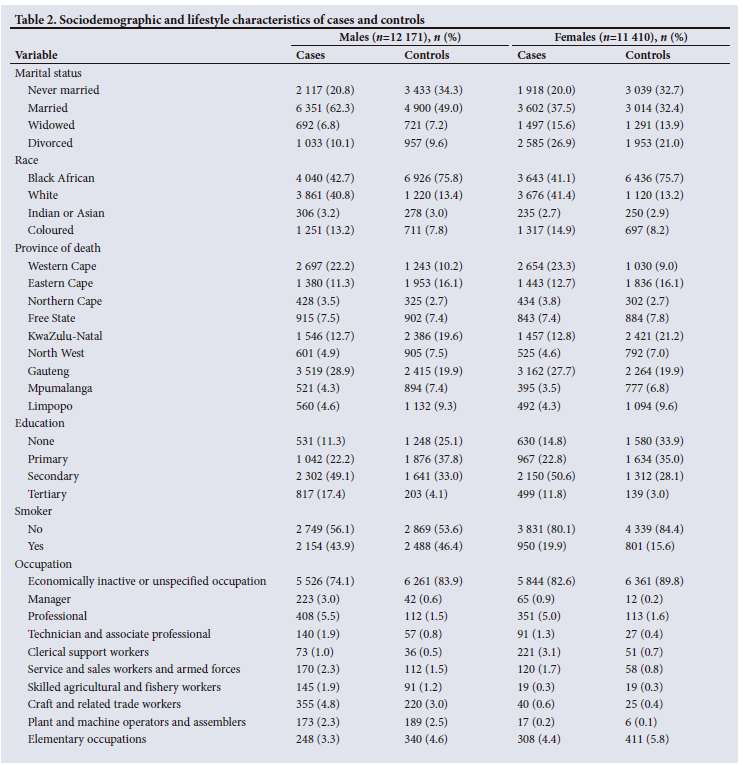
Of the 23 581 cases, 12 171 were males, and 11 410 were females. Controls were randomly selected to be as similar as possible to the cases, which defined a ratio of 1:1 between controls and cases. Most pancreatic cancer deaths occurred among males (n=6 351; 62.3%) and females (n=3 602; 37.5%) who were married. Non-cancer deaths accounted for >30% of males (n=4 900; 49.0%) and females (n=3 014; 32.4%) who were married. Widowed males (n=692; 6.8%) and females (n=1 497; 15.6%) reported the lowest pancreatic cancer mortality. The largest increase of cases was observed in black Africans (n=4 040; 42.7%), followed by white (n=3 861; 40.8%) and coloured (n=1 251; 13.2%) patients, and the greatest reduction was among Indians or Asians (n=306; 3.2%) in males. A similar pattern was observed among females, except that most cases occurred in whites and were followed by black Africans. In females, 3 676 whites (41.4%) and 3 643 black Africans (41.1%) were in the case group. Black Africans were more frequent among controls in males (n=6 926; 75.8%) and females (n=6 436; 75.7%). Gauteng Province displayed the highest proportion of pancreatic cancer deaths, regardless of sex. In males and females, 3 519 cases (28.9%) and 3 162 cases (27.7%), respectively, occurred in Gauteng. Northern Cape Province presented the lowest pancreatic cancer deaths among males (n=428; 3.5%), whereas Mpumalanga Province displayed the smallest number of cases in females (n=395; 3.5%). Among controls, Gauteng prevailed in males (n=2 415; 19.9%) and KwaZulu-Natal Province dominated in females (n=2 421; 21.2%). The majority of males (n=2 302, 49.1%) with secondary school education were in the case group, while 531 (11.3%) were illiterate. Females with secondary school education accounted for more than half (n=2 150, 50.6%) of cases, whereas 499 (11.8%) had tertiary education. Approximately 2 154 males (43.9%) in the case group and 950 females (19.9%) in this group were smokers. Among controls, >50% of males (n=2 869; 53.6%) and females (n=4 339; 84.4%) had never smoked. Most cases (n=408; 5.5%) were professional in males, while the largest reduction of cases was among clerical support workers (n=73; 1.0%). A significantly greater proportion of cases were among professionals (n=351; 5.0%) in females. In contrast, a small number of cases (n=17; 0.2%) were women who were plant and machine operators and assemblers (Table 2).
Factors associated with pancreatic cancer mortality
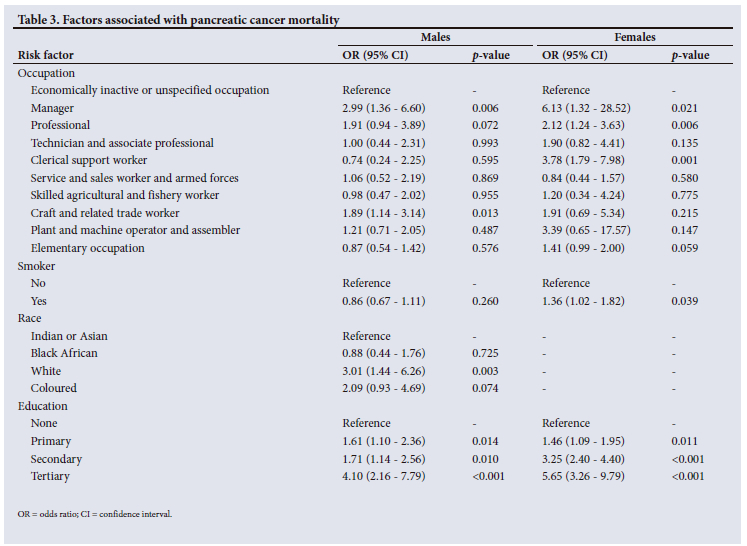
Table 3 presents the results of the analysis of association between sociodemographic and lifestyle risk factors and pancreatic cancer mortality. Applying conditional logistic regression, it was determined that occupation, smoking, race and education were associated with pancreatic cancer mortality. Males who were managers (OR 2.99; 95% CI 1.36 - 6.60; p=0.006) and craft and related trade workers (OR 1.89; 95% CI 1.14 - 3.14; p=0.013) were more likely than males in other occupations to die from pancreatic cancer. An elevation of pancreatic cancer mortality among white males (OR 3.01; 95% CI 1.44 - 6.26; p=0.003) was also observed. Significantly increased risks of pancreatic cancer mortality were found among females who were managers (OR 6.13; 95% CI 1.32 - 28.52; p=0.021), professionals (OR 2.12; 95% CI 1.24 - 3.63; p=0.0.006), clerical support workers (OR 3.78; 95% CI 1.79 - 7.98; p=0.001) and elementary occupation workers (OR 1.41; 95% CI 0.99 - 2.00; p=0.059). Increased risk of pancreatic cancer mortality also appeared among female smokers (OR 1.36; 95% CI 1.02 - 1.82; p=0.039). Males who attained primary school education (OR 1.61; 95% CI 1.10 - 2.36; p=0.014) were more likely than females (OR 1.46; 95% CI 1.09 - 1.95; p=0.011) with the same educational level to die from pancreatic cancer. In contrast, females who had secondary school education (OR 3.25; 95% CI 2.40 - 4.40; p<0.001) and tertiary education (OR 5.65; 95% CI 3.26 - 9.79; p<0.001) had higher risk of pancreatic cancer mortality than males who attained secondary school education (OR 1.71; 95% CI 1.14 - 2.56; p=0.010) and tertiary education (OR 4.10; 95% CI 2.16 - 7.79; p<0.001).
Association between occupations and pancreatic cancer mortality
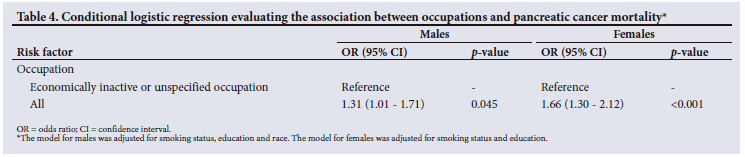
Table 4 shows adjusted ORs and their 95% CIs of pancreatic cancer mortality according to all occupations. Statistically significant increased risks of pancreatic cancer mortality were associated with all occupations in males and females. A significantly increased OR of 1.31 (95% CI 1.01 - 1.71; p=0.045) was observed among males who worked in several occupations. Results of the multivariate analysis also showed that females who reported occupations (OR 1.66; 95% CI 1.30 - 2.12; p<0.001) were at higher risk of pancreatic cancer mortality than females who did not report occupations.
Discussion
This case-control study of pancreatic cancer was based on mortality data provided by Stats SA from 1997 to 2016. The pancreatic cancer-related deaths increased during the study period, which may suggest an increased exposure to risk factors. Another possible explanation is the substantial increase in hepatopancreaticobiliary units in the country, leading to high diagnostic rates. Gauteng and Western Cape provinces presented higher cases compared with Eastern Cape and KwaZulu-Natal. The availability and infrastructure of tertiary healthcare are different between these two groups of provinces. Hence, it is possible that patients with pancreatic cancer were not diagnosed in under-resourced areas. There were more men than women who died from pancreatic cancer from 1997 to 2016. There is a high rate of unemployment in SA; hence, this aspect was also reflected by the enormous number of study participants classified as economically inactive or with unspecified occupations in this study. The workplace exposure, responses, carcinogenic potency, prevalence of risk factors and susceptibility may differ among men and women. Hence, the analyses were stratified by sex. Females in the case and control groups were slightly older than males. Cases were somewhat educated regardless of sex. Our findings further suggest that race, education, smoking and occupation were significant predictors of pancreatic cancer mortality. While males employed in managerial and craft and related trade occupations had a higher risk of death from cancer of the pancreas than other males, females who were managers, professionals, clerical support workers and elementary occupation workers were more likely than females in other occupations to die from this malignancy. Many workers employed in various occupations utilise solvents to perform their jobs. The increased risks of pancreatic cancer mortality among workers employed in various occupations may be due to exposure to solvents in the workplace. As solvents are common in different occupations, there is also the possibility of interactive effects of these solvents, which may increase the risk of death from pancreatic cancer.
These solvents are used for different purposes in industries. Workers employed in hospital-related occupations and industries and chemical petroleum processing are exposed to formaldehyde. This occupational exposure is associated with pancreas cancer.[16] Formaldehyde is widely used for preservation and disinfection as well as in the production of industrial chemical compounds. The chlorohydrin production workers who produced dichloromethane were at greater risk of dying from pancreatic and lymphopoietic cancers.[8] Dichloromethane is commonly used in the food and pharmaceutical industries. Our study confirmed some results from previous epidemiological studies of occupational cancer. We found an association between elementary occupations and pancreatic cancer mortality; this is further corroborated by previous studies that reported an excess risk among those who worked as garagemen, dry cleaners and service station workers.[17,18] Globally, around 100 000 chemicals are classified as commodities and many chemicals are invented yearly,[19] which contribute to economic growth and technological improvement. These hazardous occupational exposures may further increase the risk of pancreatic cancer mortality among workers. An excess in mortality of pancreatic cancer in an auto mechanics cohort study was reported,[20,21] and an excess risk of pancreatic cancer was observed among vehicle drivers and railroad workers.[22-24] Despite the association between occupational group and excess risk of pancreatic cancer mortality in this study, some differences in the strength of associations were recognised. Some of the occupational exposures are found in specific industries, and these risk factors may contribute to pancreatic cancer mortality and morbidity; this may explain these variations. Furthermore, SA is a large country with nine provinces, and the distribution of occupational groups and industries varies within the country. SA has both rural and urban areas; certain occupations are concentrated in urban areas, while others are located in rural areas. However, statistical power constraints limited the ability to investigate associations between occupational groups and pancreatic cancer mortality stratified by both place of death and sex. Given the mobility between occupations in SA, we did consider looking at the association between all occupations and pancreatic cancer mortality. Workers move between occupations when there are new job vacancies, to get higher wages and to improve the match between their skills and the skills required by each occupation. Our analysis suggested statistically significant increased risks of pancreatic cancer mortality among males and females who reported occupations. Due to initiatives that promote gender equality in SA, changes are occurring in the workplace. Women are increasingly being employed in sectors that were dominated by men in the past. Thus, women are exposed to potentially hazardous carcinogens in the workplace, which contribute to pancreatic cancer mortality and morbidity. It is possible to estimate the risk of pancreatic cancer in women based on studies that report the risk among men, but sometimes there is variability in the results.[25] Studies on occupational risk that focused only on men have been conducted in other countries,[26-28] but such information is limited in SA.
The association between smoking and pancreatic cancer mortality could be explained by the high prevalence of lifestyle risk factors. People start smoking at a young age in SA; as they grow, the duration of exposure to smoking also increases, which increases the risk of developing pancreas cancer, leading to death. The reality is that patients diagnosed with pancreatic cancer may die if this disease is not treated. Pancreatic cancer is associated with several intrinsic and extrinsic factors. Smoking is a well-established modifiable risk factor for pancreatic cancer,[29,30] while its cessation reduces the risk of this malignancy.[31,32] Cigarette smokers are exposed to a mixture of >8 000 compounds, and >70 of them are known carcinogens. Cigarette smoking causes at least 20 different types or subtypes of cancer, including pancreas cancer.[33] Smoking contributes to carcinogenesis through multiple biological mechanisms, involved in the early and late stages of carcinogenesis. Smoking cessation ends further increments to cumulative exposure to tobacco smoke regardless of the specific mechanisms that lead to the reduction of cancer risk. There is inconsistency surrounding the detrimental smoking-related association with pancreatic cancer risk stratified by sex; some studies report possible sex differences for the smoking-related association with pancreatic cancer,[34,35] while others do not show significant differences.[36,37]
Many study participants employed in various industries among cases were smokers. The combination of smoking with hazardous operations may increase the risk of pancreatic cancer mortality. In reality, workers are also exposed to other extrinsic and intrinsic factors contributing to pancreatic cancer mortality. Besides clinical, sociodemographic and environmental risk factors, it is possible that these workers were also alcohol drinkers, and there is an interactive effect of smoking and alcohol consumption. Understanding the associations between occupational and individual factors and pancreatic cancer mortality has the potential to reduce deaths from this disease. Avoidance of smoking, early diagnosis and treatment of pancreatic cancer, arrangement of working time and proper use of protective equipment at workplaces may reduce pancreatic cancer mortality.
Study strengths and limitations
The major strengths of this study include its relevance, size and availability of exposures. To the best of our knowledge, this is the first large case-control study that has examined the association between risk factors and pancreatic cancer mortality in SA. The availability of sociodemographic and lifestyle factors in the data enabled us to evaluate the association between these exposures and pancreatic cancer mortality. Another strength is the availability of data for both males and females, which allowed stratified analysis by sex. Despite these strengths, the study suffered from some limitations. Pancreatic cancer was not classified according to the stage at diagnosis. We lack information about alcohol consumption, which is associated with an increased risk of pancreatic cancer mortality. We lack detailed information about occupational risk factors. Information about the duration of smoking and employment was not captured. Also, we lack information about the amount of cigarette smoking. Therefore, it was not possible to examine the dose-response pattern of smoking.
Conclusion
This study helped to resolve concerns about the scarcity of epidemiological studies on pancreatic cancer mortality in SA. The findings were informative and provided evidence for an association between smoking and pancreatic cancer mortality. Many investigators have reported cigarette smoking as a predictor of pancreatic cancer mortality. In addition to this lifestyle factor, our study suggested that population group, educational attainment and occupation were associated with elevated risks of pancreatic cancer mortality. Although we identified the predictors of pancreatic cancer mortality, further research evaluating the association between other extrinsic and intrinsic factors and pancreatic cancer mortality is needed to address the limitations of this study.
Declaration. The research for this study was done in partial fulfilment of the requirements for MLN's PhD in Public Health at the University of the Witwatersrand.
Acknowledgements. The authors would like to sincerely thank Stats SA for providing the data.
Author contributions. MLN conceptualised the study, designed the study, analysed the data, compiled the results, interpreted the results and wrote the manuscript. IE and EM contributed to concept development and revisions to the manuscript. All authors read the final draft of the manuscript and approved it for publication.
Funding. The work reported herein was made possible through funding by the SA Medical Research Council (SAMRC) through its Division of Research Capacity Development under the Bongani Mayosi National Health Scholars Programme from funding received from the Public Health Enhancement Fund/SA National Department of Health. The content hereof is the sole responsibility of the authors and does not necessarily represent the official views of the SAMRC. The authors acknowledge financial support for the study from the National Research Foundation and TATA Africa Holdings.
Conflicts of interest. None.
References
1. Arnold M, Abnet CC, Neale RE, et al. Global burden of 5 major types of gastrointestinal cancer. Gastroenterology 2020;159(1):335-349. https://doi.org/10.1053/j.gastro.2020.02.068 [ Links ]
2. Huang J, Lok V, Ngai CH, et al. Worldwide burden of, risk factors for, and trends in pancreatic cancer. Gastroenterology 2021;160(3):744-754. https://doi.org/10.1053/j.gastro.2020.10.007 [ Links ]
3. Ferlay J, Ervik M, Lam F, et al. Global Cancer Observatory: Cancer Today. Lyon, France: International Agency for Research on Cancer, 2020. https://gco.iarc.fr/today (accessed 28 April 2023). [ Links ]
4. Mizrahi JD, Surana R, Valle JW, Shroff RT. Pancreatic cancer. Lancet 2020;395(10242):2008-2020. https://doi.org/10.1016/s0140-6736(20)30974-0 [ Links ]
5. Gheorghe G, Diaconu CC, Ionescu V, et al. Risk factors for pancreatic cancer: Emerging role of viral hepatitis. J Personalised Med 2022;12(1):83. https://doi.org/10.3390/jpm12010083 [ Links ]
6. Coughlin SS, Calle EE, Patel AV, Thun MJ. Predictors ofpancreatic cancer mortality among a large cohort of United States adults. Cancer Causes Control 2000;11(10):915-923. https://doi.org/10.1023/a:1026580131793 [ Links ]
7. Gapstur SM, Jacobs EJ, Deka A, McCullough ML, Patel AV, Thun MJ. Association of alcohol intake with pancreatic cancer mortality in never smokers. Arch Int Med 2011;171(5):444-451. https://doi.org/10.1001/archinternmed.2010.536 [ Links ]
8. Kernan GJ, Ji BT, Dosemeci M, Silverman DT, Balbus J, Zahm SH. Occupational risk factors for pancreatic cancer: A case-control study based on death certificates from 24 US states. Am J Industrial Med 1999;36(2):260-270. https://doi.org/10.1002/(sici)1097-0274(199908)36:2<260::aid-ajim5>3.0.co;2-p [ Links ]
9. Dhungel B, Murakami T, Gilmour S, Ikeda S, Wada K. Occupation-and industry-specific cancer mortality among Japanese women from 1980 to 2015. BMC Pub Health 2022;22(1):2003. https://doi.org/10.1186/s12889-022-14304-4 [ Links ]
10. Hassan MM, Bondy ML, Wolff RA, et al. Risk factors for pancreatic cancer: Case-control study. Am J Gastroenterol 2007;102(12):2696-2707. https://doi.org/10.1111/j.1572-0241.2007.01510.x [ Links ]
11. Pickle LW, Gottlieb MS. Pancreatic cancer mortality in Louisiana. Am J Public Health 1980;70(3):256-259. https://doi.org/10.2105/ajph.70.3.256 [ Links ]
12. Clary T, Ritz B. Pancreatic cancer mortality and organochlorine pesticide exposure in California, 1989 -1996. Am J Industrial Med 2003;43(3):306-313. https://doi.org/10.1002/ajim.10188 [ Links ]
13. Coughlin SS, Calle EE, Teras LR, Petrelli J, Thun MJ. Diabetes mellitus as a predictor of cancer mortality in a large cohort of US adults. Am J Epidemiol 2004;159(12):1160-1167. https://doi.org/10.1093/aje/kwh161 [ Links ]
14. Jeppe CY, Smith MD. Transversal descriptive study of xenobiotic exposures in patients with chronic pancreatitis and pancreatic cancer. JOP 2008;9(2):235-239. [ Links ]
15. Yako YY, Brand M, Smith M, Kruger D. Inflammatory cytokines and angiogenic factors as potential biomarkers in South African pancreatic ductal adenocarcinoma patients: A preliminary report. Pancreatology 2017;17(3):438-444. https://doi.org/10.1016/j.pan.2017.03.003 [ Links ]
16. Collins JJ, Esmen NA, Hall TA. A review and meta-analysis of formaldehyde exposure and pancreatic cancer. Am J Industrial Med 2001;39(3):336-345. https://doi.org/10.1002/1097-0274(200103)39:3<336::aid-ajim1022>3.0.co;2-k [ Links ]
17. Weiderpass E, Partanen T, Kaaks R, et al. Occurrence, trends and environmental etiology of pancreatic cancer. Scand J Work Environ Health 1998;24(3):165-174. https://doi.org/10.5271/sjweh.295 [ Links ]
18. Lin RS, Kessler II. A multifactorial model for pancreatic cancer in man: Epidemiologic evidence. JAMA 1981345(2):147-152. https://doi.org/10.1001/jama.245.2.147 [ Links ]
19. Egeghy PP, Judson R, Gangwal S, et al. The exposure data landscape for manufactured chemicals. Sci Total Environ 2012;414:159-166. https://doi.org/10.1016/j.scitotenv.2011.10.046 [ Links ]
20. Santos AS, Martins AA, Gonqalves ES, Meyer A. Mortality from selected cancers among Brazilian mechanics. Asian Pacific J Cancer Preven 2020;21(6):1779-1786. https://doi.org/10.31557/apjcp.2020.2L6.1779 [ Links ]
21. Hansen ES. Mortality of auto mechanics: A ten-year follow-up. Scand J Work Environ Health 1989;15(1):43-46. https://doi.org/10.5271/sjweh.1883 [ Links ]
22. Zhang Y, Cantor KP, Lynch CF, Zhu Y, Zheng T. Occupation and risk of pancreatic cancer: A population-based case-control study in Iowa. J Occup Environ Med 2005;47(4):392-398. https://doi.org/10.1097/01.jom.0000158707.88801.f5 [ Links ]
23. Boffetta P, Stellman SD, Garfinkel L. Diesel exhaust exposure and mortality among males in the American Cancer Society prospective study. Am J Industrial Med 1988;14(4):403-415. https://doi.org/10.1002/ajim.4700140405 [ Links ]
24. Partanen T, Kauppinen T, Degerth R, et al. Pancreatic cancer in industrial branches and occupations in Finland. Am J Industrial Med 1994;25(6):851-866. https://doi.org/10.1002/ajim.4700250609 [ Links ]
25. Blair A, Zahm SH, Silverman DT. Occupational cancer among women: Research status and methodologic considerations. Am J Industrial Med 1999;36(1):6-17. https://doi.org/10.1002/(sici)1097-0274(199907)36:1<6::aid-ajim2>3.0.co;2-f [ Links ]
26. Singh S, McDonald JT, Ilie G, Adisesh A. An examination of the association between lifetime history of prostate and pancreatic cancer diagnosis and occupation in a population sample of Canadians. PLoS ONE 2020;15(2):e0227622. https://doi.org/10.1371/journalpone.0227622 [ Links ]
27. Zaitsu M, Kaneko R, Takeuchi T, Sato Y, Kobayashi Y, Kawachi I. Occupational class and male cancer incidence: Nationwide, multicenter, hospital-based case-control study in Japan. Cancer Med 2019;8(2):795-813. https://doi.org/10.1002/cam4.1945 [ Links ]
28. Mallin K, Rubin M, Joo E. Occupational cancer mortality in Illinois white and black males, 1979 - 1984, for seven cancer sites. Am J Industrial Med 1989;15(6):699-717. https://doi.org/10.1002/ajim.4700150609 [ Links ]
29. Nam DJ, Oh CM, Ha E, et al. The association of pancreatic cancer incidence with smoking status and smoking amount in Korean men. Epidemiol Health 2022;44:e2022040. https://doi.org/10.4178/epih.e2022040 [ Links ]
30. Ben QW, Liu J, Sun YW, Wang LF, Zou DW, Yuan YZ. Cigarette smoking and mortality in patients with pancreatic cancer: A systematic review and meta-analysis. Pancreas 2019;48(8):985-995. https://doi.org/10.1097/mpa.0000000000001383 [ Links ]
31. Gram IT, Park SY, Wilkens LR, le Marchand L, Setiawan VW. Smoking and pancreatic cancer: A sex-specific analysis in the multiethnic cohort study. Cancer Causes Control 2023;34(1):89-100. https://doi.org/10.1007/s10552-022-01637-z [ Links ]
32. Molina-Montes E, van Hoogstraten L, Gomez-Rubio P, et al. Pancreatic cancer risk in relation to lifetime smoking patterns, tobacco type, and dose-response relationships. Cancer Epidemiol Biomarkers Preven 2020;29(5):1009-1018. https://doiorg/10.1158/1055-9965.epi-19-1027 [ Links ]
33. Wild CP, Weiderpass E, Stewart BW World Cancer Report: Cancer Research for Cancer Prevention. Lyon: International Agency for Research on Cancer, 2020. https://publications.iarc.fr/586 (accessed 30 April 2023). [ Links ]
34. Hayden JA, van der Windt DA, Cartwright JL, Cöté P, Bombardier C. Assessing bias in studies ofprognostic factors. Ann Internal Med 2013;158(4):280-286. https://doi.org/10.7326/0003-4819-158-4-201302190-00009 [ Links ]
35. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and metaanalyses: The PRISMA statement. Ann Internal Med 2009;151(4):264-269. https://doi.org/10.1371/journal.pmed.1000097 [ Links ]
36. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ 2003;327(7414):557-560. https://doi.org/10.1136/bmj.327.7414.557 [ Links ]
37. Greenland S, Longnecker MP. Methods for trend estimation from summarised dose-response data, with applications to meta-analysis. Am J Epidemiol 1992;135(11):1301-1309. https://doi.org/10.1093/oxfordjournals.aje.a116237 [ Links ]
 Correspondence:
Correspondence:
M L Nhleko
mandlakayise.nhleko@gmail.com
Accepted 30 October 2023


{kind=link}
{kind=link}
{kind=link}
{kind=link}