










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.113 n.12 Pretoria Dec. 2023
http://dx.doi.org/10.7196/samj.2023.v113i12.971
RESEARCH
An outbreak within an outbreak: The impact of infection prevention and control strategies on hospital-acquired infections and the occurrence of multidrug-resistant organisms during the COVID-19 pandemic
B MashigoI; A ParkerII, III; U LallaIV; B W AllwoodV; M S MoollaVI; T LovelockVII; C F N KoegelenbergVIII
IMB ChB; Division of Pulmonology, Department of Medicine, Stellenbosch University and Tygerberg Hospital, Cape Town, South Africa
IIFCP (SA), Cert ID (SA); Unit for Infection Prevention and Control, Tygerberg Hospital, Cape Town, South Africa
IIIFCP (SA), Cert ID (SA); Division of Infectious Diseases, Department of Medicine, Stellenbosch University and Tygerberg Hospital, Cape Town, South Africa
IVFCP (SA), Cert Crit Care (SA) Phys; Division of Pulmonology, Department of Medicine, Stellenbosch University and Tygerberg Hospital, Cape Town, South Africa
VFCP (SA), PhD; Division of Pulmonology, Department of Medicine, Stellenbosch University and Tygerberg Hospital, Cape Town, South Africa
VIMB ChB, FCP (SA); Division of Pulmonology, Department of Medicine, Stellenbosch University and Tygerberg Hospital, Cape Town, South Africa
VIIMB ChB, FCP (SA); Division of Infectious Diseases, Department of Medicine, Stellenbosch University and Tygerberg Hospital, Cape Town, South Africa
VIIIFCP (SA), PhD; Division of Pulmonology, Department of Medicine, Stellenbosch University and Tygerberg Hospital, Cape Town, South Africa
ABSTRACT
BACKGROUND: The coronavirus disease 2019 (COVID-19) pandemic placed an unprecedented strain on intensive care units (ICUs) in South Africa. Infection prevention and control (IPC) strategies were highlighted to minimise the risk to healthcare workers and for the protection of patients from contracting hospital-acquired infections (HAIs). During the third wave, our institution adopted a shift system to address severe burnout among ICU personnel. We noted an upstroke in the occurrence of HAIs, specifically carbapenem-resistant Enterobacterales (CRE) and multidrug-resistant (MDR) Acinetobacter baumannii
OBJECTIVES: To report these outbreaks, compare the rate of CRE and A. baumannii infections with the first COVID-19 wave and to analyse its impact on patient outcomes
METHOD: We retrospectively analysed data from a prospectively collected registry involving all adult patients with severe COVID-19 admitted to the dedicated COVID-19 ICU from May 2021 to September 2021. Information from the admission database, including the patients' demographics, comorbidities, laboratory results and length of ICU stay were extracted
RESULTS: Ninety patients were admitted with severe COVID-19 during the third wave. There was an outbreak of both CRE (the majority Klebsiella pneumoniae) and A. baumannii. Furthermore, 18 patients cultured the same CRE organism, and 25 patients cultured the environmental organism A. baumannii. The HAI rate was significantly higher compared with the first wave published data: 59/90 (65.6%) v. 73/363 (20.1%, p<0.01). Patients with any HAI had a longer mean stay in ICU (10.1 days v. 6.7 days (p<0.01) and a higher mortality of 48/59 (81%) v. 19/31 (61%) (p=0.05
CONCLUSION: We observed a very significant rise in HAIs in the COVID-19 ICU during the third wave compared with the first, with almost three times as many patients developing HAIs. Unsurprisingly, it was associated with a longer mean stay in ICU and a higher mortality. The outbreak of both CRE and A. baumannii, and the fact that many patients cultured the same CRE organism and A. baumannii, strongly suggests that a critical breakdown in IPC measures had occurred
The coronavirus disease 2019 (COVID-19) pandemic placed an unprecedented strain on intensive care units (ICUs) in South Africa (SA) and across the globe.[1] Novel ways of expanding respiratory support even outside the intensive care environment were described, and infection prevention and control (IPC) strategies were highlighted, both for protection of healthcare workers from infection with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), but also protection of patients from contracting hospital-acquired infections (HAIs).[2,3]
Antimicrobial resistance (AMR) is recognised as a major threat to human health by the World Health Organization (WHO).[4] Bacterial AMR was estimated to be responsible for 4.95 million deaths globally in 2019, with the highest deaths attributed to bacterial AMR in western sub-Saharan Africa.[5] IPC measures to combat rising AMR are highlighted as strategic objectives in the global action plan for AMR,[4] and IPC is a key research priority in the global research agenda for AMR.[6] Local and international data suggested that the overall rate of bacterial co-infection in patients with confirmed SARS-CoV-2 was low on admission.[7-9] However, published data from our institution from the first wave have already suggested the occurrence of multidrug-resistant (MDR) HAIs in patients admitted to the ICU with COVID-19, with Acinetobacter baumannii being the most common isolate.[7]
During the third wave of COVID-19, our institution adopted an extensive shift system to address severe burnout among ICU personnel, which led to a large pool of personnel performing limited numbers of shifts, some only after hours. This was potentially responsible for less stringent IPC measures, as many of the staff did not routinely work in an ICU environment. The IPC department was also severely short-staffed, with reported staff burnout and resignations. IPC staff were also rerouted to assist in COVID-19 testing and vaccination centres. An upstroke in the occurrence of not only nosocomial sepsis, but specifically carbapenem-resistant Enterobacterales (CRE) and MDR A. baumannii was noted.
The aims of this study were to report this outbreak, to compare the rate of CRE and A. baumannii infections with published data from the first COVID-19 wave and to analyse its impact on patient outcomes.
Methods
We retrospectively analysed data from a prospectively collected registry involving all adult patients with severe COVID-19 admitted to the dedicated COVID-19 ICU at Tygerberg Hospital, Cape Town, SA, from May 2021 to September 2021, corresponding to the third wave of SARS-CoV-2 infections. Of note is that 'incidental' SARS-CoV-2-positive patients who required ICU admission were admitted elsewhere in the hospital and were not included. Ethical approval was obtained from the Health Research Ethics Committee of Stellenbosch University (ref. no S21/04/005_COVID-19_Sub-study N20/04/002-14897). Information from the admission database, including the patient demographics (age and sex), comorbidities, laboratory results and length of ICU stay, was extracted.
All cultures were submitted to the on-site National Health Laboratory Services (NHLS) microbiology laboratory and processed using standard procedures. Identification and antibiotic susceptibility testing of cultured isolates involved use of the automated VITEK 2 system (Biomérieux, France) and was supplemented where necessary with E-test (Biomérieux, France) to confirm the minimum inhibitory concentration (MIC) of ertapenem, imipenem and meropenem. MIC breakpoints for Enterobacterales were <1 mg/L (imipenem and meropenem) and <0.5 mg/L (ertapenem) for susceptible isolates, 2 mg/L (imipenem and meropenem) and 1 mg/L (ertapenem) for intermediately resistant isolates, and >4 mg/L (imipenem and meropenem) and >2 mg/L (ertapenem) for resistant isolates. MIC breakpoints for A. baumannii were <2 mg/L (imipenem and meropenem), 4 mg/L (imipenem and meropenem) for intermediately resistant isolates, and >8 mg/L (imipenem and meropenem) for resistant isolates.
Positive culture results were deduplicated based on site of sample collection, with a positive result showing the same pathogen with the same susceptibility profile within a 5-day period being considered a single episode. Organisms such as coagulase-negative staphylococci (CoNS) and Bacillus cereus were considered contaminants if they were only cultured once, or pathogens if they were cultured more than once in the same patient in an appropriate setting (e.g. central line-associated bloodstream infection) where the attending physician deemed these cultures clinically significant.
Infection with a bacterial isolate was diagnosed once the isolate was cultured from a given site, and according to the treating clinician the associated clinical manifestations were due to infection. HAI was defined as infection detected >48 hours after hospital admission and not incubating at the time of admission; cultures prior to that period were considered early cultures. Of note is that antibiotics were not routinely prescribed on admission, as previous published data from the first wave by Moolla et al.[7] from our institution showed a low incidence of early bacterial infection.
Statistical analysis was performed using SPSS version 28 (IBM Corp., USA). Statistical significance was set at p<0.05. Pearson's χ2 test was used to identify associations between categorical variables and the outcomes of interest. When comparing the means of continuous data, t-tests were used to assess normally distributed variables, while the non-parametric Wilcoxon rank-sum test was used to assess variables that did not follow a normal distribution pattern.
Results
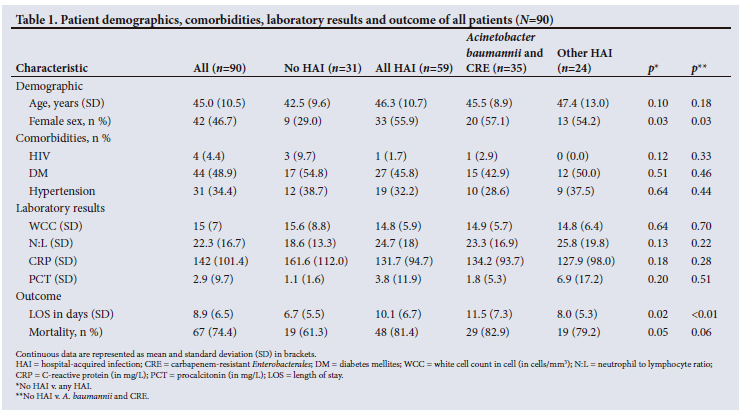
There were 90 patients admitted with severe COVID-19 pneumonia during the third wave. General patient demographics, comorbidities, laboratory results and outcome of all admissions are summarised in Table 1. Of note is the significant association with female sex and any HAI: 55.9% (33/59) v. 29.0% (33/59, p=0.03). There was no association between comorbidities and HAI. Laboratory results on admission also did not predict HAI during the subsequent admission.
Patients with any HAI had a longer mean stay in ICU (10.1 days v. 6.7 days (p<0.01) and a higher mortality of 81.4% (48/59) v. 61.3% (19/31, p=0.05).
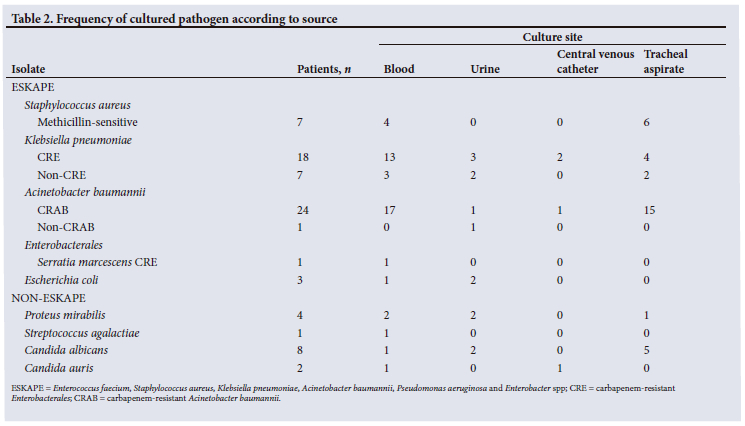
The HAI rate was significantly higher compared with the first wave published data:[7] 65.6% (59/90) v. 20.1% (73/363, p<0.01). The details (sites, isolates and susceptibility profile) of cultures are summarised in Table 2. Most organisms cultured were from the ESKAPE group of pathogens. ESKAPE organisms were cultured in 61 patients of the total 90 (68%), v. 15 patients (17%) who cultured the non-ESKAPE organisms. Of these, A. baumannii was cultured 35 times in 25 patients, with only one isolate which was carbapenem-susceptible. Most Klebsiella pneumoniae were carbapenem-resistant. In total, 23 cultures of CRE were grown from 18 patients, mostly K. pneumoniae, with only one culture of Serratia marcescens.
Discussion
We observed a very significant rise in HAIs, specifically due to CRE and A. baumannii, in the COVID-19 ICU during the third wave compared with the first, with almost three times as many patients developing nosocomial sepsis. Unsurprisingly, it was associated with a longer mean stay in ICU and a higher mortality. The outbreak of both CRE (the majority K. pneumoniae) and A. baumannii was alarming. Furthermore, the facts that 18 patients cultured the same CRE organism, and 25 patients cultured the environmental organism A. baumannii, strongly suggested that a critical breakdown in IPC measures had occurred.
Close to the end of the third wave, on 2 September 2021, the decision was made to stop all new admissions the COVID-19 ICU as all patients (7 of the 10-bed capacity at the time) had cultured either a CRE and/or MDR A. baumannii. New ICU admissions were diverted to an alternative ICU in the facility, whereafter the dedicated COVID-19 ICU resumed activities 1 week later, following terminal cleaning of the entire unit and IPC training of all involved staff members. There were no new cases in the 6-week period thereafter, emphasising the critical importance of simple IPC measures to prevent HAI.
The clinical and statistical differences between our findings and those reported by Moolla et al.[7] are striking. During the first wave, the COVID-19 ICU's capacity exceeded 40 beds, and 363 patients were admitted. Only 73 patients (20.1%) had positive cultures later during their stay. The most frequently isolated pathogens at all sites were A. baumannii (n=54). As with our study, length of ICU stay (p<0.001) was associated with positive cultures. Differences between the ICU response between the waves need to be highlighted: during the first wave, many patients were supported with high-flow nasal oxygen (HFNO) in the ICU (due to greater bed capacity), which was shown to be associated with a decreased risk of HAI.[7,10] Furthermore, doctors performed a 3-month rotation, all the nursing staff were ICU-trained and IPC practices were constantly reinforced. However, during the third wave, the ICU's capacity was much lower and was reserved for ventilated patients, as HFNO and other forms of respiratory support were administered outside the ICU. Doctors performed single shifts (often one per week), and non-ICU trained nursing staff were diverted to ICU. Although these measures were deemed necessary to reduce strain on the workforce, they undoubtedly impacted on IPC processes.
In a meta-analysis that included data from 35 263 patients with COVID-19 from China, the middle east, Southeast Asia, Europe and North America, Langford et al.[9] reported bacterial infection after presentation in 14.3% of patients. In contrast, the incidence of nosocomial CRE and A. baumannii infection was 38.9% (35/90) in our cohort.
Our study has some unique strengths, particularly the fact that we had accurate historical data to compare the incidence of nosocomial infections. The retrospective design is an inherent limitation. Although the data were captured prospectively, not all data points were captured serially (e.g. PCT), which limited the value analysis to admission investigations.
Conclusion
In conclusion, the incidence of nosocomial sepsis was three times higher in the third wave and associated with a longer mean stay in ICU and a higher mortality. The outbreak of CRE and A. baumannii infections was alarming, suggesting a breakdown in IPC practices. Subsequent outbreak resolution after environmental cleaning and IPC training of staff emphasises the critical importance of basic IPC measures to prevent HAI.
Declaration. The research for this study was done in partial fulfilment of the requirements for BM's MMed (Internal Medicine) degree at Stellenbosch University.
Acknowledgements. We acknowledge the input Mr Daniel Mashishi (Epidemiology and Biostatistics, Stellenbosch University) for his assistance with the statistical analysis.
Author contributions. BM and CFNK designed the study and BM wrote the manuscript. BM and MSM collected the data, which were analysed by CK. The study was supervised by CFNK. All co-authors reviewed and approved the manuscript.
Funding. None.
Conflicts of interest. None.
References
1. Parker A, Karamchand S, Schrueder N, Lahri S, Rabie H, Aucamp M. Leadership and early strategic response to the SARS- CoV-2 pandemic at a COVID-19 designated hospital in South Africa. S Afr Med J 2020;110(6):463-465. https://doi.org/10.7196/SAMJ.2020.v110i6.14809 [ Links ]
2. Broadhurst AGB, Botha C, Calligaro G, et al. The optimal management of the patient with COVID-19 pneumonia: HFNC, NIV/CPAP or mechanical ventilation? Afr J Thorac Crit Care Med 2022;28(3):119-128. https://doi.org/10.7196/AJTCCM.2022.v28i3.241 [ Links ]
3. Dheda K, Charalambous S, Karat AS, et al. A position statement and practical guide to the use of particulate filtering facepiece respirators (N95, FFP2 or equivalent) for South African health workers exposed to respiratory pathogens including Mycobacterium tuberculosis and SARS-CoV-2. Afr J Thorac Crit Care Med 2021;27(4):177-186. https://doi.org/10.7196/AJTCCM.2021.v27i4.173 [ Links ]
4. World Health Organization. Global action plan on antimicrobial resistance. Geneva: WHO, 2015. https://www.who.int/publications/i/item/9789241509763 (accessed 7 June 2023). [ Links ]
5. Murray CJL, Ikuta KS, Sharara F, et al. Global burden of bacterial antimicrobial resistance in 2019: A systematic analysis. Lancet 2022;399(10325):629-655. https://doi.org/10.1016/s0140-6736(21)02724-0 [ Links ]
6. World Health Organization. Global research agenda for antimicrobial resistance in human health. Geneva: WHO, 2023. https://www.who.int/publications/m/item/global-research-agenda-for-antimicrobial-resistance-in-human-health (accessed 7 June 2023). [ Links ]
7. Moolla MS, Reddy K, Fwemba I, et al. Bacterial infection, antibiotic use and COVID-19: Lessons from the intensive care unit. S Afr Med J 2021;111(6):575-581. https://doi.org/10.7196/SAMJ.2021.v111i6.15590 [ Links ]
8. Lansbury L, Lim B, Baskaran V, Lim WS. Co-infections in people with COVID-19: A systematic review and meta-analysis. J Infect 2020;81(2):266-275. https://do.org/10.2139/ssrn.3594598 [ Links ]
9. Langford BJ, So M, Raybardhan S, et al. Bacterial co-infection and secondary infection in patients with COVID-19: A living rapid review and meta-analysis. Clin Microbiol Infect 2020;26(12):1622-1629. https://doi.org/10.1016/j.cmi.2020.07.016 [ Links ]
10. Calligaro GL, Lalla U, Audley G, et al. The utility of high-flow nasal oxygen for severe COVID-19 pneumonia in a resource-constrained setting: A multi-centre prospective observational study. Lancet eCLin Med 2020;28:100570. https://doi.org/10.1016/j.eclinm.2020.100570 [ Links ]
 Correspondence:
Correspondence:
B Mashigo
be.mashigo@gmail.com
Accepted 19 October 2023


{kind=link}
{kind=link}