










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.113 n.12 Pretoria Dec. 2023
http://dx.doi.org/10.7196/samj.2023.v113i12.1066
RESEARCH
Antivirals for the treatment of mild and moderate COVID-19 in South Africa
R PerumalI; V NaidooII; S GovenderII; T N GengiahIII
IMB ChB, PhD; Centre for the AIDS Programme of Research in South Africa, Durban, South Africa
IIBPharm; Centre for the AIDS Programme of Research in South Africa, Durban, South Africa
IIIBPharm, PhD; Centre for the AIDS Programme of Research in South Africa, Durban, South Africa
ABSTRACT
While the majority of COVID-19 cases in South Africa (SA) are mild, patients with severe COVID-19 requiring hospitalisation present with significant morbidity and mortality and place a substantial burden on healthcare services. Given the low vaccine uptake in SA and other low- and middle-income countries in sub-Saharan Africa, the high prevalence of comorbidities and limited healthcare system capacity, evidence-based interventions that reduce the risk of severe disease and death should be considered for implementation. Several antiviral classes have been newly developed or repurposed to treat COVID-19 early after infection to retard progression to severe disease and reduce the risk of death, particularly in the elderly and/or in patients with comorbidities. COVID-19 antivirals such as remdesivir, nirmatrelvir/ ritonavir and molnupiravir are safe and cost-effective and have received either full approval or emergency use authorisation from regulators. Using a proposed test-and-treat strategy, judicious use of antivirals could be impactful.
The COVID-19 pandemic resulted in excessive loss of human life and destabilised healthcare systems, economies and social structures globally. Up to March 2023, over 680 million cases of COVID-19 had been reported globally, with an associated 6.8 million deaths.[1] The burden of COVID-19 has been heterogeneously distributed across countries and regions, largely driven by disparities in social, economic and environmental factors.[2] In Africa, as of March 2023, there have been ~9.5 million cases and ~175 000 deaths,[1] with South Africa (SA) reporting the highest number of cases and deaths on the continent, ~4 million and 100 000, respectively.[3]
The severity of COVID-19 infection ranges from mild to critical, with critical disease resulting in death in 0.5 - 2% of cases.[4] Early in the pandemic (December 2019 - February 2020; Wuhan-Hu-1), 81% of cases were reported as mild or moderate, 14% severe and 5% critical.'51 With the development of variants over time, disease severity associated with Alpha, Gamma and Delta variants was comparable, while Omicron infections were associated with less severe disease.'61 During the Omicron wave in SA, 8.3% of patients required hospitalisation, compared with 12.9%, 12.6% and 10.0% in the D614G (first), Beta (second) and Delta (third) waves. Of these admissions, 52.3%, 63.4%, 63.0% and 33.6% were severe or critical disease during the D614G, Beta, Delta and Omicron waves, respectively.'71 Severe and critical COVID-19 places a substantial burden on health systems owing to the need for hospitalisation, supplementary oxygen, organ support and pharmacotherapy.
Constrained resources and limited diagnostic capabilities have resulted in the true burden of COVID-19 in low- and middle-income countries (LMICs) being poorly characterised.[8] A retrospective data analysis (2020 - 2021) found that of an estimated 505.6 million infections in Africa, only 1.4% were reported.[9] Furthermore, modelling for excess mortality between 3 May 2020 and 27 March 2021 revealed 150 271 excess deaths, most of which were attributable to unreported COVID-19.[8] In SA, the economic cost of caring for a patient with severe COVID-19 was estimated at ZAR13 800 -ZAR14 300 daily.[10,11] Between May 2020 and December 2022, SA reported 22 968 intensive care unit (ICU) admissions related to severe COVID-19.[12-14] In addition to financial and economic costs, the COVID-19 pandemic has had a significant impact on human resources, including medical staff, allied health professionals, nursing and support staff.[11] Furthermore, the World Bank reported that the disease has pushed between 88 million and 115 million people into extreme poverty.[15,16]
Although mitigation strategies such as vaccination, the use of personal protective equipment (PPE), general infection prevention and control measures and social distancing have played a role in the reduction of COVID-19 transmission, these strategies have significant limitations in LMICs. More than 80% of the population has probably been infected at least once since the start of the pandemic, evident by the high seroprevalence of SARS-CoV-2 antibodies.[17] Supply-chain and access-related challenges have limited the efficacy of vaccines and PPE as a strategy to curb the burden of COVID-19.[18] In addition, the efficacy of vaccines is limited in populations diagnosed with malignancies, particularly blood cancers, as well as immunosuppressed individuals.[19] Individuals with allergies to vaccine excipients and those who have experienced allergic reactions to the initial dose of the COVID-19 vaccine are unable to vaccinate, with those opting not to vaccinate also contributing to the unvaccinated population. As a result, we can no longer rely solely on vaccination, and so a 'vaccination plus' strategy must be adopted in order to reduce the global burden of COVID-19.[20] Vaccine hesitancy and refusal have grown, and vaccination levels have reached a plateau in LMICs such as SA.[21] Given the low vaccine uptake in sub-Saharan Africa, the high prevalence of comorbidities and the limited capacity of the healthcare system, existing mitigation strategies must be supplemented by other evidence-based interventions to reduce the risk of severe disease. One supplemental strategy is treatment of COVID-19 with effective oral antiviral agents to reduce the overall burden of disease, curtail transmission and retard progression to severe disease.[22]
Several antivirals have been developed or repurposed to treat COVID-19 early after infection is established.[23] Remdesivir, nirmatrelvir/ritonavir and molnupiravir are cost-effective and have received either full approval or emergency use authorisation from regulatory authorities in most LMICs, and existing supply chain networks have been successfully established. In October 2021, Merck Sharp & Dohme (MSD) authorised a licence agreement with the Medicines Patent Pool (MPP) for molnupiravir that allowed 105 countries access to generic formulations of the antiviral for the treatment for mild to moderate COVID-19.[24] In November 2021, Pfizer authorised a licence agreement with the MPP to facilitate affordable access to nirmatrelvir/ritonavir. This allowed for access to generic antiviral products for the treatment of COVID-19 in 95 countries worldwide. The licensing agreements secured by MPP have enhanced global production, thus limiting supply shortages, and increased equitable access to therapeutics in LMICs, which in turn increases the global capacity to curb the transmission and progression of COVID-19, and therefore the morbidity and mortality.[25] In addition, licensing agreements allow for potential reduction in the cost of treatment, with generic formulations in LMICs and potential for exportation of generics from such countries to neighbouring countries. Other interventions include treatment with monoclonal antibodies, immunomodulating agents such as Janus kinase (JAK) inhibitors and convalescent plasma. While each intervention has shown sufficient levels of efficacy in the setting of high-income countries (HICs), limitations in LMICs such as costs, relevant regulatory body approval, supply chains, cold chain integrity and safety profile in a high HIV burden setting make these interventions difficult to implement. The implementation of oral antivirals for the treatment of COVID-19, however, may be the most pragmatic option in the LMIC setting.
Recent evidence also shows that in people with SARS-CoV-2 infection and at least one risk factor for progression to severe COVID-19, early treatment with antivirals (nirmatrelvir/ritonavir) during the acute phase of COVID-19 was associated with reduced risk (relative risk 0.74; 95% confidence interval (CI) 0.72 - 0.77) of post-COVID conditions (long COVID), including reduced risk of sequelae in the cardiovascular system (dysrhythmia and ischaemic heart disease), coagulation and haematological disorders (pulmonary embolism and deep vein thrombosis), fatigue and malaise, acute kidney disease, muscle pain, neurological system (neurocognitive impairment and dysautonomia) and shortness of breath.[26]
In support of a public health approach, therapeutic interventions in LMICs need to be designed for implementation at a nurse-driven, doctor-supported primary healthcare level, with minimal clinical monitoring and ease of administration being prioritised. Primary healthcare serves the majority of the population in LMICs and is easily available, accessible and affordable.[27] As a result, test-and-treat strategies should be aimed at this sector in order to be feasible, scalable, sustainable and have the greatest impact on the health of the population. A test-and-treat strategy to facilitate early administration of oral antivirals in a sub-saharan African setting could reduce hospitalisation and progression to severe illness, thus reducing the burden of COVID-19 on already resource-limited healthcare systems. The risk of progression from mild to critical disease is high in susceptible populations such as that of sub-Saharan Africa, where the healthcare system is ill-equipped to deal with such a burden, and the prevalence of comorbidities is high. Ideal interventions in this setting should be safe, effective, have a low potential for drug-drug interactions, be easy to administer and be economically and logistically feasible.
This review article provides information on presently available therapeutics for the treatment of mild/moderate COVID-19 as well as novel therapeutics in their developmental phases that could potentially be used to prevent the progression to severe disease in the sub-Saharan African setting.
Methods
We performed searches of Medline/PubMed, SCOPUS and the Cochrane Central Register of Controlled Trials from January 2020 to 31 March 2023. Publications in which the clinical evaluation of COVID-19 antiviral agents was reported were included. The search strategy included the following Medical Subject Heading (MeSH) terms in titles and abstracts: ('SARS-COV-2 OR 'coronavirus' OR 'COVID-19' OR 'COVID') AND ('antiviral' OR 'treatment' OR 'clinical trial' OR 'intervention'). Publications were limited to human studies in the English language. A review of all articles from the reference lists of identified articles was conducted to identify additional articles not found by the electronic search. We included all studies that described at least one antiviral agent, evaluated in at least one phase II, III or IV trial, and which reported clinical safety, efficacy outcomes, barriers to implementation, or enablers of implementation. Case reports, case series and review articles were excluded. We further restricted the search to oral antiviral agents with authorisation for use in at least one jurisdiction for use in the treatment of mild or moderate COVID-19. Studies that described the use of antiviral agents for prophylaxis only were excluded, while studies describing the effects of antiviral agents for COVID-19 on healthcare systems and infrastructure were included. In addition to published articles, COVID-19 treatment guidelines published by the World Health Organization (WHO), National Institutes of Health (NIH) and Centers for Disease Control and Prevention were also reviewed, as well as national government documents and policies.
Discussion
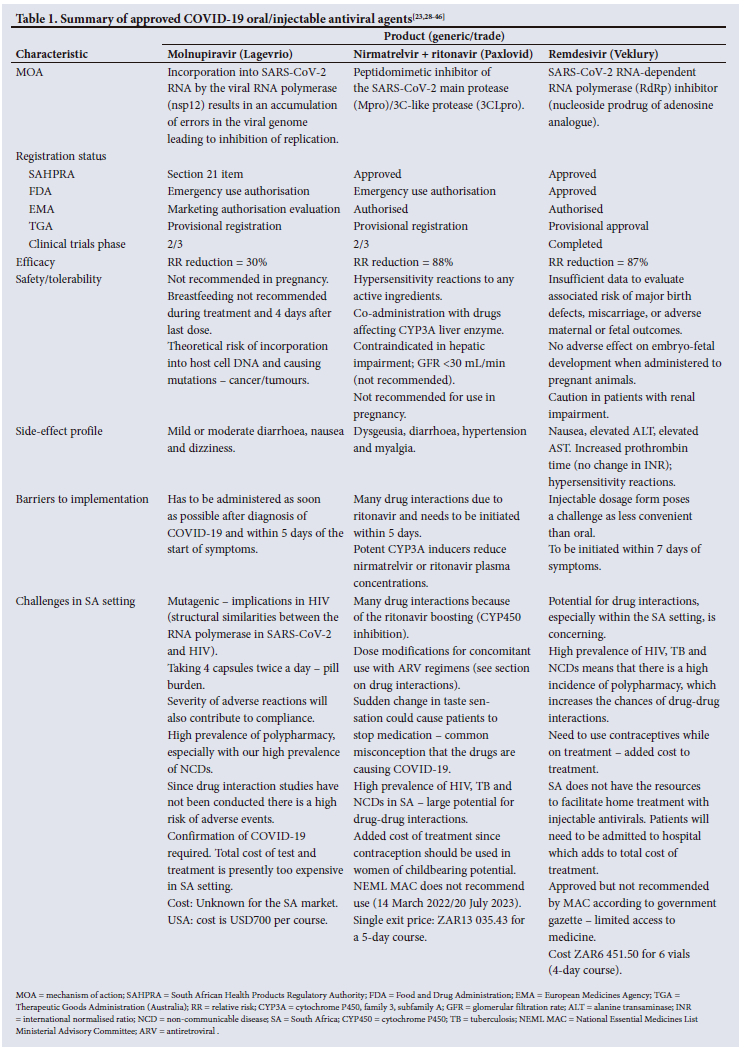
There are three antiviral agents that are available for use in SA (Table 1).[23,28-46] Currently registered antivirals for the treatment of COVID-19 include ritonavir-boosted nirmatrelvir (Paxlovid), molnupiravir (Lagevrio) and remdesivir (Veklury). While remdesivir has received full approval by the US Food and Drug Administration (FDA), ritonavir-boosted nirmatrelvir and molnupiravir have received emergency use authorisation (EUA).[28-32] Clinical investigations of ritonavir-boosted nirmatrelvir demonstrated a relative risk reduction in progression to severe disease of 89.1% in high-risk individuals.[33] Similar investigations show that molnupiravir is associated with a 30% reduction in COVID-19 hospitalisation or death in high-risk individuals.[34] In addition, a large-scale, real-world, retrospective cohort study during the Omicron (B.1.1.529) subvariant BA.2.2 wave demonstrated an overall reduction in mortality of 24% with molnuprinavir and 66% with ritonavir-boosted nirmatrelvir.[35-37] A SA cohort study investigating effectiveness of nirmatrelvir/ritonavir reported 79.6% effectiveness in preventing hospital admission or death within 30 days of a positive test if the patient received treatment 0 - 5 days after symptom onset. The effectiveness of treatment on patients who received the course on the day of their test was 89.6%. Effectiveness of treatment was 43.8% in patients who received the treatment >6 days after the onset of symptoms.[38] PANORAMIC, an open-label, platform-adaptive randomised controlled trial comparing the use of molnupiravir plus usual care v. usual care alone as early treatment for COVID-19 in high-risk adults reported that early addition of molnupiravir to usual care did not reduce hospitalisation or death. However, participants who received molnupiravir plus usual care recovered faster than those receiving only usual care, had a higher rate of early sustained recovery and had fewer general practitioner consultations.[39] A study published in February 2023 assessing the effectiveness of molnupiravir and nirmatrelvir/ritonavir in reducing hospitalisation and death in a real-world cohort of non-hospitalised patients reported that the use of either drug was not associated with lower risk of ICU admission, invasive mechanical ventilation and/or death as compared with patients who did not receive antivirals.[40] The use of nirmatrelvir/ritonavir, but not molnupiravir, was associated with a reduced risk of hospitalisation.[40] In addition, although nirmatrelvir/ ritonavir use improves outcomes in high-risk patients aged >65 years, data in younger (between 50 and 64 years old) vaccinated patients are inconsistent.[41-44] While molnupiravir is a known mutagenic agent, a recent concern about the mechanism by which it works has been expressed, with the drug causing mutations that have been associated with onwards transmission.[45,46]
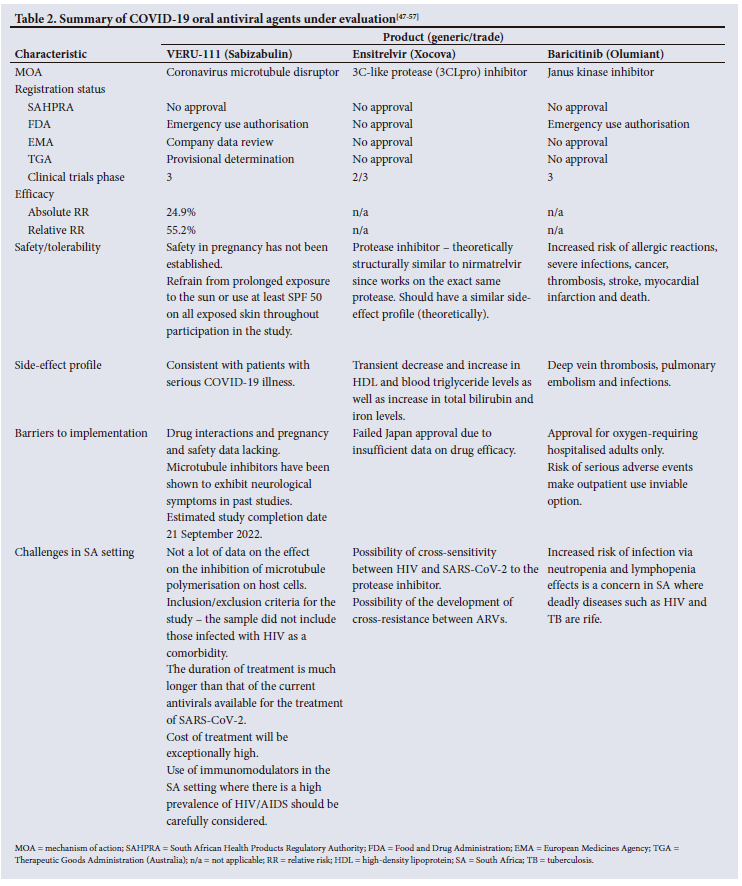
Several oral antivirals are currently under evaluation by relevant regulatory bodies and show promise as antivirals for the treatment of COVID-19 (Table 2).1[47-57] Sabizabulin (VERU-111), a coronavirus microtubule disruptor, and baricitinib, a JAK inhibitor, have both received EUA by the FDA, while ensitrelvir, a C3-like protease inhibitor, is still under investigation. A phase III clinical trial assessing the benefit of oral sabizabulin in hospitalised adults with COVID-19 on supplemental oxygen reported a 55.2% relative reduction in mortality compared with placebo.[47] The COV-BARRIER study, a randomised, double-blind, placebo-controlled phase III trial assessing the efficacy and safety of baricitinib for the treatment of hospitalised adults with COVID-19, reported a 38.2% reduction in 28-day all-cause mortality compared with placebo.[48] A recent study also reported that ensitrelvir demonstrates strong in vitro antiviral activity against SARS-CoV-2 Omicron subvariants BA.4 and BA.5.[49]
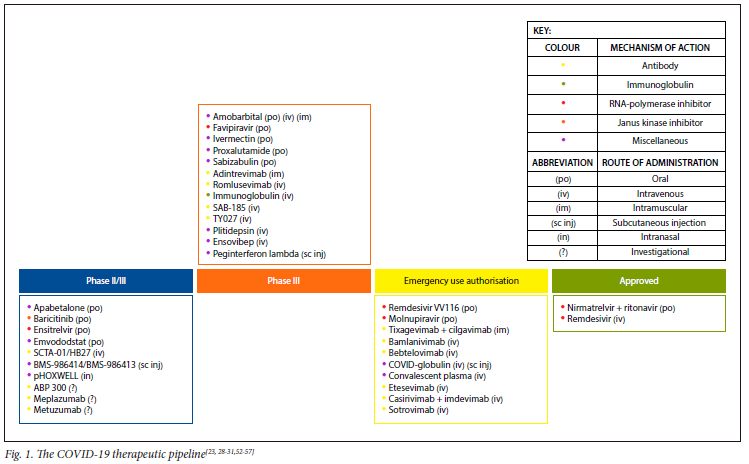
Fig. 1 presents a pipeline of treatments for COVID-19 in different phases of clinical trials and regulatory evaluation.[23, 28-31,52-57] Classes of drugs shown in the diagram include monoclonal antibodies, immunoglobulins, antivirals and JAK inhibitors, each with its corresponding route of administration, i.e. oral, intravenous, intramuscular, subcutaneous or intranasal. In the global fight against COVID-19, access initiatives such as the WHO's Access to COVID-19 Tools Accelerator (ACT-A) and the Global Accountability Platform to fight COVID-19 (COVID GAP) led by Duke University have been established to build global relationships to accelerate the end of the pandemic.[20,51] These initiatives focus on improving access to resources in settings where healthcare systems are ill-equipped to manage a high burden of severe disease. In addition to facilitating access to resources such as vaccines, the ACT-A strategic plan and COVID GAP outline strategies to improve testing capacity and enhance access to effective antiviral therapy to reduce the progression of disease and the overall burden of severe disease.
One initiative, the COVID Treatment Quick Start Consortium, a collaboration between Duke University, the Clinton Health Access Initiative (CHAI), COVID Collaborative and Americares, aims to support governments to increase access to novel COVID-19 antivirals in high-risk populations. It is one of the first initiatives to bring COVID-19 antivirals to low- and middle-income partner countries, including Ghana, Kenya, Laos, Malawi, Nigeria, Rwanda, SA, Uganda, Zambia and Zimbabwe.[58]
As of December 2022, Zambia became the first LMIC to receive a shipment of 1 000 courses of nirmatrelvir-ritonavir (Paxlovid), which is now available to patients for the treatment of mild-to-moderate COVID-19 in the implementation of a test-and-treat initiative in a vulnerable population.[59]
Various guidelines and policies for the treatment of mild to moderate COVID-19 have been implemented on a global scale. However, in the sub-Saharan African setting there have been many barriers to their implementation. The WHO's 'Therapeutics and COVID-19 Living Guidelines' as well as the NIH's 'Guidelines on Mild to Moderate COVID' are two examples of up-to-date scientific guides that recommend the use of novel oral antivirals for the treatment of mild to moderate COVID-19, including nirmatrelvir/ ritonavir (Paxlovid), remdesivir and molnupiravir.[60,61]
Test-and-treat strategy
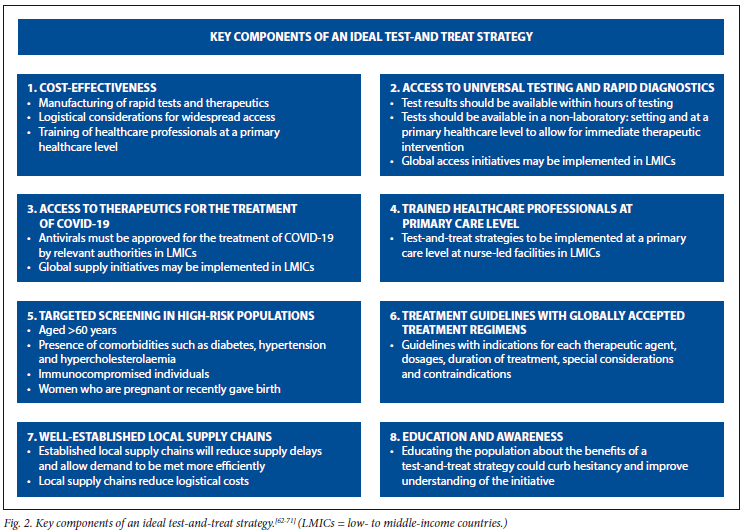
With limitations to the current mitigation strategies to reduce COVID-19 morbidity and mortality in LMICs, the implementation of a test-and-treat strategy could play a key role in reducing transmission and progression of the disease (Fig. 2). Although there is a current lack of control trial data on the efficacy of a test-and-treat strategy for COVID-19, the approach itself has shown to be effective in other illnesses such as HIV and malaria (in endemic areas). Universal test-and-treat trials (UTT) conducted in LMICs such as sub-Saharan Africa demonstrated significantly improved population-level viral suppression and decreased HIV incidence and mortality associated with this strategy.[62,63] A model-based study estimating the potential need and impact of test-and-treat programmes in LMICs predicted a significant reduction in severe cases of COVID-19 and COVID-19-related deaths, provided testing rates are high enough to facilitate a test-and-treat programme.[64] A modelling study carried out in Wallis and Futuna suggested that a test-and-treat strategy may contribute to the mitigation of COVID-19 epidemic resurgences, particularly in populations with low immunity and high levels of comorbidities. '651 Furthermore, there is strong support for a test-and-treat strategy aimed at reducing progression to severe COVID-19 in children and elderly patients.[66] Home testing coupled with patient self-sampling may enhance testing the population using local regulator-approved test kits.[67] Delivery of therapeutics, including oral antivirals, to patients' homes may be a viable option that could be explored to improve access to treatment. The need for therapeutic trials in the outpatient setting of LMICs remains, and the high costs associated with these trials is a potential hurdle to the rollout of a test-and-treat programme.[66] However, implementation studies may succeed in filling this gap and offer an opportunity to nest ancillary research, including much-needed drug interaction studies among tuberculosis (TB)/HIV co-infected individuals and patients on statin therapy, and offers opportunities to assess the feasibility of COVID-19 home testing as examples of future research opportunities.
Studies assessing point-of-care testing in HICs, such as that for group A streptococcus in Wales, have shown not only clinical but cost-saving benefits as well.[68] A confirmed diagnosis before initiating treatment prevents overdispensing of medication and unnecessary prescribing of drugs. HICs such as the USA and the UK have proceeded to implement test-and-treat strategies for the management of COVID-19, despite the lack of clinical trial evidence. The implementation of a test-and-treat strategy in some HICs, such as New Zealand, allowed increased involvement of pharmacists in the prescribing and dispensing of antivirals for the treatment of COVID-19.[69] This allowed for increased access to the antivirals while requiring little to no additional training of healthcare workers. The importance of the pharmacy profession in test-and-treat initiatives should be considered. Local pharmacy clinics are ideal sites for administration of antivirals. The ideal test-and-treat strategy should include a multidisciplinary approach involving the healthcare professionals who are at community level (e.g. nurses, pharmacists, community healthcare workers, traditional healers) for greater access, convenience and coverage.[70]
The novel COVID-19 antivirals discussed in this review offer a promising approach in the treatment of mild to moderate COVID-19 when implemented as part of a test-and-treat strategy. Since these therapeutics must be initiated within 5 days of onset of symptoms, treatment must be closely linked to testing to reduce the burden of disease in a sub-Saharan African setting.[71] This implies a need for an increase in diagnostic capacity of healthcare systems in LMICs as well as increased access to oral antivirals, both of which may be accomplished by the intervention of previously mentioned global initiatives. Manufacturing of generic antiviral products has been slowed by regulatory processes and the need for high-quality bioequivalence data; therefore, access to effective biosimilars (biotherapeutics that have a high level of similarity to an already-approved 'reference' product) remains limited in most LMICs.[72,73]
Barriers and potential solutions for implementation
Access challenges
There is a limited supply of therapeutics, and although there are many global initiatives to provide access for LMICs to these drugs, HICs and high- to middle-income countries (HMICs) are often first to act. LMICs need to estimate their need for therapeutics prior to purchase to prevent misuse of resources. In the same way, sponsors, funders and other global initiatives require these estimates in order to purchase therapeutics on behalf of low-income countries (LICs) and LMICs to ensure supply on the basis of need in the face of global supply constraints. Forecasting the needs of LICs and LMICs depend on many variables, including testing capacity, capacity to get the therapeutics to the patients and hesitancy or lack of trust in the therapeutics.[20]
In order to overcome accessibility and supply barriers, countries in need of assistance in procuring and distributing these antivirals must work together with organisations and other countries in access initiatives such as ACT-A and COVID GAP. Pooled procurement of COVID-19 therapeutics to build treatment capacity is a strategy that can be utilised.[74] In addition to initiatives such as the COVID Treatment Quick Start Consortium, which is increasing access to COVID-19 antivirals to execute a test-and-treat approach, policy and guidelines on mobilisation and decentralisation of testing facilities must be developed.[75]
Global funding initiatives have been developed to ensure that countries in need are offered financial support for the procurement of COVID-19 tools including vaccines, treatment and test kits.[20,51,76] Reluctance to vaccinate or comply with treatment can be addressed with widespread education programmes that increase understanding and awareness of the test-and-treat strategy. Evidence-based communication strategies are key in reducing misunderstanding and promoting compliance.[77]
Local manufacturing of COVID-19 antivirals could also help to reduce cost and increase availability in a sub-Saharan African setting. Voluntary licences may be granted to generic manufacturers either directly from parent companies or via the MPP in order to increase production.[71]
Testing capacity
Oral antivirals for the treatment of COVID-19 need to be initiated within 5 days of symptom onset in patients with a confirmed diagnosis.[78] Access to rapid antigen tests in LMICs is limited compared with HICs, where at-home testing is easily accessible to confirm a diagnosis and initiate treatment. In many LMICs, testing facilities are inconveniently located, with many individuals having to travel long distances to clinics or hospitals. An assessment carried out in October 2021 by the WHO reported that only one in seven COVID-19 infections (14.2%) were being detected in Africa.[79] The implications of limited testing capacity include a greater burden of disease than estimated and inadequate clinical care of undiagnosed cases, leading to progression of disease.[80] An adequate testing capacity is one of the key components to a successful test-and-treat strategy, and initiatives such as ACT-A, CHAI and COVID GAP have facilitated an increased supply of tests to LMICs to be implemented at a primary healthcare level.
Capacity of the healthcare system
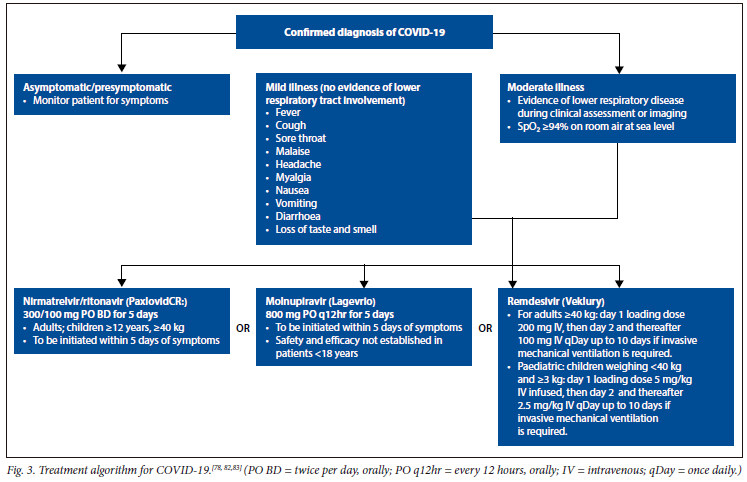
In many LICs and LMICs, such as those in sub-Saharan Africa, healthcare systems do not have the capacity to test patients timeously and simultaneously deliver therapeutics for the initiation of treatment. A large majority of cases go undetected, and since treatment must be closely linked to testing, this poses a great barrier in the global fight against COVID-19.[71] The test-and-treat strategy has been successful in HICs as a result of mobilisation of testing facilities as well as the supply of therapeutics on the basis of need. Healthcare workers need to be trained on how to test and treat effectively, and the population at large needs to be educated on how to use a home test kit. In addition, an authorised prescriber is needed in order to prescribe therapeutics following a positive COVID-19 diagnosis in mild/moderate disease, and patients need to be made aware of possible adverse reactions and to report to a healthcare facility should they experience such effects.[81] This is particularly important in a sub-Saharan African setting where the potential for drug-drug interactions is high owing to high rates of comorbidities. A proposed algorithm for a test-and-treat strategy is presented in Fig. 3.[78,82,83]
Literacy level of the population
Literacy, particularly COVID-19 health literacy, is a major driver of adherence to treatment as well as willingness to be treated.[84] The low literacy level of LMIC populations is expected to contribute to a higher reluctance to be treated with oral antivirals. In sub-Saharan Africa, the literacy levels are significantly lower than those in HICs, and so, although the population may benefit from treatment, many may opt not to take it. The lack of trust in therapeutics, however, is something that can be addressed with increased education and awareness, as seen from previous implementation of test-and-treat strategies for HIV in LMICs. Prescriber hesitancy, as seen in the early stages of vaccination rollouts worldwide, may be an additional hindrance to the success of a test-and-treat strategy in LMICs.[85]
Licensing issues
Access challenges result from limited production capacity due to delayed submission by licence holders following regulatory approval.[20] In addition, not all oral antivirals for the treatment of COVID-19 are registered in LMICs, presenting a major barrier to the implementation of treatment guidelines for mild/moderate COVID-19.[20] The United Nations-backed public health organisation, the MPP, is one organisation that aims to address these access challenges by signing agreements with patent holders to increase production and distribution of oral antivirals for the treatment of COVID-19 and COVID-19 technologies.[86] Voluntary licensing and patent pooling allow for LMICs to have rapid access to testing and treatment, thus making it not only possible but feasible to implement a test-and-treat strategy for COVID-19. The SA Health Products Regulatory Authority (SAHPRA) approved remdesivir and nirmatrelvir/ritonavir for the treatment of COVID-19, while molnupiravir was authorised as a section 21 item (to be prescribed on a patient-to-patient basis).
Risk of drug-drug interactions
According to Statistics SA, ~8.45 million people are living with HIV as of 2022 (mid-year statistics) in SA (13.9% of the total population).[87] According to the Joint United Nations Programme on HIV and AIDS (UNAIDS), ~74% of people living with HIV are on antiretroviral (ARV) therapy, and ~67% are virally supressed.[88] Paxlovid has the potential for drug-drug interactions with many therapeutics, including ARVs and drugs used to treat TB. In a population where HIV and TB are so prevalent, the effects of these potential drug-drug interactions on an individual's quality of life are currently unknown, and adverse drug events could result in poor compliance and treatment interruption, contributing to increased HIV and TB morbidity and mortality. However, the short treatment duration of most antivirals for COVID-19 provides some mitigation against this risk, and there are no known interactions expected between the current SA first-line ART, tenofovir/lamivudine/ dolutegravir (TLD) and Paxlovid, while there is potential for interactions with second-line protease inhibitor-based regimens. For healthcare workers prescribing COVID-19 antivirals, the University of Liverpool COVID-19 drug interaction tracker is a valuable tool to guide clinical practice (https://www.covid19-druginteractions.org/checker).
Conclusion
This review sought to identify therapeutics that are effective at reducing progression of mild or moderate COVID-19 to severe disease, and to consider a test-and-treat approach that could be implemented in LMICs. In the SA setting, remdesivir, nirmatrelvir-ritonavir (Paxlovid) and molnupiravir are promising therapeutic agents. Other therapeutic agents, such as biologics and JAK inhibitors, remain in the therapeutic pipeline, but will likely be of limited use owing to their high cost and parenteral routes of administration. In a population where the prevalence of comorbidities such as hypertension, diabetes, hypercholesterolaemia, HIV and TB are high, strategies to reduce the burden of severe COVID-19 must be pursued to limit morbidity and mortality. Notwithstanding the significant challenges highlighted in this review, initiating a test-and-treat strategy with point-of-care testing and immediate administration of approved oral antivirals for the treatment of COVID-19 in high-risk patients may be a highly effective strategy in LMICs.
Declaration. None.
Acknowledgements. None.
Author contributions. RP and TNG conceptualised the manuscript and supervised all aspects of the review. VN and SG performed the literature search and produced the first draft. All others contributed to writing, reviewing and finalising the manuscript.
Funding. None.
Conflicts of interest. None.
References
1. World Health Organization. WHO Coronavirus Dashboard. Geneva: WHO, 2023. https://covid10.who.int2023 (accessed 31 March 2023). [ Links ]
2. Kong JD, Tekwa EW, Gignoux-Wolfsohn SA. Social, economic, and environmental factors influencing the basic reproduction number of COVID-19 across countries. PLoS ONE 2021;16(6):e0252373. https://doi.org/10.1371/journal.pone.0252373 [ Links ]
3. World Health Organization. WHO coronavirus dashboard table view situation by region, country, territory and area. Geneva: WHO, 2023. [ Links ]
4. World Health Organization. WHO Coronavirus Dashboard. Geneva: WHO, 2022. https://covid19.who.int/ (accessed 20 November 2022). [ Links ]
5. Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: Summary of a report of 72 314 cases from the Chinese Centers for Disease Control and Prevention. JAMA 2020;323(13):1239-1242. https://doi.org/10.1001/jama.2020.2648 [ Links ]
6. Esper FP, Adhikari TM, Tu ZJ, et al. Alpha to Omicron: Disease severity and clinical outcomes of major SARS-CoV-2 variants. J Infect Dis 2023;227(3):344-352. https://doi.org/10.1093/infdis/jiac411 [ Links ]
7. Jassat W, Karim SSA, Mudara C, et al. Clinical severity of COVID-19 in patients admitted to hospital during the omicron wave in South Africa: A retrospective observational study. Lancet Glob Health 2022;10(7):e961-e969. https://doi.org/10.1016/S2214-109X(22)00114-0 [ Links ]
8. Madhi SA, Nel J. Epidemiology of severe COVID-19 from South Africa. Lancet HIV 2021;8(9):e524-e526. https://doi.org/10.1016/S2352-3018(21)00183-1. [ Links ]
9. Cabore JW, Karamagi HC, Kipruto HK, et al. COVID-19 in the 47 countries ofthe WHO African region: A modelling analysis of past trends and future patterns. Lancet Glob Health 2022;10(8):e1099-e1114. https://doi.org/10.1016/S2214-109X(22)00233-9 [ Links ]
10. Vassall A, Sweeney S, Kahn J, et al. Reference case for estimating the costs of global health services and interventions. Global Health Cost Consortium, 2017. https://ghcosting.org/pages/standards/reference_case (accessed 15 May 2023). [ Links ]
11. Edoka I, Fraser H, Jamieson L, Meyer-Rath G, Mdewa W. Inpatient care costs of COVID-19 in South Africa's public healthcare system. Int J Health Policy Manage 2022;11(8):1354-1361. https://doi.org/10.34172/ijhpm.2021.24 [ Links ]
12. Our World in Data. Number of COVID-19 patients in hospital. Our World in Data, 2022. https://ourworldindata.org/grapher/current-covid-patients-hospital?tab=table&country=~ZAF (accessed 11 October 2022). [ Links ]
13. Our World in Data. Current number of COVID-19 Patients in ICU. Our World in Data, 2022. https://ourworldindata.org/grapher/current-covid-patients-icu?tab=tabl (accessed 11 October 2022). [ Links ]
14. National Institiute for Communicable Diseases. Daily Hospital Surveillance (DATCOV) Report. Pretoria: NICD, 2022. [ Links ]
15. Pereznieto P, Oehler I. Social costs of the COVID-19 pandemic 2021. https://theindependentpanel.org/wp-content/uploads/2021/05/Background-paper-9-Social-impact.pdf (accessed 15 May 2023). [ Links ]
16. Saladino V, Algeri D, Auriemma V The psychological and social impact of COVID-19: New perspectives of well-being. Front Psychol 2020;11:577684. [ Links ]
17. Madhi SA. Why it is time for the national coronavirus command council to go. Business Live, 2023. https://www.businesslive.co.za/bd/opinion/2022-02-03-shabir-a-madhi-why-it-is-time-for-the-national-coronavirus-command-council-to-go/ (accessed 15 May 2023). [ Links ]
18. Lancet. Access to COVID-19 vaccines: Looking beyond COVAX. Lancet 2021;397(10278):941. https://doi.org/10.1016/S0140-6736(21)00617-6 [ Links ]
19. COVID-19 vaccine may be less effective in some people with cancer. Cancer, 2021. https://www.cancer.gov/news-events/cancer-currents-blog/2021/covid-vaccine-limited-protection-in-cancer-patients (accessed 18 May 2023). [ Links ]
20. Boyer B, Chupp E, Edson G, et al. Pills to people: Accelerating equitable global access to oral therapeutics for COVID-19. Covid Gap, 2022. https://covid19gap.org/insights/pills-to-people-accelerating-equitable-global-access-to-oral-therapeutics-for-covid-19 (accessed 18 May 2023). [ Links ]
21. Cooper S, van Rooyen H, Wiysonge CS. COVID-19 vaccine hesitancy in South Africa: How can we maximise uptake of COVID-19 vaccines? Expert Rev Vacc 2021;20(8):921-933. https://doi.org/10.1080/14760584.2021.1949291 [ Links ]
22. World Health Organization. COVID-19 vaccination roll-out stagnates in Africa 2022. Geneva: WHO, 2022. https://www.afro.who.int/news/covid-19-vaccination-roll-out-stagnates-africa (accessed 25 May 2023). [ Links ]
23. Biotechnology Innovation Organisation. BIO COVID-19 Therapeutic Development Tracker. New York: BIO, 2022. [ Links ]
24. World Health Organization. License agreements for COVID-19 therapeutics. Geneva: WHO, 2022. [ Links ]
25. Shadlen KC. Accelerating pooled licensing of medicines to enhance global production and equitable access. Lancet 2022;400(10352):632-634. https://doi.org/10.1016/S0140-6736(22)01013-3 [ Links ]
26. Xie Y, Choi T, Al-Aly Z. Association of treatment with nirmatrelvir and the risk of post-COVID-19 condition. JAMA Intern Med 2023;183(6):554-564. https://doi.org/10.1001/jamainternmed.2023.0743 [ Links ]
27. World Health Organization. Primary health care systems: Case study from South Africa. Geneva: WHO, 2017. [ Links ]
28. Pfizer. Fact sheet for healthcare providers: Emergency use authorisation for Paxlovid. New York: Pfizer, 2022. [ Links ]
29. Pfizer. Fact sheet for patients, parents, and caregivers: Emergency user authorisation (EUA) of Paxlovid for coronavirus disease 2019 (COVID-19). New York: Pfizer, 2022. [ Links ]
30. Pfizer. Pfizer receives US FDA emergency use authorisation for novel COVID-19 oral antiviral treatment. New York: Pfizer, 2021. https://www.pfizer.com/news/press-release/press-release-detail/pfizer-receives-us-fda-emergency-use-authorisation-novel (accessed 23 May 2023). [ Links ]
31. European Medicines Agency. EMA issues advice on use of Lagevrio (molnupiravir) for the treatment of COVID-19 2021. https://www.ema.europa.eu/en/news/ema-issues-advice-use-lagevrio-molnupiravir-treatment-covid-19 (accessed 20 May 2023). [ Links ]
32. Food and Drug Administration. Lagevrio (Molnupiravir) HCP FS 02012023. FDA, 2021. [ Links ]
33. Hammond J, Leister-Tebbe H, Gardner A, et al. Oral nirmatrelvir for high-risk, nonhospitalised adults with COVID-19. N Engl J Med 2022;386(15):1397-1408. https://doi.org/10.1056/NEJMoa2118542 [ Links ]
34. Merck. Merck and Ridgeback Biotherapeutics provide update on results from MOVE-OUT study of molnupiravir, an investigational oral antiviral medicine, in at risk adults with mild-to-moderate COVID-19. Merck, 2021. https://www.merck.com/news/merck-and-ridgeback-biotherapeutics-provide-update-on-results-from-move-out-study-of-molnupiravir-an-investigational-oral-antiviral-medicine-in-at-risk-adults-with-mild-to-moderate-covid-19/ (accessed 25 May 2023). [ Links ]
35. Burdet C, Ader F. Real-world effectiveness of oral antivirals for COVID-19. Lancet 2022;400(10359):1175-1176. https://doi.org/10.1093/infdis/jiad324 [ Links ]
36. Wong CKH, Au ICH, Lau KTK, Lau EHY, Cowling BJ, Leung GM. Real-world effectiveness of molnupiravir and nirmatrelvir plus ritonavir against mortality, hospitalisation, and in-hospital outcomes among community-dwelling, ambulatory patients with confirmed SARS-CoV-2 infection during the omicron wave in Hong Kong: An observational study. Lancet 2022;400(10359):1213-1222. https://doi.org/10.1016/S0140-6736(22)01586-0 [ Links ]
37. Saravolatz LD, Depcinski S, Sharma M. Molnupiravir and nirmatrelvir-ritonavir: Oral coronavirus disease 2019 antiviral drugs. Clin Infect Dis 2022;76(1):165-171. https://doi.org10.1093/cid/ciac180 [ Links ]
38. Lewnard JA, McLaughlin JM, Malden D, et al. Effectiveness of nirmatrelvir-ritonavir against hospital admission or death: A cohort study in a large US healthcare system. medRxiv 2023:2022.10.02.22280623 [ Links ]
39. Butler CC, Hobbs FDR, Gbinigie OA, et al. Molnupiravir plus usual care versus usual care alone as early treatment for adults with COVID-19 at increased risk of adverse outcomes (PANORAMIC): An open-label, platform-adaptive randomised controlled trial. Lancet 2023;401(10373):281-293. https://doi.org10.1016/S0140-6736(22)02597-1 [ Links ]
40. Yip TC, Lui GC, Lai MS, et al. Impact of the use of oral antiviral agents on the risk of hospitalisation in community coronavirus disease 2019 patients (COVID-19). Clin Infect Dis 2023;76(3):e26-e33. https://doi.org10.1093/cid/ciac687 [ Links ]
41. Ebell MH. Nirmatrelvir/ritonavir reduces hospitalisation, mortality in patients 65 years and older with COVID-19; effect on younger patients unclear. Am Fam Physician 2023;107(3):316. [ Links ]
42. Cheema HA, Jafar U, Sohail A, et al. Nirmatrelvir-ritonavir for the treatment of COVID-19 patients: A systematic review and meta-analysis. J Med Virol 2023;95(2):e28471. https://doi.org10.1002/jmv.28471 [ Links ]
43. Reis S, Metzendorf MI, Kuehn R, et al. Nirmatrelvir combined with ritonavir for preventing and treating COVID-19. Cochrane Database Syst Rev 2022;9(9):Cd015395. https://doi.org/10.1002/14651858.cd015395.pub2 [ Links ]
44. Arbel R, Wolff Sagy Y, Hoshen M, et al. Nirmatrelvir use and severe covid-19 outcomes during the omicron surge. N Engl J Med 2022;387(9):790-798. https://doi.org/10.1056/nejmoa2204919 [ Links ]
45. Sanderson T, Hisner R, Donovan-Banfield I, Peacock T, Ruis C. Identification of a molnupiravir-associated mutational signature in SARS-CoV-2 sequencing databases. medRxiv 2023:2023.01.26.23284998. https://doi.org10.1056/NEJMoa2204919 [ Links ]
46. National Institute for Communicable Diseases. SARS-COV-2 genomic surveillance update. Johannesburg: NICD, 2023. [ Links ]
47. Gonzales TL, Skarda P, Bird TG, et al. LB1530. Clinical benefit of oral sabisabulin for hospitalised adults with COVID-19 on supplemental oxygen. Open Forum Infect Dis 2022;9(Suppl2):ofac492.1876 https://doi.org10.1093/ofid/ofac492.1876 [ Links ]
48. Marconi VC, Ramanan AV, de Bono S, et al. Efficacy and safety of baricitinib for the treatment of hospitalised adults with COVID-19 (COV-BARRIER): A randomised, double-blind, parallel-group, placebo-controlled phase 3 trial. Lancet Respir Med 2021;9(12):1407-1418. https://doi.org10.1016/S2213-2600(21)00331-3 [ Links ]
49. McCarthy MW. Ensitrelvir as a potential treatment for COVID-19. Expert Opin Pharmacother 2022;23(18):1995-1998. https://doi.org10.1080/14656566.2022.2146493 [ Links ]
50. Cao Z, Gao W, Bao H, et al. VV116 versus nirmatrelvir-ritonavir for oral treatment of COVID-19. N Engl J Med 2023;388(5):406-417. https://doi.org10.1056/NEJMoa2208822 [ Links ]
51. World Health Organization. Access to COVID-19 tools accelerator strategic plan and budget. Geneva: WHO, 2022. [ Links ]
52. European Medicines Agency. EMA reviewing data on sabisabulin for COVID-19. EMA, 2022. https://www.ema.europa.eu/en/news/ema-reviewing-data-sabisabulin-covid-19 (accessed 25 May 2023). [ Links ]
53. Gilead Sciences. Highlights of prescribing information: Veklury, 2022. https://www.gilead.com/-/media/files/pdfs/medicines/covid-19/veklury/veklury_pi.pdf (accessed 20 May 2023). [ Links ]
54. Verupharma. Biopharmaceutical company focused on COVID-19 and oncology. Very Corporate, 2022. https://verupharma.com/wp-content/uploads/2022/05/Veru-Corporate-Presentation-May-2022.pdf (accessed 25 May 2023). [ Links ]
55. Barnette KG, Gordon MS, Rodriguez D, et al. Oral sabizabulin for high-risk, hospitalised adults with COVID-19: Interim analysis. N Engl J Med Evidence 2022;1(9):220145. https://doi.org10.1056/EVIDoa2200145 [ Links ]
56. Hauteng Pharma. Ensitrelvir, an oral antiviral drug for COVID-19 treatment. Hauteng Pharma, 2022. https://www.molecularcloud.org/p/ensitrelvir-an-oral-antiviral-drug-for-covid-19-treatment (accessed 23 May 2023). [ Links ]
57. Mukaea H, Yotsuyanagi H, Ohmagaric N, et al. A randomised phase 2/3 study of ensitrelvir, a novel oral SARS-CoV-2 3C-like protease 3 inhibitor, in Japanese patients with mild-to-moderate COVID-19 or asymptomatic SARS-CoV-2 infection: Results of the phase 2a part. Antimicrob Agents Chemother 2022;66(10):e0069722. https://doi.org10.1128/aac.00697-222022 [ Links ]
58. The COVID Treatment Quick Start Consortium. Duke University, 2022. https://www.covidcollaborative.us/initiatives/quickstart-consortium#:~:text=What%20is%20COVID%20Treatment%20Quick,Hilton%20Foundation (accessed 25 May 2023). [ Links ]
59. Quick Start Consortium. Zambia Becomes First Country to Receive PAXLOVID through COVID Treatment Quick Start Consortium. Quick Start Consortium, 2022. https://dukeghic.org/wp-content/uploads/sites/20/2022/12/Paxlovid_PR_22-Dec-2022_Zambia.pdf (accessed 23 May 2023). [ Links ]
60. National Institutes of Health. Coronavirus disease 2019 (COVID-19) treatment guidelines. New York: NIH, 2022. [ Links ]
61. World Health Organization. Therapeutics and COVID-19: Living guidelines. Geneva: WHO, 2022. [ Links ]
62. Girum T, Yasin F, Wasie A, Shumbej T, Bekele F, Zeleke B. The effect of 'universal test and treat' program on HIV treatment outcomes and patient survival among a cohort of adults taking antiretroviral treatment (ART) in low income settings of Gurage zone, South Ethiopia. AIDS Research and Therapy 2020;17(1):19. https://doi.org10.1186/s12981-020-00274-3 [ Links ]
63. Havlir D, Lockman S, Ayles H, Larmarange J, Chamie G, Gaolathe T, et al. What do the Universal Test and Treat trials tell us about the path to HIV epidemic control? J Int AIDS Soc 2020;23(2):e25455. https://doi.org10.1002/jia2.25455 [ Links ]
64. Han AX, Hannay E, Carmona S, et al. Estimating the potential need and impact of SARS-CoV-2 test-and-treat programs with oral antivirals in low-and-middle-income countries. medRxiv 2022;13:2022.10.05.22280727. https://doi.org10.1101/2022.10.05.22280727 [ Links ]
65. Brault A, Tran-Kiem C, Couteaux C, et al. Modelling the end of a Zero-COVID strategy using nirmatrelvir/ritonavir, vaccination and NPIs in Wallis and Futuna. Lancet Reg Health West Pac 2023;30:100634. https://doi.org10.1016/j.lanwpc.2022.100634 [ Links ]
66. Schiffer JT, Johnston C, Wald A, Corey L. An early test-and-treat strategy for severe acute respiratory syndrome coronavirus 2. Open For Infect Dis 2020(7):ofaa232. https://doi.org/10.1093/ofid/ofaa232 [ Links ]
67. South African Health Products Regulatory Authority. SAHPRA approves antigen self-test kits for public use. Cape Town: SAHPRA, 2022. [ Links ]
68. Mantzourani E, Cannings-John R, Evans A, Ahmed H. To swab or not to swab? Using point-of-care tests to detect Group A Streptococcus infections as part of a Sore Throat Test and Treat service in community pharmacy. J Antimicrobial Chemo 2022;77(3):803-806. https://doi.org/10.1093/jac/dkab470 [ Links ]
69. Smith DJ, McGill L, Carranza D, Adeyemo A, Hakim AJ. Global engagement of pharmacists in test and treat initiatives: Bringing care from clinics to communities. J Am Pharm Assoc 2023;63(1):419-423. https://doi.org/10.1016/j.japh.2022.10.013 [ Links ]
70. Gentles A. COVID-19 test-and-treat strategy: A precedent-setting opportunity for us as societal leaders. J Am Pharmacists Assoc 2023;63(1):416-418. https://doi.org/10.1016/j.japh.2022.11.008 [ Links ]
71. Wroe EB, Seung KJ, Baker BK, Farmer PE. Test and treat: A missing link in the global fight against COVID-19. Lancet Glob Health 2022;10(2):e181-e182. https://doi.org/10.1016/S2214-109X(21)00568-4 [ Links ]
72. Gherghescu I, Delgado-Charro MB. The biosimilar landscape: An overview of regulatory approvals by the EMA and FDA. Pharmaceutics 2020;13(1):48. https://doi.org/10.3390/pharmaceutics13010048 [ Links ]
73. Pepperrell T, Ellis L, Wang J, Hill A. Barriers to worldwide access for Paxlovid, a new treatment for COVID-19. Open For Infect Dis 2022;9(9):ofac174. https://doi.org/10.1093/ofid/ofac174 [ Links ]
74. Bright B, Babalola CP, Sam-Agudu NA, et al. COVID-19 preparedness: Capacity to manufacture vaccines, therapeutics and diagnostics in sub-Saharan Africa. Globalis Health 2021;17(1):24. https://doi.org/10.1186/s12992-021-00668-6 [ Links ]
75. Hengel B, Causer L, Matthews S, et al. A decentralised point-of-care testing model to address inequities in the COVID-19 response. Lancet Infect Dis 2021;21(7):e183-e190. https://doi.org/10.1016/S1473-3099(20)30859-8 [ Links ]
76. World Health Organization. European Union Funding boosts COVID-19 vaccination in Africa. Geneva: WHO, 2022. https://www.afro.who.int/news/european-union-funding-boosts-covid-19-vaccination-africa (accessed 20 May 2023). [ Links ]
77. Chou W-YS, Budenz A. Considering emotion in COVID-19 vaccine Communication: Addressing vaccine hesitancy and fostering vaccine confidence. Health Comm 2020;35(14):1718-1722. https://doi.org/10.1080/10410236.2020.1838096 [ Links ]
78. COVID-19 Treatment Guidelines Panel. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. Bethesda: National Institutes for Health, 2022. https://www.covid19treatmentguidelines.nih.gov/ (accessed 23 May 2023). [ Links ]
79. World Health Organization. Six in seven COVID-19 infections go undetected in Africa. Geneva: WHO, 2021. https://www.afro.who.int/news/six-seven-covid-19-infections-go-undetected-africa (accessed 25 May 2023) [ Links ]
80. Torres I, Sippy R, Sacoto F. Assessing critical gaps in COVID-19 testing capacity: The case of delayed results in Ecuador. BMC Pub Health 2021;21(1):637. https://doi.org/10.1186/s12889-021-10715-x. [ Links ]
81. Tsiouris F, Hartsough K, Poimboeuf M, et al. Rapid scale-up of COVID-19 training for frontline health workers in 11 African countries. Hum Res Health 2022;20(1):43. https://doi.org/10.1186/s12960-022-00739-8. [ Links ]
82. Gottlieb RL, Vaca CE, Paredes R, et al. Early remdesivir to prevent progression to severe COVID-19 in outpatients. N Engl J Med 2022;386(4):305-315. https://doi.org/10.1056/NEJMoa2116846. [ Links ]
83. Bhimraj A, Morgan RL, Shumaker AH, et al. IDSA guidelines on the treatment and management of patients with COVID-19. Clin Infect Dis. 2020;27:ciaa478. https://doi.org/10.1093/cid/ciaa478. [ Links ]
84. Seytre B, Barros C, Bona P, et al. Revisiting COVID-19 communication in Western Africa: A health literacy-based approach to health communication. Am J Trop Med Hyg 2021;105(3):708-712. https://doi.org/10.4269/ajtmh.21-0013. [ Links ]
85. Van Vuuren CJJ, van Vuuren JMJ. Perspectives of healthcare workers in South Africa on COVID-19 vaccination passports. Health SA 2022;27:1823. https://doi.org/10.4102/hsag.v27i0.1823. [ Links ]
86. Medicines Patent Pool. Medicines patent pool progress and achievements: Licences. MPP, 2023. https://medicinespatentpool.org/who-we-are/about- (accessed 25 May 2023). [ Links ]
87. Statistics South Africa. Mid-Year Population Estimates: 2021 (P0302). Pretoria: Stats SA, 2021. [ Links ]
88. Joint United Nations Programme on HIV and AIDS. South Africa. Country Factsheet. Geneva: UNAIDS, 2022. https://www.unaids.org/en/regionscountries/countries/southafrica (accessed 25 May 2023). [ Links ]
 Correspondence:
Correspondence:
R Perumal
rubeshan.perumal@caprisa.org
Accepted 19 October 2023


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}