










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSAMJ: South African Medical Journal
versão On-line ISSN 2078-5135
versão impressa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.113 no.11 Pretoria Nov. 2023
http://dx.doi.org/10.7196/SAMJ.2023.v113i11.497
RESEARCH
Treating drug-resistant tuberculosis in an era of shorter regimens: Insights from rural South Africa
J-D K LotzI, II; J D PorterI, III, IV; H H ConradieV; T H BoylesVI, VII, VIII; C B GauntIX; S DimandaX; D CortXI
IMB ChB, FCFP; Department of Family Medicine and Rural Health, Walter Sisulu University, Mthatha, South Africa
IIMB ChB, FCFP; Madwaleni District Hospital, Elliotdale, South Africa
IIIMB ChB, FCFP; Division of Family Medicine, Department of Family, Community, and Emergency Care, University of Cape Town, South Africa
IVMB ChB, FCFP; False Bay District Hospital, Cape Town, South Africa
VMB ChB, FCFP; Department of Family Medicine and Primary Care, Stellenbosch University, Cape Town, South Africa
VIBM BCh, Cert ID; Right to Care, Centurion, South Africa
VIIBM BCh, Cert ID; Clinical HIV Research Unit, University of the Witwatersrand, Johannesburg, South Africa
VIIIBM BCh, Cert ID; London School of Hygiene and Tropical Medicine, London, United Kingdom
IXMB ChB, MSc; Zithulele District Hospital, Coffee Bay, South Africa
XBMCP; Madwaleni District Hospital, Elliotdale, South Africa
XIMA, PhD; Department of Sociology, University of Massachusetts, Amherst, USA
ABSTRACT
BACKGROUND: Progressive interventions have recently improved programmatic outcomes in drug-resistant tuberculosis (DR-TB) care in South Africa (SA). Amidst these, a shorter regimen was introduced in 2017 with weak evidence, and has shown mixed results. Outcomes still fall short of national targets, and the coronavirus disease 2019 pandemic has undermined progress to date
OBJECTIVES: To describe the outcomes of participants treated for DR-TB using a shorter, compared with a longer, regimen in a deeply rural SA setting, and to explore other factors affecting these outcomes
METHODS: This retrospective cohort study describes outcomes in short and long DR-TB treatment regimens, over 5 years, at two rural treatment sites in SA. Characteristics were analysed for outcome correlates using multivariable logistic regression models
RESULTS: Of 282 treatment episodes, 62% were successful, with higher success in shorter (69%) compared with longer regimens (58%). Mortality was approximately 21% in both groups. Characteristics included high proportions of HIV co-infection (61%). Injectables (adjusted odds ratio (aOR) 3.00, 95% confidence interval (CI) 1.48 - 6.09), bedaquiline (aOR 3.16, 95% CI 1.36 - 7.35), increasing age (aOR 0.97, 95% CI 0.95 - 0.99) and HIV viraemia defined as final HIV-RNA viral load >1 000 copies/mL (aOR 0.16, 95% CI 0.07 - 0.37) were all significantly and independently associated with treatment success. Injectables (aOR 0.22, 95% CI 0.08 - 0.57), bedaquiline (aOR 0.05, 95% CI 0.01 - 0.19), increasing age (aOR 1.09, 95% CI 1.05 - 1.13), extra-pulmonary TB (aOR 8.15, 95% CI 1.62 - 41.03) and HIV viraemia (aOR 9.20, 95% CI 3.22 - 26.24) were all significantly and independently associated with mortality
CONCLUSION: In a rural context, treating DR-TB amid limited resources and a high burden of HIV co-infection, we found that after considering controls, a short regimen was no different to a longer regimen in terms of success or mortality. Therefore, by alleviating burdens on multiple stakeholders, a short regimen is likely to be favourable for rural patients, clinicians, and healthcare systems. Besides other previously described correlates of outcomes, HIV viraemia emerged as a novel marker for reliably predicting poor outcomes in DR-TB with HIV co-infection, and a pragmatic target for intervention
Despite being recently overshadowed by the urgency of the novel coronavirus disease 2019 (COVID-19) pandemic, tuberculosis (TB) remains a huge global burden. Approximately one-quarter of the world's population is infected by the bacillus Mycobacterium tuberculosis. Of these, 10.6 million cases progressed to active disease in 2021, and around 1.6 million people died.[1] In 2019, TB was still the leading global cause of death by a single infectious organism.[2] Drug-resistant TB (DR-TB) forms a significant proportion of this burden, comprising around 4% of incident cases.[1] In comparison to drug-susceptible strains (DS-TB), treatment up until recently has been prolonged (9 -24 months), is more expensive, and has less favourable outcomes.[1,3,4] As one of seven countries who shoulder two-thirds of the global burden, South Africa (SA) carries a disproportionately large share of global DR-TB.[1] The local DR-TB landscape included 13 005 patients diagnosed, and 8 743 (67%) initiated on treatment in 2019,[5] and a number of focused interventions have recently been introduced in response. However, set in the most unequal country in the world (based on Gini coefficients),[6] the contours of this landscape require careful mapping to understand the disaggregated effects of these interventions. A rural facet is, as far as the authors of this study are aware, yet to be well described.
Rurality is difficult to define, but according to the World Bank accounted for around one-third of South Africa's population in 2019.[7] Rural areas are marked by above-average levels of unemployment and poverty, poor infrastructure, lower proportions of healthcare workers employed, and unequal access to basic services, including healthcare.[8] Rural communities, and clinicians, therefore face unique barriers to care, but progressive iterations of national programmatic DR-TB care have provided potential ameliorants. [9] These include decentralisation of treatment sites,[10] improved diagnostics,[11] increasing access to novel and repurposed drugs,[12,13] and the introduction of a shortened (9 - 11-month) regimen[14] - subsequently modified to replace injectable agents with bedaquiline.[15,16] Amidst these, however, a shorter (9 - 11-month) regimen was initially introduced with weak evidence, and has shown mixed results.[17] It was with a conditional recommendation based on very low quality of evidence that the World Health Organization (WHO) initially recommended its implementation in their 2016 update on DR-TB treatment guidelines,[14] and that it should be implemented programmatically in SA in 2017.[16] Despite performing well under study conditions,[18,19] a subsequent review under programmatic conditions by the WHO then found a pooled adjusted odds ratio (aOR) of 2.0 for treatment failure or relapse when compared with longer regimens (and an aOR of 1.2 for death).[20] Evolution of regimens continues, and an even shorter 6-month regimen for treating multidrug-resistant (MDR)/rifampicin-resistant (RR)-TB (comprising bedaquiline, pretomanid, linezolid and moxifloxacin) has recently been recommended by the WHO and awaits programmatic implementation.[4]
As new data emerge to inform an agile DR-TB programme in SA, high-level interventions remain blunt tools without careful guidance using nuanced data from different contexts, and with critical monitoring over time. In light of existing aggregate data, and on the brink of the next iteration of programmatic regimen changes, this study thus sought to critically analyse the effects that an initial (9 -11-month) shorter regimen had on DR-TB treatment outcomes, specifically in a deeply rural SA setting. Such an analysis, focusing on two district hospital treatment programmes, over 5 years of iterative interventions and programmatic changes, also presented the opportunity to retrospectively observe the impacts that various other factors may have had on the risks of a successful treatment outcome, or death.
Such contextual descriptions are vital for mapping out the varied contours of the local, and indeed global, DR-TB landscape. It is hoped that elucidating these nuances may help inform and sharpen current and future tools at our disposal in the fight against TB - especially in the ongoing work towards equitable and quality care that rural healthcare workers strive to achieve with the communities they serve. With a COVID-19 pandemic undermining the progress made in recent years, understanding how to improve TB care is now more urgent than ever.
Objectives
This study thus sought to describe the outcomes of participants treated for DR-TB using a shorter (9 - 11-month), compared with a longer (>18-month) regimen, at two facilities in a deeply rural SA setting. Other characteristics affecting these outcomes were then explored.
Methods
Study design and participants
We performed a retrospective cohort study by analysing all existing patient records for episodes of RR-TB or MDR-TB treatment initiated by either of the two sites, between 1 January 2015 and 30 June 2018 for those treated using a long treatment regimen, and between 1 January 2015 and 31 March 2019 for those treated using a short regimen. This ensured that all episodes received outcomes before data collection. Patient records included onsite patient folders, and online records such as the EDRweb (WAMtechnology, 2018) - an online register of DR-TB patients in SA - and National Health Laboratory Services records of patient results. These records were accessed between July 2019 and October 2020.
Episodes were selected for shorter or longer regimens by local clinicians at respective treatment sites as part of routine programmatic care, based on contemporary SA guidelines. [10,12,15,21,22] A summary of standardised regimens used by participants is available in the attached appendix (https://www.samedical.org/file/2128; Table A1). According to these guidelines, exclusion criteria for a short regimen included previous exposure to second-line anti-tuberculous drugs for more than 1 month, evidence of extended resistance (to fluoroquinolones, injectable agents, bedaquiline, clofazimine, or linezolid), and extensive extra-pulmonary TB (EPTB) disease (including meningitis, pericarditis, osteoarticular, or abdominal disease) or extensive, bilateral, cavitatory pulmonary disease. While regimen selection occurred at the point of treatment initiation, certain situations also required a switch from shorter to longer regimens. These included new evidence of resistance, persistently positive sputum culture results at month 4 of treatment, premature discontinuation of key drugs (including bedaquiline, linezolid, levofloxacin, or clofazimine) for reasons such as toxicity, or a clinical deterioration. In such cases, the episode would be classified programmatically according to the final regimen received.[15]
Study exclusion criteria included episodes with any migration between treatment sites, and those with extended resistance -including dual mutations to isoniazid (in both inhA and katG genes), or resistance to either fluoroquinolones or injectables. These resistance patterns required alternative regimens and precluded the use of a shorter regimen. There were no exclusion criteria based on age, so episodes of treatment in all age groups were included.
Study setting
Two rural district level hospitals were thus selected for participation in this study. Situated along the Wild Coast area of the Eastern Cape Province - an area comprising part of what was formerly known as the Transkei, a designated 'homeland' that suffered from systematic deprivation under Apartheid rule in South Africa - Madwaleni and Zithulele Hospitals have both been designated as decentralised sites for the initiation and ongoing management of DR-TB since 2014.
DR-TB programmes are serviced by generalist medical practitioners and clinical associates (CAs), and form only one component of a comprehensive package of 24-hour district-level generalist care being offered at each facility. The number of doctors and CAs varied between 8 and 14 for each of the facilities over the period of this study, servicing populations of around 150 000 and 130 000, respectively, via a referral network of nurse-led primary-and community-level healthcare facilities. Generalists had not received specialised training in the management of DR-TB, but had benefited from telephonic and electronic support from more specialised practitioners at other facilities. More recently, specialist family physicians were employed at both facilities to further support comprehensive clinical oversight.
Data analysis
Data were initially reviewed and cleaned by screening for missing data or erroneous (impossible) data entries (such as negative time durations). These were mitigated by correlation between various sources of patient records (such as patient files and online records) and removing erroneous entries if no reasonable correction could be found. Once reviewed, de-identified data were analysed using Stata version 15 (StataCorp., USA). For categorical data, frequencies and proportions were described as n (%) unless otherwise specified. To describe measured data that were not normally distributed, medians (with interquartile ranges (IQR)) were used.
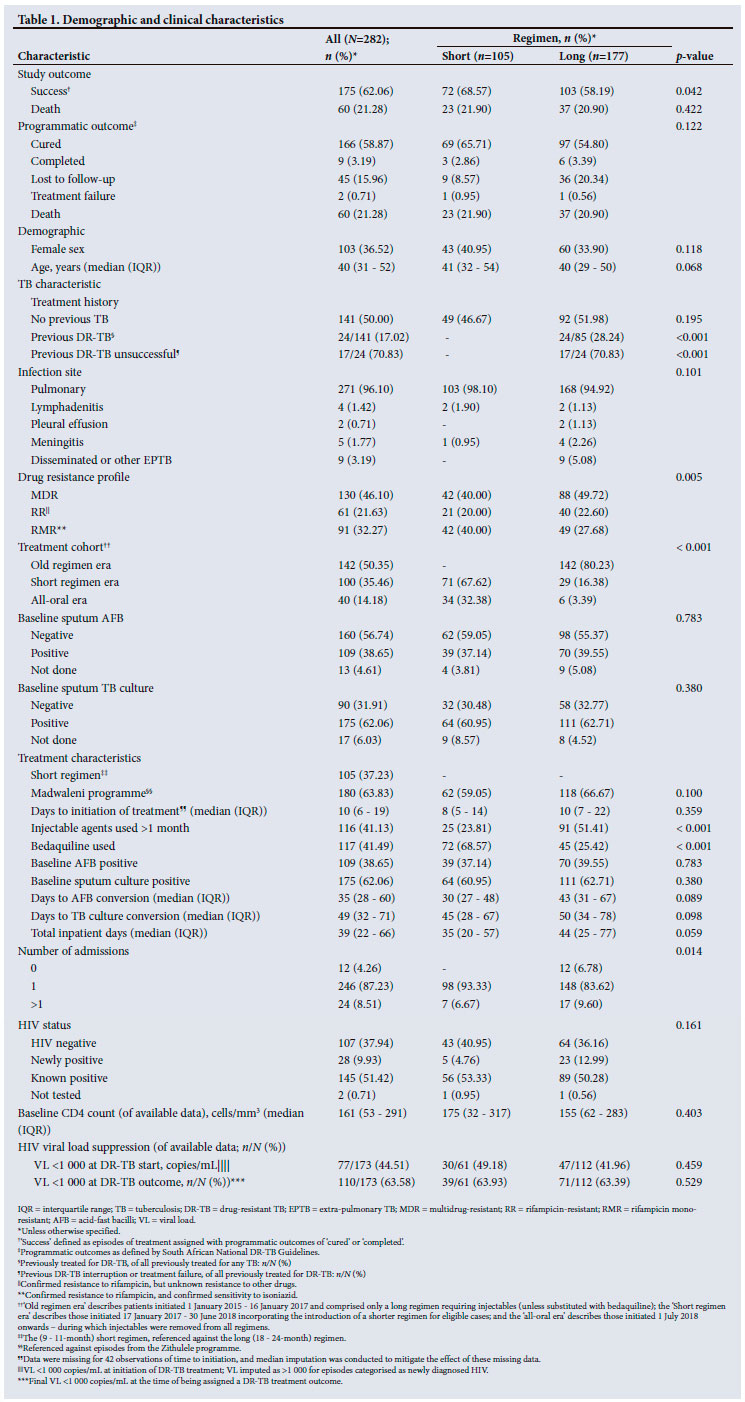
The two treatment groups of short and long regimens were compared in terms of outcomes and characteristics (Table 1). In accordance with WHO norms on reporting,[20,23] two main outcomes were defined for this study: treatment success (defined as WHO and SA National guideline definitions of 'cured' or 'completed'),[15,24] compared with any other outcome; and death compared with survival (i.e. death compared with all other programmatic outcomes). As this study used only programmatic definitions of DR-TB treatment outcomes and did not include further post-treatment follow-up, deaths that occurred after an outcome was assigned were not recorded. Characteristics were selected in accordance with data available in patient records, with additional categorisations including era of treatment initiation, and the clinical categorisation of HIV into 'negative', 'positive with successful viral load (VL) suppression' (defined as a final VL of <1 000 copies/mL before being assigned with a DR-TB treatment outcome) and 'positive with viraemia' (defined as a final VL of >1 000 copies/mL before being assigned with a DR-TB treatment outcome).
Outcomes and characteristics were initially compared, stratified according to shorter v. longer treatment regimens for a simple description. For hypothesis testing, Student's t-test was used to compare continuous, or binary, independent variables with a binary dependent variable. A χ2 test was performed to compare categorical independent variables with binary dependent variables.
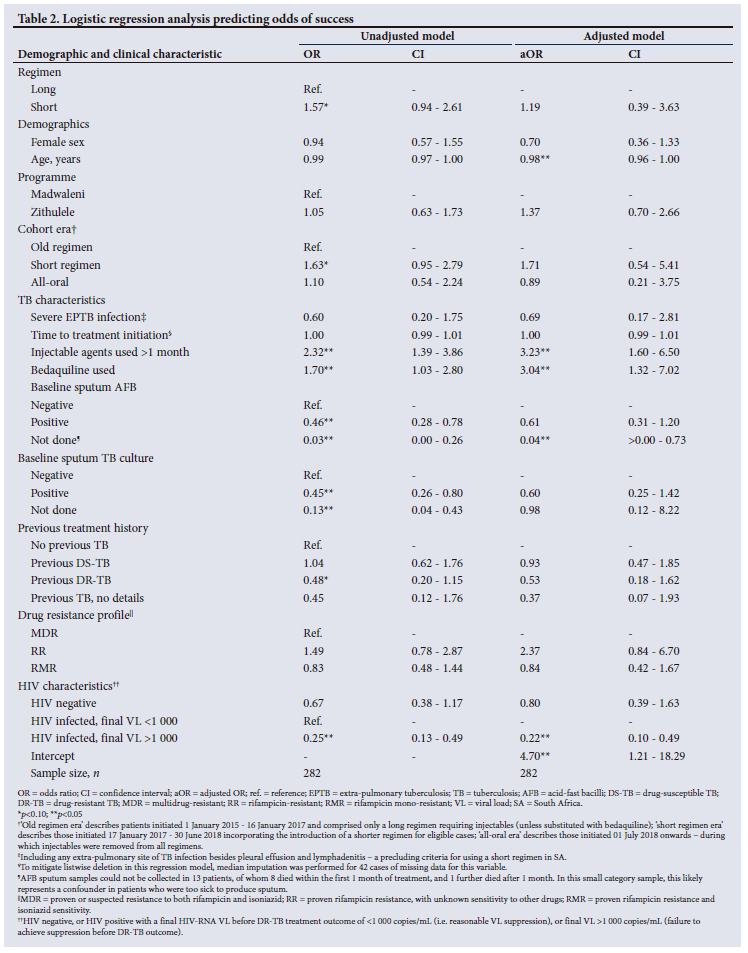
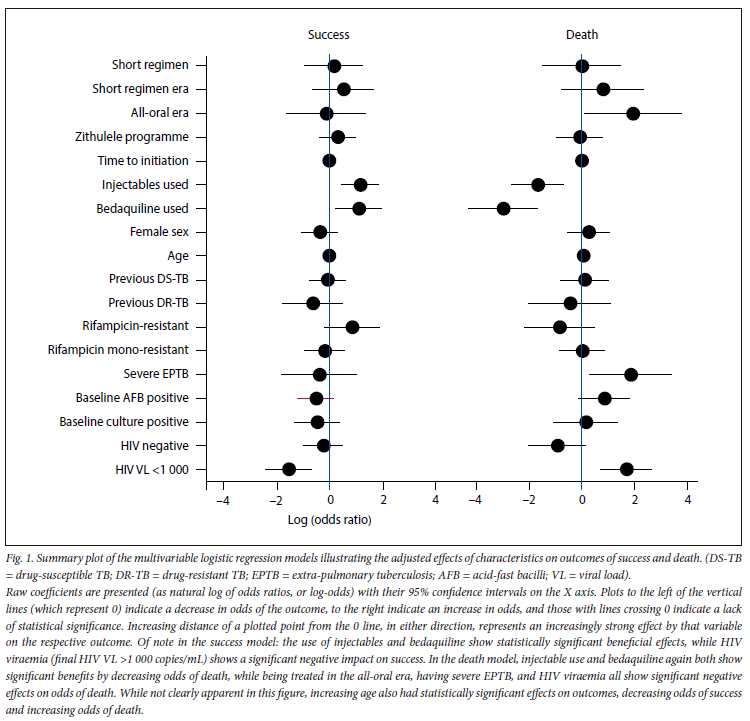
To elucidate the independent effect that regimen had on outcomes, as well as to explore factors that affected outcomes of treatment success or death, multivariable logistic regression models were built for each of the two study outcomes - a model for treatment success as a binary dependent variable of successful v. not successful, and a model for death as a binary dependent variable of death v. survival. A purposeful selection model-building strategy was performed.[25] Independent variables were selected for inclusion in the regressions based on known correlates demonstrated in other literature,[26,27] and variables deemed of clinical significance by the authors. Univariate followed by multivariable models are presented for each outcome in Tables 2 and 3. Summary plots of the multivariable models are presented in Fig. 1. All analyses were conducted according to existing data, with the exception of the 'time to initiation' variable, where median imputation was conducted for 42 cases of missing data in order to mitigate listwise deletion effects in the regression models. Further details can be obtained directly from the authors on request.
Ethical considerations
This analysis was approved by the Human Research Committee of Walter Sisulu University (ref. no. 116/2018), the Eastern Cape Health Research Committee (ref. no. EC-201904-024), and local management at research sites. The requirement for informed consent was waived as this retrospective record review had no influence on patient care. Adverse drug reactions were reported by clinicians prior to the study and are summarised in the appendix (https://www.samedical.org/file/2128; Table A.2).
Results
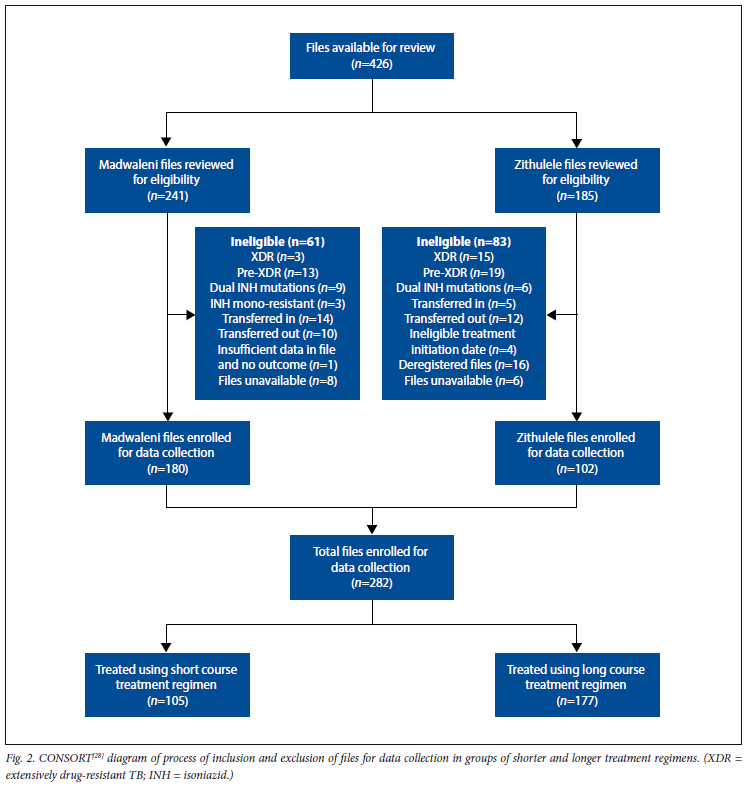
A total of 426 episodes of DR-TB treatment initiation were identified for inclusion, with 282 declared eligible according to study criteria (Fig. 2).[28] Baseline demographics and characteristics for all of these 282 eligible episodes are shown in Table 1. Of these, 105 (37%) were treated with the short treatment regimen, and 177 (63%) with the longer.
Overall, 175 episodes (62%) were successfully treated, and there were 60 deaths (21%). Rates of treatment success were significantly different between the short- and long-treatment groups; 72 episodes (69%) were successful after the shorter regimen treatment, compared with 103 episodes (58%) receiving the long regimen (p=0.042). There was no significant difference in deaths between the two treatment regimens (22% v. 21%, p=0.422). While a comparison of all categories of programmatic outcomes using a χ2 test yielded no significant difference when tested together (p=0.122), there was a notable difference observed in proportions of those lost to follow-up (9% v. 20%).
HIV characteristics did not differ significantly between the two treatment groups. Overall, 173 patients (61%) were co-infected with HIV, with a median (IQR) baseline (at the time of initiating DR-TB treatment) CD4 count of 161 cells/mm3 (53 - 291). Of these, 77 patients (45% of those co-infected) arrived for DR-TB treatment initiation with HIV VL <1 000 copies/mL, while 110 episodes (64% of those co-infected) achieved suppression <1 000 copies/mL by the time they received an outcome for their DR-TB treatment episode.
When demographics and clinical characteristics were compared between the short and longer treatment groups, significant differences were noted. Programmatically, previous exposure to DR-TB treatment precluded the use of a shorter regimen, and therefore treatment history differed significantly, while treatment cohorts (patients were initiated over three distinct programmatic eras in time during the course of this study, and so divided into three cohorts) also differed significantly (p<0.001) with the more recent introduction of the short regimen.
Besides programmatic influences, other significant differences included drug resistance profiles with lower proportions of MDR, and higher proportions of rifampicin mono-resistance (RMR) in the shorter regimen group (p=0.005). Of note, lower proportions of injectable use were observed in the short regimen (24% v. 51%, p<0.001), with higher proportions of bedaquiline use (69% v. 25%, p<0.001). Numbers of admissions differed, with no patients avoiding admission when treated with the shorter regimen, but more of these episodes only requiring a single admission (p=0.014).
Adjusted comparison of short v. long treatment regimens
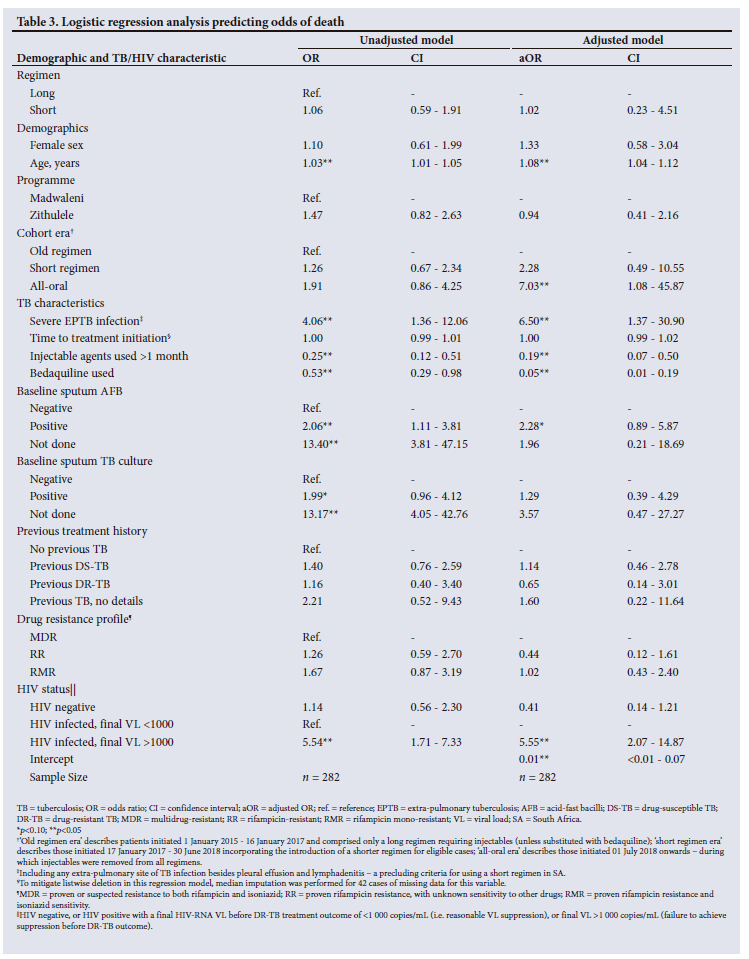
Table 2 presents the findings from a logistic regression model analysing the outcome of success, while Table 3 presents the analysis of death as an outcome. In contrast to an unadjusted analysis, controlling for other factors attenuated the treatment effect that a shorter treatment regimen had on a successful outcome. There was no impact on adjusted odds of treatment success (adjusted odds ratio (aOR) 1.19, 95% confidence interval (CI) 0.39 - 3.63), or mortality (aOR 1.02, 95% CI 0.23 - 4.51) when compared with a longer regimen (Fig. 1). In a further sensitivity analysis, the use of bedaquiline emerged as the leading variable responsible for the attenuation effect.
Exploring characteristics affecting treatment success and mortality
In an exploratory approach, several other characteristics were identified that independently and significantly affected outcomes of success or death, including demographics, TB characteristics and HIV characteristics (Tables 2 and 3, and Fig. 1).
Each year of increasing age decreased odds of success by 2% (aOR 0.98, 95% CI 0.96 - 1.00), and increased odds of death by 8% (aOR 1.08, 95% CI 1.04 - 1.12). Among the three cohorts of treatment episode eras, and while using the 'old regimen era' as a reference, the only effect observed was an increase in odds of death among episodes in the 'all-oral' era (aOR 7.03, 95% CI 1.08 - 45.87).
Severe EPTB (including any extra-pulmonary site of infection besides pleural effusions and lymphadenitis) did not affect odds of success, but increased odds of death significantly by more than five-fold (aOR 6.50, 95% CI 1.37 - 30.90). Exposure to injectable agents for longer than 1 month increased the odds of success significantly by more than two-fold (aOR 3.23, 95% CI 1.60 - 6.50) compared with not being exposed for as long or having no injectable exposure. This exposure also decreased odds of death by 81% (aOR 0.19, 95% CI 0.07 - 0.50). Exposure to bedaquiline increased odds of treatment success by more than two-fold (aOR 3.04, 95% CI 1.32 - 7.02), and decreased odds of death by 95% (aOR 0.05, 95% CI 0.01 - 0.19).
HIV status was divided into three categories: those who were not infected; those infected with reasonable suppression of their VL during their DR-TB treatment course (with a final VL of <1 000 copies/mL before being assigned a DR-TB outcome); and those with HIV viraemia (final VL >1 000 copies/mL before being assigned a DR-TB outcome). When compared with a reference category of HIV-infected with VL suppression, not being infected with HIV did not have any effects on success or death, while HIV viraemia had significant effects on outcomes of both success and death - independently decreasing odds of success by 78% (aOR 0.22, 95% CI 0.10 - 0.49), and increasing odds of death by over four-fold (aOR 5.55, 95% CI 2.07 - 14.87).
While characteristics of previous TB treatment exposures were already controlled for, a further sensitivity analysis was conducted to analyse the effect of excluding the 24 episodes of treatment with prior exposure to DR-TB therapy. The only statistically significant differences noted were in the regression model analysing death as an outcome; the effect observed in severe EPTB was marginally attenuated (aOR 5.75, 95% CI 0.97 - 34.00), while the effect of having a positive baseline acid-fast bacilli was slightly strengthened (aOR 2.77, 95% CI: 1.04 - 7.37).
Discussion
At the time of introducing a shorter (9 - 11-month) regimen to the SA DR-TB programme in 2017,[16] the WHO endorsed its use with very little evidence for its implementation.[14] It was in this landscape of scanty evidence that this study was designed and executed.
Since then, a large randomised non-inferiority trial has emerged showing it to be non-inferior to a longer regimen,[19] and a subsequent review by the WHO showed slightly poorer outcomes, but still supported its ongoing use in programmes.[20] While some of our individual patient data form part of those already analysed by the WHO, our methodology allowed for more detailed data to be collected directly from patient records, and we are able to present an analysis among a rural population facing very different barriers to care than those in urban settings.
In our rural SA context, over 5 years of treating RR/MDR-TB amid limited resources and a high burden of HIV co-infection, we observed a 69% rate of successful treatment using a shorter regimen, with a 22% mortality rate. For those treated using a longer regimen, the success rate was 58%, with 21% mortality.
Our outcomes were similar to those reported for the SA DR-TB programme. Nationally, those treated using a short regimen in 2017 had a collective success rate of 67%, with 18% mortality, while the longer regimen yielded 54% success and 20% mortality nationally in 2016.[17]
Despite these similarities, we found that a superficial report of outcomes belied a thorough understanding of the effects of a shorter regimen in our context. In a deeper analysis of these outcomes using multivariable logistic regression models, we found that after controlling for other characteristics, a shorter (9 - 11-month) regimen was no different to a longer (>18-month) regimen in terms of success (aOR 1.19, 95% CI 0.39 - 3.63) or mortality (aOR 1.02, 95% CI 0.23 - 4.51).
However, by alleviating burdens on multiple stakeholders, a short regimen is still likely to be highly favourable for rural patients, clinicians and healthcare systems. By reducing indirect costs such as travel expenses and time unable to work, a shorter regimen likely benefits the high proportion of our economically fragile population facing catastrophic household costs due to a diagnosis of DR-TB.[29-32] By reducing the time many patients need to be managed and monitored by almost a half, the workload on a stretched workforce of healthcare workers is dramatically relieved. Finally, costing studies have shown significant potential cost-saving for a healthcare system by choosing a shorter treatment regimen.[32,33]
Besides other previously described correlates of outcomes such as bedaquiline use, age and severe EPTB infection,[26,27] we found that HIV viraemia (in terms of poor virological suppression) emerged as a novel surrogate for reliably predicting poor outcomes in DR-TB with HIV co-infection.
The effect that HIV co-infection has on outcomes in DR-TB has been described in terms of whether patients are co-infected with HIV,[34,35] and whether they are receiving ART or not,[26,29] but according to our data signals it appears that distinguishing persistent HIV viraemia from suppression may be an important and as yet largely unexplored nuance that significantly affects DR-TB outcomes in co-infected patients. Due to the limitations of observational data, this study is only able to establish a relationship between HIV viraemia and the odds of successful DR-TB treatment or mortality, not causality. Therefore, the effects we observed may, for example, be due to immunological or other host factors at play, or it may be that HIV viraemia might reflect problems with patient adherence to ART and to DR-TB treatment. Whatever the underlying reason, the pragmatic conclusion for clinicians seems to remain: VL should be monitored carefully, a patient with HIV and DR-TB co-infection should be flagged as being at high risk for unfavourable DR-TB outcomes if VL remains >1 000 copies/mL, and measures should be taken to check adherence (to both ART and DR-TB treatment) and expedite the timely provision of adequate ART in order to achieve VL suppression. Reasons behind this relationship, and its utility for monitoring and guiding interventions during DR-TB treatment, should be further explored.
Study limitations
This study is limited in some respects: data are observational; relapse rates could not be determined from existing records; and some variables that may influence outcomes (such as body mass index, concomitant diabetes mellitus and the use of linezolid) were not included owing to limitations in data collection. However, results remain statistically significant and clinically relevant.
Conclusion
In reporting these findings, we look forward to a renewed emphasis on good HIV care in a setting burdened with co-infection of HIV and TB, as well as the evolution of shorter and all-oral DR-TB regimens incorporating bedaquiline - especially those recently recommended by the WHO[4] - and their ongoing careful analysis in real-world programmatic settings. This ongoing analysis would do well to consider the values and preferences of all stakeholders involved, not least of which are the people and communities affected by TB.
We therefore also acknowledge the vision by the WHO[36] and SA Department of Health,[37] that successful outcomes require more than a biomedical focus. While global and national therapeutic and programmatic interventions continue to drive ongoing improvements in outcomes, further progress in the fight against DR-TB likely requires more local nuances than simply relying on programmatic broad strokes and therapeutic silver bullets. As frontline workers in a rural setting, we too support the vision to strive toward a patient-centred approach to care, and seek to add weight to the multidisciplinary approach involving multiple stakeholders to address upstream determinants of TB in the communities we serve, to stop TB together.
Declaration. The research for this study was done in partial fulfilment of the requirements for JDL's MMed (Family Medicine) degree at Walter Sisulu University.
Acknowledgements. The primary author (JDL) extends sincere thanks for the wholehearted support of this work: to friends and family of the Madwaleni 'village', to rural colleagues at Zithulele (and beyond), and to a cheering Department of Family Medicine and Rural Health at WSU. And then to his family, who filled him up, and a loving God who lifted him up, and to whom this work belongs.
Author contributions. JDL is the primary author. JDL, CBG, JDP, HHC and DC designed the study. JDP and HHC supervised the study. All authors contributed to drafting and final editing of the manuscript. JDL and SD conducted data collection and curation. JDL and DC conducted the data analyses. All authors read and approved the final manuscript.
Funding. Research reported in this publication was supported by the National Research Foundation and the Discovery Foundation.
Conflicts of interest. None.
References
1. World Health Organization. Global tuberculosis report 2022. Geneva: WHO, 2022. https://www.who.int/teams/global-tuberculosis-programme/tb-reports (accessed 10 October 2022). [ Links ]
2. World Health Organization. Global tuberculosis report 2020. Geneva: WHO, 2020. https://www.who.int/publications/i/item/9789240013131 (accessed 15 November 2020). [ Links ]
3. Lange C, Dheda K, Chesov D, Mandalakas AM, Udwadia Z, Horsburgh CR. Management of drug-resistant tuberculosis. Lancet 2019;394:953-966. https://doi.org/10.1016/s0140-6736(19)31882-3 [ Links ]
4. World Health Organization. Rapid communication: Key changes to the treatment of drug-resistant tuberculosis. Geneva: WHO, 2022. https://www.who.int/southeastasia/publications/i/item/WHO-UCN-TB-2022-2#:~:text=These%20updates%20include%20shorter%20novel,of%20MDR%2FRR%2DTB (accessed 15 July 2022). [ Links ]
5. World Health Organisation. Global tuberculosis report 2019. Geneva: WHO, 2019. https://www.who.int/teams/global-tuberculosis-programme/tb-reports/global-report-2019 (accessed 15 November 2020). [ Links ]
6. The World Bank. Inequality in Southern Africa: An assessment of the Southern African Customs Union. Washington, DC: World Bank, 2022. https://documents1.worldbank.org/curated/en/099125303072236903/pdf/P1649270c02a1f06b0a3ae02e57eadd7a82.pdf (accessed 10 October 2022). [ Links ]
7. World Bank. Rural population - South Africa. World Bank, 2019. https://data.worldbank.org/indicator/SP.RUR.TOTL.ZS?locations=ZA (accessed 24 October 2020). [ Links ]
8. Eagar D, Versteeg-Mojanaga M, Cooke R. Defining rurality within the context of health policy, planning, resourcing and service delivery: complexities, typologies and recommendations. Johannesburg: Rural Health Advocacy Project, 2014. http://rhap.org.za/wp-content/uploads/2019/11/RHAP-Submission-NHI-Bill_291119.pdf (accessed 10 October 2020). [ Links ]
9. Cox H, Dickson-Hall L, Jassat W, et al Drug-resistant tuberculosis in South Africa: History, progress and opportunities for achieving universal access to diagnosis and effective treatment. In: Padarath A, Barron P, eds. South African Health Review 2017. 20th ed. Durban: Health Systems Trust, 2017:157-168. [ Links ]
10. National Department of Health, South Africa. Multi-drug resistant tuberculosis: A policy framework on decentralised and deinstitutionalised management for South Africa. Pretoria: NDoH, 2011. http://www.sanacws.org.za (accessed 8 October 2020). [ Links ]
11. Dheda K, Cox H, Esmail A, Wasserman S, Chang KC, Lange C. Recent controversies about MDR and XDR-TB: Global implementation of the WHO shorter MDR-TB regimen and bedaquiline for all with MDR-TB? Respirology 2018;23(1):36-45. https://doi.org/10.1111/resp.13143 [ Links ]
12. National Department of Health, South Africa. Introduction of new drugs and drug regimens for the management of drug-resistant tuberculosis in South Africa: Policy framework. Pretoria: NDoH; 2015. [ Links ]
13. Ndjeka N, Conradie F, Schnippel K, et al. Treatment of drug-resistant tuberculosis with bedaquiline in a high HIV prevalence setting: An interim cohort analysis. Int J Tuberc Lung Dis 2015;19(8):979-985. https://doi.org/10.5588/ijtld.14.0944 [ Links ]
14. World Health Organisation. WHO treatment guidelines for drug-resistant tuberculosis: 2016 update. Geneva: WHO, 2016. http://apps.who.int/iris/handle/10665/250125 (accessed 5 October 2020). [ Links ]
15. National Department of Health, South Africa. Management of rifampicin-resistant tuberculosis: A clinical reference guide. Pretoria: NDoH, 2019. [ Links ]
16. Ndjeka N, Hughes J, Reuter A, et al. Implementing novel regimens for drug-resistant TB in South Africa: What can the world learn? Int J Tuberc Lung Dis 2020;24(10):1073-1080. https://doi.org/10.55.5588/ijtld.20.0174 [ Links ]
17. Massyn N, Barron P, Day C, Ndlovu N, Padarath A. District Health Barometer 2018/19. Vol. 53. Durban: Health Systems Trust, 2020. [ Links ]
18. Van Deun A, Maug AKJ, Salim MAH, et al. Short, highly effective, and inexpensive standardised treatment of multidrug-resistant tuberculosis. Am J Respir Crit Care Med 2010;182(5):684-692. https://doi.org/10.1164/rccm.201001-0077OC [ Links ]
19. Nunn AJ, Phillips PPJ, Meredith SK, et al. A trial of a shorter regimen for rifampin-resistant tuberculosis. N Engl J Med 2019;380(13):1201-1213. https://doi.org/10.1056/NEJMoa1811867 [ Links ]
20. World Health Organisation. WHO consolidated guidelines on drug-resistant tuberculosis treatment. Geneva: WHO, 2019. [ Links ]
21. Directorate Drug-Resistant TB TB & HIV, National Department of Health, South Africa. Management of drug-resistant TB: Policy guidelines. Pretoria: NDoH, 2013. http://www.health-e.org.za/wp-content/uploads/2014/06/MDR-TB-Clinical-Guidelines-Updated-Jan-2013.pdf (accessed 12 October 2020). [ Links ]
22. National Department of Health, South Africa. Interim clinical guidance for the implementation of injectable-free regimens for rifampicin-resistant tuberculosis in adults, adolescents and children. Pretoria: NDoH, 2018. [ Links ]
23. World Health Organization. Global Tuberculosis Report 2021. Geneva: WHO, 2021. www.who.int/publications/i/item/9789240037021 (accessed 18 October 2022). [ Links ]
24. World Health Organization. Definitions and reporting framework for tuberculosis - 2013 revision. Vol. 18, Eurosurveillance. Geneva: WHO, 2013. [ Links ]
25. Bursac Z, Gauss CH, Williams DK, Hosmer DW. Source code for biology and purposeful selection of variables in logistic regression. Source Code Biol Med 2008;3(17):1-8. [ Links ]
26. Ahmad N, Ahuja SD, Akkerman OW, et al. Treatment correlates of successful outcomes in pulmonary multidrug-resistant tuberculosis: an individual patient data meta-analysis. Lancet 2018;392(10150):821-834. https://doi.org/10.1016/S0140-6736(18)31644-1 [ Links ]
27. Ndjeka N, Campbell J, Meintjes G, et al. Treatment outcomes 24 months after initiating short, all-oral bedaquiline-containing or injectable-containing rifampicin-resistant tuberculosis treatment regimens in South Africa: A retrospective cohort study. Lancet Infect Dis 2022;22(7):1042-1051. https://doi.org/10.1016/S1473-3099(21)00811-2 [ Links ]
28. Schulz KF, Altman DG, Moher D. CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials. PLoS Med 2010;7(3):1-7. https://doi.org/10.1186/1741-7015-8-18 [ Links ]
29. Foster N, Vassall A, Cleary S, Cunnama L, Churchyard G, Sinanovic E. The economic burden of TB diagnosis and treatment in South Africa. Soc Sci Med 2015;130:42-50. https://doi.org/10.1016/j.socscimed.2015.01.046 [ Links ]
30. Sweeney S, Vassall A, Guinness L, et al. Examining approaches to estimate the prevalence of catastrophic costs due to tuberculosis from small-scale studies in South Africa. Pharmacoeconomics 2020;38(6):619-631. https://doi.org/10.1007/s40273-020-00898-3 [ Links ]
31. Verguet S, Riumallo-Herl C, Gomez GB, et al. Catastrophic costs potentially averted by tuberculosis control in India and South Africa: A modelling study. Lancet Glob Heal 2017;5(11):e1123-1132. https://doi.org/10.1016/S2214-109X(17)30341-8 [ Links ]
32. Madan JJ, Rosu L, Tefera MG, et al. Economic evaluation of short treatment for multidrug-resistant tuberculosis, Ethiopia and South Africa: The stream trial. Bull World Health Organ 2020;98(5):306-314. https://doi.org/10/2471/BLT.19.243584 [ Links ]
33. Masuku SD, Berhanu R, Van Rensburg C, et al. Managing multidrug-resistant tuberculosis in South Africa: A budget impact analysis. Int J Tuberc Lung Dis 2020;24(4):376-382. https://doi.org/10.5588/ijtld.19.0409 [ Links ]
34. Bastos ML, Cosme LB, Fregona G, et al Treatment outcomes of MDR-tuberculosis patients in Brazil: A retrospective cohort analysis. BMC Infect Dis 2017;17(718):1-12. https://doi.org/10/1186/s12879-017-2810-1 [ Links ]
35. Edessa D, Sisay M, Dessie Y. Unfavorable outcomes to second-line tuberculosis therapy among HIV-infected versus HIV-uninfected patients in sub-Saharan Africa: A systematic review and meta-analysis. PLoS One 2020;15(8): e0237534. https://doi.org/10.1371/journal.pone.0237534 [ Links ]
36. World Health Organization. The End TB Strategy. Vol. 53. Geneva: WHO, 2015. [ Links ]
37. South African National AIDS Council. South Africa's National Strategic Plan for HIV, TB and STIs 2017-2022. Pretoria: SANAC, 2017. https://sanac.org.za//wp-content/uploads/2017/06/NSP_FullDocument_FINAL.pdf (accessed 14 October 2020). [ Links ]
 Correspondence:
Correspondence:
J-D K Lotz
jdlotz@gmail.com
Accepted 5 October 2023


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}