










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.113 n.11 Pretoria Nov. 2023
http://dx.doi.org/10.7196/SAMJ.2023.v113i11.814
RESEARCH
LSD and psilocybin for chronic nociplastic pain: A narrative review of the literature supporting the use of classic psychedelic agents in chronic pain
J J N van der WaltI; R ParkerII
IMB ChB, FCA (SA); Department of Anaesthesia and Perioperative Medicine, Faculty of Health Sciences, University of Cape Town, South Africa
IIMSc (Pain), PhD; Department of Anaesthesia and Perioperative Medicine, Faculty of Health Sciences, University of Cape Town, South Africa
ABSTRACT
Healthcare providers face the challenging task of managing patients who suffer from chronic nociplastic pain conditions. Pain is a multidimensional experience, and the current approach to managing people in chronic pain often fails to meet the needs of these patients. Novel ways of treating people who suffer from chronic nociplastic pain with classic psychedelic agents may offer a new lens through which to approach their pain. Lysergic acid diethylamide (LSD) and psilocybin are both serotonergic agents with a long history of use in treating people with chronic pain and mental health disorders. The new wave of research into psychedelics for major depressive disorder provides an opportunity to investigate and understand the potential for incorporating these drugs into chronic pain management pathways. This narrative review presents healthcare workers with a framework to understand the method of action of these drugs in chronic nociplastic pain pathways and a brief history into their use. We conducted an online search using Pubmed with keywords 'chronic pain' AND/OR 'psilocybin' AND/OR 'lysergic acid diethylamide' AND/OR 'psychedelics' with no date limit applied. We identified further articles that contained information on the neuroscience of psychedelics and the serotonergic system using Google Scholar. During the final stages of writing the article, the latest publications on psychedelics and chronic pain in leading pain journals were again included to update the information.
'The human body is the stage where the psycho-cosmic drama takes place' - Lama Anagarika Govinda
Chronic pain is one of the leading global burdens of disease.[1] It impacts an estimated 20% of the global population, and often as comorbidity with other disease states. The International Association for the Study of Pain (IASP) has adopted a new definition of pain that describes the experience of pain from the perspective of the person suffering with pain.[1] The new IASP definition from 2020 defines pain as 'an unpleasant sensory and emotional experience associated with, or resembling that associated with, actual or potential tissue damage'. The ability to view pain through the lens of suffering allows pain to be understood as a conscious construct of the brain in response to a perceived threat.[2] These threats may constitute a variety of internal or external factors. Viewing pain through the eyes of the person with pain incorporates the biopsychosocial aspects of the lived experience.[3] This approach also highlights the experiential aspect of pain as part of emotional and cognitive processing that interacts with the mechanistic aspect of nociceptive pain physiology on a receptor pathway level. When people suffer from chronic pain these factors become compounded.
In 2016, the term nociplastic pain was adopted to describe chronic pain due to an alteration in peripheral and central nervous system (CNS) processing of sensory and emotional stimuli.[4] The adoption of nociplastic pain as a mechanistic descriptor of chronic pain that is not clearly defined as either nociceptive or neuropathic allows previous diagnoses such as functional neurological disorder to be appropriately classified as distinct from pain due to tissue damage,
inflammation or damage to the nervous system. In reality, nociplastic pain rarely exists in isolation, but is rather part of a pain continuum with nociceptive and neuropathic pain.[4] The basic neurophysiology of nociplastic pain is described by increased facilitation or decreased inhibition of painful stimuli in the CNS. The neuromatrix of pain proposed by Melzack[5] is a suitable framework to understand the multidimensional nature of nociplastic pain, and especially points towards the co-existence of mental health disorders in people with nociplastic pain. Recent studies have signalled significant overlap in the neuroplastic changes that underlie both the chronification of pain and major depressive disorder (MDD).[6] The prevalence of chronic pain in people with MDD is between 51.8% and 59.1%. The involvement of the monoamine neurotransmitter serotonin (5-HT) and noradrenaline in pain and mood processing points to a shared pathophysiology and response to treatment.[7]
All people with pain and chronic pain face a multitude of therapeutic challenges on their road to finding treatment and making peace with their life with pain. Some of these challenges include drug polypharmacy and drug side-effects that not only complicate their pain treatment, but are often insufficient to meet the need to ease their suffering, or fail to enable them to re-engage with meaningful life roles.[3] People with pain have extensive psychological, social and spiritual needs, and may desire to reclaim an internal locus of control to address unresolved family and relationship issues.[8,9] Recent developments in the approach to managing chronic pain
have expanded treatment modalities beyond oral analgesics and interventional pain procedures.[10] Today we include psychological support, patient education and physical therapy to manage people with pain. However, despite this expanded treatment approach, we often fail to meet the complex demands of people with pain. Even with multidisciplinary interventions using mindfulness and cognitive behavioural therapy (CBT), people with chronic pain present a treatment challenge to the most caring physician. We propose that management of the chronic pain experience must focus not only on the mechanisms of nociception on a receptor level, but move beyond physiology to incorporate the experiential aspect of pain as an 'embodied' experience within a specific psychosocial 'embedded' environment.[11]
Recent neuroimaging studies combined with small sample interventions with classic psychedelic agents may point towards a possible means of improving the treatment of chronic pain on a mechanistic and experiential level.[12] The classic psychedelics are those drugs with 5-HT2A receptor activity, and include lysergic acid diethylamide (LSD) and psilocybin. These drugs may have antinociceptive effects acting on 5-HT1A receptors in descending noxious inhibitory pathways, while the mood-enhancing effects of psychedelic induced 5-HT2A agonism in the cerebrum appear to act on the neuroplastic changes that occur in nociplastic pain.[13,14]
The classic psychedelic agents
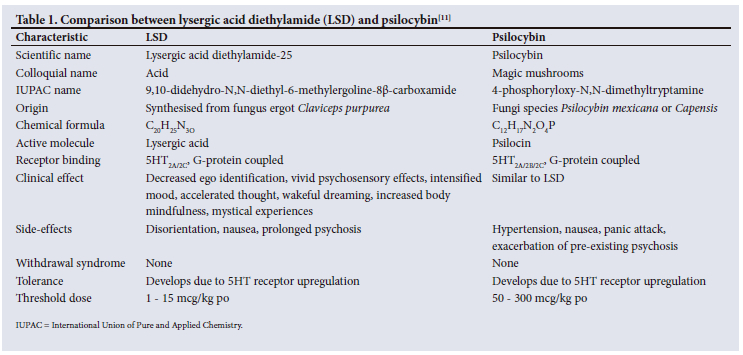
LSD is part of a family of plant-based alkaloids that include other psychedelic agents such as psilocybin.[11] Their clinical effect is due to serotonin receptor binding in the CNS. LSD was first synthesised by the Swiss chemist Albert Hofmann in 1938 while investigating the smooth muscle-contracting effects of ergotamine found in the fungus Claviceps purpurea.[9] Hofmann experienced a non-ordinary state of consciousness (NOSC) after accidentally inhaling a preparation of LSD-25, and described the psychedelic experience of increased bliss, decreased ego identification and altered perceptual experience.
Psilocybin is a plant-based alkaloid and has been used as an entheogen in indigenous cultures for thousands of years.[15] Albert Hofmann identified the chemical structure of psilocybin in 1958. Psilocybin shares the tryptamine chemical backbone of LSD.[16] After oral ingestion it is dephosphorylated in the liver into the active form psilocin, which binds 5-HT2A receptors in the cerebral cortex.[9] This leads to the depolarisation of pyramidal neurons in the cortex and dysregulation of central brain regions, with a resultant increase in entropy.[16,17] In Table 1, we compare the two agents. Psilocybin's 5HT1A and 2A receptor binding in the CNS has similar effects to LSD on cognition, emotional processing, self-awareness and the perception of pain, which underpins its potential therapeutic benefit in treating people suffering with pain. Numerous small trials of LSD and psilocybin for chronic pain have already shown a good safety profile, with minimal physical dependance, withdrawal syndrome, or compulsive drug seeking compared with other analgesic agents.[11]
Psychedelic research
The history of psychedelic research into LSD and psilocybin is complex and has been shaped by public opinion and political interference. After the discovery of LSD-25 by Albert Hofmann in 1943, Sandoz marketed the substance as 'Delysid' for use in psychiatric research and psychotherapy.[11] During the 1950s and 1960s, LSD showed promising results in the management of drug dependency and alcohol addiction.[3] There are more than 1 000 published reports on the clinical use of LSD in psychotherapy from 1949 to 1966.[18] Although the trials published during these years had small sample sizes and will not live up to the scrutiny that we expect from modern clinical research, they did point towards the safety and tolerability of LSD in a clinical setting. During the American 'counterculture' movement in the late 1960s and 1970s, LSD use became associated with anti-government sentiment, and the US government led a global campaign to shut down research in LSD and other controlled substances. The Controlled Substances Act of 1970 made LSD and psilocybin schedule 1, which prohibited further research. From 1977 until the early 2000s, no more LSD research was published, despite overwhelming evidence pointing towards therapeutic benefit.[11]
Psilocybin is a naturally occurring plant-based psychedelic with a long history of use stretching back thousands of years in indigenous societies. In these societies, it is supported by an active culture of self-medication, with positive reports on its effects on mental health.[12] There have been no reports of direct mortality, and no withdrawal following chronic use.[11] The use of psilocybin was popularised in 1957 when the American amateur ethnobotanist Robert Gordon Wasson published his experiences with these fungi in central America. The following year Albert Hofmann identified the tryptamine backbone of psilocybin. The use of psilocybin in clinical research ended at the same time as LSD research as the Controlled Substances Act was enforced.
The new wave of psychedelic research that has slowly been building since the 1990s has been termed the 'psychedelic renaissance'.[12] The new frontier of neurocognitive science using neuroimaging has been able to bring interest in the therapeutic benefit of psychedelic drugs back into the domain of clinical research. Psychiatrists have enrolled small sample trials exploring the potential benefit of psychedelic drugs in treating anxiety, MDD and end-of-life cancer with depression, showing promising results. The successful use of psilocybin in managing obsessive compulsive disorder, treating alcohol addiction and for smoking cessation has also been reported.[11] These small-sized trials have revealed the good safety profile of these drugs, and how a carefully controlled environment with a focus on adequate self-preparation and a well-supported clinical setting ensures a low risk for adverse effects.[19] Larger clinical trials have been enrolled, and in 2022, Compass Pathways, a mental healthcare company based in the UK, began the world's first phase 3 clinical trial using psilocybin for treatment-resistant depression. A New York-based biotech company called Mindmed plans to enrol a phase 2B clinical trial to treat generalised anxiety disorder with LSD. This will be the most advanced clinical trial into LSD, for any indication.
Between 1964 and 1977, 5 small-scale clinical trials and a case series looked at the use of LSD in chronic pain.[20-24] In 1964, Kast and Collins[20] reported that LSD had a superior analgesic effect to pethidine and dihydromorphine in patients with severe cancer pain and gangrene. The analgesic effect lasted for at least 7 hours post dose in 74.4%, and 19 hours after a single dose of 100 μg in 48.9% of patients. In 1967, Kast[21] reported on the use of 100 μg of LSD in a case series of 128 terminally ill patients. Pain intensity was decreased for 3 weeks. In 1967, Pahnke et al.[22] studied the effect of LSD on terminal metastatic cancer with depression. They commented on improved pain, mood and anxiety in the 22 patients treated with LSD psychotherapy. Grof et al.[23] enrolled 31 patients with metastatic cancer into an LSD-assisted psychotherapy programme in 1973. These patients received psychological support before, during and after LSD therapy. They found an improvement in pain severity, preoccupation with pain and physical suffering.[23] The last case series reported before research was shut down was by Fanciullacci et al.[24] in 1977. Seven patients with phantom limb pain were treated with sub-hallucinogenic doses of LSD (25 μg per day for 1 week followed by 50 μg per day for a further 2 further weeks). They reported decreased analgesic requirements, and two patients had resolution of their pain.[24]
During the new wave of psychedelic research, both Sewell et al.[25] in 2006, and Schindler et al.[26] in 2016, used surveys and interviews to collect data from people who were self-medicating with LSD and/ or psilocybin for their cluster headaches. They reported improved analgesia compared with conventional treatments, with longer periods of remission. Recent trials on end-of-life depression in cancer patients showed a sustained improvement in mood and quality of life, which could have a substantial effect on managing chronic pain in these patients.[27] In 2021, researchers at Imperial College London conducted structured interviews with people who self-medicate their chronic pain symptoms using classic psychedelic agents. This small-sample case series, in preparation for a much larger randomised controlled trial, revealed a decrease in the experience of pain during the psychedelic session and for up to 5 days after treatment, before their pain returned to baseline. The most exciting revelation from these interviews relates to the lasting psychological and emotional effect the psychedelics had on those interviewed. They describe increased resilience, body-self-awareness and psychological flexibility, which led to feelings of acceptance, agency and hope.[28] Most recently, the journal Pain published a case series of three people with chronic neuropathic pain who took low-dose psilocybin, termed 'microdosing', to manage their symptoms.[29] The authors commented on the favourable effects of microdosing, with minimal side-effects and a decreased need for traditional analgesic agents.
The neuroplastic changes of chronic nociplastic pain
The IASP define central sensitisation as the increased responsiveness of nociceptive neurons in the CNS to their normal or subthreshold afferent input.[30] The peripheral and central sensitisation that occurs in acute nociceptive pain is sustained with intensifying consequences in chronic nociplastic pain. These mechanisms have been well described in the literature, and some of them include the process of phenotypic switching, altered gene expression and the modification of intracellular proteins.[30,31] The neuroplastic changes of chronic nociplastic pain are the targets for the classic psychedelic agents. They may have an effect on (i) shifting interoceptive focus in the insula, (ii) modulate neurotrophic factors, (iii) synaptogenesis in the CNS and (iv) CNS inflammatory modulation.
Neuroimaging studies of people with chronic nociplastic pain have recently identified a signal pointing towards a biodynamic process that may also describe one of the processes leading to the chronification of pain.[32] Sensory afferent Αδ and C-fibers that innervate the entire human body terminate in lamina 1 of the dorsal spinal horn (DSH). Homeostatic information on temperature, nociception, metabolism, touch, muscle contraction as well as hormonal and immunological function forms a meta representation of interoceptive activity in the body.[32] This interoceptive map projects towards the insular cortex (IC) via lamina 1 in the DSH spino-thalamo-cortical tract, and plays an important role in the generation of pain. In chronic nociplastic pain states there is a shift from the posterior part of the insula, involved in sensory processing, towards the anterior insula, which is involved in the emotional and limbic systems.[33] The shift in activity from the posterior to the anterior insula in chronic nociplastic pain reflects an increased emotional response to pain and a decrease in accurate interoceptive processing.[11,32] The action of LSD and psilocybin on cortical 5-HT2A receptors may improve these neuroplastic changes in chronic pain and reorientate the person with pain towards a less distressing emotional response and accurate sensory awareness of nociception and pain.[11,18]
A further link in the formation of nociplastic pain is the neurotrophic factors and lipids that influence signalling pathways in the CNS.[34] Brain-derived neurotrophic factor (BDNF) belongs to the family of neurotrophic factors, and is involved in neuroplasticity and synaptogenesis.[6] Decreased levels of BDNF have been implicated in chronic nociplastic pain conditions as well as in the development of MDD. By modulating peripheral and central synaptic plasticity, BDNF can alter pain perception and the level of pain-induced depression. LSD and psilocybin have been shown to increase BDNF and glial cell line-derived neurotrophic factor, which may improve synaptogenesis in people suffering from pain and MDD.[35]
The synaptogenic changes of depression and chronic nociplastic pain may also be influenced by inflammatory mediators.[6] Depression is increasingly being described as an inflammatory disorder associated with other chronic nociplastic pain syndromes such as inflammatory bowel syndrome (IBS), fibromyalgia syndrome (FMS) and complex regional pain syndrome (CRPS). Inflammatory chronic pain conditions may therefore also predispose patients to the development
of depression, and vice versa.[7] Inflammatory mediators released after neuronal injury are also involved in MDD and nociplastic chronic pain.[36] Microglial cell activation seen in response to nerve injury has been implicated in the development of neuropathic and other types of chronic pain. The role of microglia and astrocytes in neuronal plasticity has been described in the pathophysiology of chronic pain and in MDD.[36,37] LSD- and psilocybin-induced activation of the 5-HT2A receptor upregulates genes associated with neuroplasticity and suppresses TNFa-induced inflammation. Protein kinases such as mammalian target of rapamycin (mTOR) upregulate protein synthesis needed for neuronal growth.[38] In vitro as well as in vivo studies have demonstrated increased activation of mTOR pathways with classic psychedelic drugs that lead to increased dendritic growth, density and synapse formation.[39]
The shift in nociceptive processing from acute nociceptive pain towards the experience of suffering in chronic nociplastic pain can be explored further by looking at the neuroplastic changes that occur in the default mode network (DMN) that lead to increased depressive rumination and abnormal self-reflective thinking.[14,17]
The default mode network
Over the last 25 years, neuroscientists have embarked on extensive task-oriented functional magnetic resonance (fMRI) studies. While studying the passive control images, in between images for goal-directed tasks, they noticed areas of the brain that displayed markedly higher activity when individuals were left to rest while thinking by themselves.[40] These areas receive 40% more cerebral blood flow and have much higher metabolic activity than the rest of the brain when at rest.[17] In 2001, a series of articles named these areas the default mode network (DMN), and neuroscientists identified it as its own system, similar to the sensory-motor system or the visual cortex. The DMN has been described as a series of interconnected regions that converge on key areas and act as a central conductor of brain function.[41] The core regions that constitute the DMN are centred around the medial prefrontal cortex (MPFC) and the posterior cingulate cortex (PCC).
The conscious resting state and stimulus-independent thought processes associated with the DMN have led to different hypotheses as to their function.[41] The sentinel hypothesis posits that the DMN has a spontaneous, broad and exogenously driven information-gathering purpose. During the resting state the DMN enters a state of 'watchfulness' and monitors the external environment. The internal mentation hypothesis proposes a series of dynamic mental simulations of alternative futures based on past experiences. It describes functions around autobiographical memory, mental time travel, moral decision-making and theory of mind.[41] Neuroimaging studies conducted in patients with MDD and chronic nociplastic pain have described sustained increased activity in the DMN with decreased functional connectivity to other brain regions.[42] The increased activity seen in the DMN correlates with excessive internal awareness, depressive rumination described as 'loopy thoughts' and trait neuroticism.[17] Decreased functional connectivity to other brain regions is associated with preferential involvement of the MPFC involving emotional and limbic circuitry that shifts nociception away from sensory regions.[43]
An overactive DMN with altered functional connectivity is now considered to be part of the disease process of MDD, Alzheimer's disease, autism spectrum disorder and schizophrenia.[41] Increased DMN activity has been observed in nociplastic pain conditions, and this signal could be used as a biomarker for central sensitisation.[14,44] Interest in the DMN has increased with the new focus on psychedelic psychotherapy. The DMN is highly saturated with 5-HT2A receptors. Controlled studies on individuals with MDD have illustrated the effect of psychedelic-induced 5-HT2A agonism on activity in the DMN.
The effect of LSD and psilocybin on the DMN and other cortical structures in MDD and chronic nociplastic pain may best be described by using the entropic brain hypothesis developed by neuroscientists in 2014.[17] This hypothesis is based on the integrated information theory (IIT) of consciousness that was initially proposed by the neuroscientist Giulio Tononi in 2004.[45] The IIT attempts to equate subjective consciousness with a measurable metric called phi which is made up of certain types of information. The entropic brain hypothesis uses the principle of entropy in the information theory sense to describe the richness of information during certain states of consciousness.[17] The amount of entropy decreases as the level of consciousness changes from the wakeful state through sleeping towards anaesthesia or the comatose state. Researchers conducting fMRI studies on people during psychedelic-induced NOSC have illustrated states of increased entropy above the wakeful state.[45] The conscious experience of increased entropy leads to the perceptual experience of psychedelic drugs and the ability to reframe the egoic-self in terms of its relationship with the internal and external milieu.
The overactive DMN described above imposes a strict hierarchical control over regional brain centres through low-frequency alpha oscillations that originate in layer 5 pyramidal neurons in the cortex.[17] Neuroimaging studies using fMRI describe the low entropy state of an overactive DMN with its depressive rumination and excessive self-awareness in chronic pain and MDD. The deep-layer pyramidal neurons within the cortex are saturated with 5-HT2A receptors. Upon binding of psychedelic drugs, these neurons become depolarised, alpha oscillations stop and cortical activity becomes desynchronised. This releases limbic and frontal brain regions from the DMN and re-sets the brain to function at a higher level of entropy. It is now widely accepted that the brain exhibits higher states of entropy on psychedelic drugs.[46] The experience of higher states of entropy allows for different cognitive and sensory processes to balance the interoceptive processing of the person.[47] The cortical effect of 5-HT2A may provide for a different therapeutic pathway in the management of people with chronic pain in combination with the 5-HT1A receptor binding in the descending noxious inhibiting pathway in the spinal cord.
Serotonin and the descending noxious inhibitory pathway
Serotonin receptors are widely distributed throughout the CNS. There are 14 receptor subtypes, and most of them are G-protein coupled acting via intracellular phospholipase C and inositol triphosphate signalling to increase intracellular calcium.[48] The descending noxious inhibitory pathway contains serotonergic and noradrenergic receptors that affect glutamate and GABA-ergic interneurons in the DSH. The serotonergic circuitry originates at a supraspinal level in the rostroventral medial medulla, periaqueductal grey and nucleus raphe magnus (NRM). Axons from these areas project rostrally to innervate forebrain regions involved in mood and emotion, and caudally to innervate the entire spinal cord.[36] The descending noxious inhibitory pathway has both a nociceptive facilitatory and inhibitory function, depending on the type of serotonin receptor involved and the duration of pain.[49] The balance of inhibitory and facilitatory function maintains a stable baseline of nociceptive awareness.[13]
Both LSD and psilocybin display affinity for the 5-HT1A and 2A receptor, which is expressed in the descending noxious inhibitory control (DNIC) system and may have antinociceptive effects on supraspinal and DSH nociception modulation pathways.[13,50] Serotonin agonism in acute pain facilitates nociception.[13] In chronic nociplastic pain, descending modulation is predominantly inhibitory and acts via 5-HT1A receptors, which are widely expressed in the NRM and the DSH.[51] During chronic inflammatory pain, the inhibitory influence of the descending serotonin pathway is maintained; however, a decrease in basal serotonin release in the spinal cord has been demonstrated in neuropathic pain models.[51] 5-HT1A receptor agonism decreases glutamate release acting at the interneurons that synapse in the DSH. This leads to increased GABA-dependent inhibition of nociception and a decreased substance P release.[36] Supraspinal 5-HT1A agonism lowers glutamate release, with analgesic effects. The 5-HT1A receptor is also involved in the pathogenesis of MDD, and forms the basis of chronic nociplastic pain treatment with antidepressive agents. The analgesic action of LSD and psilocybin via DNIC, as well as cortical processing, provides a compelling argument for the use of these classic psychedelic agents in chronic pain.[16,18] Furthermore, the analgesic effect of 5-HT2A agonism increases with repeated treatment, unlike opioid receptor stimulation, which displays receptor upregulation and decreased therapeutic effect.[13]
Conclusion
The interruption in clinical research brought about by the Controlled Substances Act of 1970 had a major impact on knowledge of psychedelic agents and their potential role in the mental health and chronic pain epidemic of the 21st century. The psychedelic renaissance, led by dedicated researchers and clinicians all over the world, has been slow and careful to reintroduce research into these plant-based alkaloids. The current challenges we face in managing patients with chronic pain, with their substantial set of physical and psychological comorbidities, may achieve significant help from the unfolding research into the role of serotonin receptor binding in treating the neuroplastic mechanisms that underpin chronic nociplastic pain.
Declaration. None.
Acknowledgements. The authors would like to acknowledge the important work being done to decriminalise psychedelic drug use to support mental health and chronic pain research and therapeutic interventions.
Author contributions. JJNvdW conceptualised and wrote the article. RP edited and supported the narrative review process.
Funding. None.
Conflicts of interest. None.
References
1. Isa A, Chetty S. Physiology and pathophysiology of chronic pain (Part I). S Afr J Anaesth Analg 2021;27(6):266-270. https://doi.org/10.36303/sajaa.2021.27.6.2491 [ Links ]
2. Stilwell P, Hudon A, Meldrum K, Pagé MG, Wideman TH. What is pain-related suffering? Conceptual critiques, key attributes, and outstanding questions. J Pain 2022;23(5):729-738. https://dolorg/10.1016/j.jpain.2021.11.005 [ Links ]
3. Das S, Maiti T. Lysergic acid diethylamide as an analgesic agent in patients with terminal illnesses. J Pain Manag 2020;10(1):9-12. https://doi.org/10.2217/pmt-2019-0043 [ Links ]
4. Fitzcharles M-A, Cohen SP, Clauw DJ, Littlejohn G, Usui C, Hàuser W. Nociplastic pain: Towards an understanding of prevalent pain conditions. Lancet 2021;397(10289):2098-2110. https://doi.org/10.1016/s0140-6736(21)00392-5 [ Links ]
5. Melzack R. From the gate to the neuromatrix. J Pain 1999;82(Supplement 1):S121-S126. https://doi.org/10.1016/s0304-3959(99)00145-1 [ Links ]
6. Sheng J, Liu S, Wang Y, Cui R, Zhang X. The link between depression and chronic pain: Neural mechanisms in the brain. Neural Plast 2017;2017:1-10. https://doi.org/10.1155/2017/9724371 [ Links ]
7. IsHak WW, Wen RY, Naghdechi L, et al. Pain and depression: A systematic review. Harv Rev Psychiatry 2018;26(6):352-363. https://doi.org/10.1097/hrp.0000000000000198 [ Links ]
8. Gasser P, Holstein D, Michel Y, et al. Safety and efficacy of lysergic acid diethylamide-assisted psychotherapy for anxiety associated with life-threatening diseases. J Nerv Ment Dis 2014;202(7):513-520. https://doi.org/10.1097/nmd.0000000000000113 [ Links ]
9. Kurland AA. LSD in the supportive care of the terminally ill cancer patient. J Psychoactive Drugs 1985;17(4):279-290. https://doi.org/10.1080/02791072.1985.10524332 [ Links ]
10. Cohen SP, Vase L, Hooten WM. Chronic pain: An update on burden, best practices, and new advances. Lancet 2021;397(10289):2082-2097. https://doi.org/10.1016/s0140-6736(21)00393-7 [ Links ]
11. Whelan A, Johnson MI. Lysergic acid diethylamide and psilocybin for the management of patients with persistent pain: A potential role? J Pain Manag 2018;8(3):217-229. https://doi.org/10.2217/pmt-2017-0068 [ Links ]
12. Carhart-Harris RL, Goodwin GM. The therapeutic potential of psychedelic drugs: past, present, and future. Neuropsychopharmacology 2017;42(11):2105-2113. https://doi.org/10.1038/npp.2017.84 [ Links ]
13. Tao Z-Y, Wang P-X, Wei S-Q, Traub RJ, Li J-F, Cao D-Y. The role of descending pain modulation in chronic primary pain: Potential application of drugs targeting serotonergic system. Neural Plast 2019;2019:1-16. https://doi.org/10.1155/2019/1389296 [ Links ]
14. Ceko M, Frangos E, Gracely J, et al. Default mode network changes in fibromyalgia patients are largely dependent on current clinical pain. NeuroImage 2020;216:116877. https://doi.org/10.1016/j.neuroimage.2020.116877 [ Links ]
15. Johnson MW, Andrew Sewell R, Griffiths RR. Psilocybin dose-dependently causes delayed, transient headaches in healthy volunteers. Drug Alcohol Depend 2012;123(1-3):132-140. https://doi.org/10.1016/j.drugalcdep.2011.10.029 [ Links ]
16. Meade E, Hehir S, Rowan N, Garvey M. Mycotherapy: Potential of fungal bioactives for the treatment of mental health disorders and morbidities of chronic pain. J Fungi 2022;8(3):290. https://doi.org/10.3390/jof8030290 [ Links ]
17. Carhart-Harris RL, Leech R, Hellyer PJ, et al. The entropic brain: A theory of conscious states informed by neuroimaging research with psychedelic drugs. Front Hum Neurosci 2014;8. https://doi.org/10.3389/fnhum.2014.00020 [ Links ]
18. Liechti ME. Modern clinical research on LSD. Neuropsychopharmacology 2017;42(11):2114-2127. https://doi.org/10.1038/npp.2017.86 [ Links ]
19. Weil AT. Drug, set, and setting: The basis for controlled intoxicant use. J Psychoactive Drugs 1984;16(3):271. https://doi.org/10.1080/02791072.1984.10524320 [ Links ]
20. Kast EC, Collins VJ. Study of lysergic acid diethylamide as an analgesic agent. Anesth Analg 1964;43(3):285-291. https://doi.org/10.1213/00000539-196405000-00013 [ Links ]
21. Kast E. Attenuation of anticipation: A therapeutic use of lysergic acid diethylamide. Psychiatr Q 1967;41(4):646-657. https://doi.org/10.1007/bf01575629 [ Links ]
22. Pahnke WN, Kurland AA, Goodman LE, Richards WA. LSD-assisted psychotherapy with terminal cancer patients. Curr Psychiatr Ther 1969;9:144-152. [ Links ]
23. Grof S, Goodman LE, Richards WA, Kurland AA. LSD-assisted psychotherapy in patients with terminal cancer. Int Pharmacopsychiatry 1973;8(3):129-144. https://doi.org/10.1159/000467984 [ Links ]
24. Fanciullacci M, Bene ED, Franchi G, Sicuteri F. Phantom limb pain: Sub-hallucinogenic treatment with lysergic acid diethylamide (LSD-25). J Headache Pain 1977;17(3):118-119. https://doi.org/10.1111/j.1526-4610.1977.hed1703118.x [ Links ]
25. Sewell RA, Halpern JH, Pope HG. Response of cluster headache to psilocybin and LSD. J Neurol 2006;66(12):1920-1922. https://doi.org/10.1212/01.wnl.0000219761.05466.43 [ Links ]
26. Schindler EAD, Gottschalk CH, Weil MJ, Shapiro RE, Wright DA, Sewell RA. Indoleamine hallucinogens in cluster headache: Results of the clusterbusters medication use survey. J Psychoactive Drugs 2015;47(5):372-381. https://doi.org/10.1080/02791072.2015.1107664 [ Links ]
27. Griffiths RR, Johnson MW, Carducci MA, et al Psilocybin produces substantial and sustained decreases in depression and anxiety in patients with life-threatening cancer: A randomised double-blind trial. J Psychopharmacology 2016;30(12):1181-1197. https://doi.org/10.1177/0269881116675513 [ Links ]
28. Bornemann J, Close JB, Spriggs MJ, Carhart-Harris R, Roseman L. Self-medication for chronic pain using classic psychedelics: A qualitative investigation to inform future research. Front Psychiatry 2021;12. https://doi.org/10.3389/fpsyt.2021.735427 [ Links ]
29. Lyes M, Yang KH, Castellanos J, Furnish T. Microdosing psilocybin for chronic pain: A case series. J Pain 2022;164(4):698-702. https://doi.org/10.1097/j.pain.0000000000002778 [ Links ]
30. Isa A, Chetty S. Physiology and pathophysiology of chronic pain (Part II): how does pain become chronic? South Afr J Anaesth Analg 2022;28(1):11-14. https://doi.org/10.36303/sajaa.2022.28.1.2497 [ Links ]
31. Wei S-Q, Tao Z-Y, Xue Y, Cao D-Y. Peripheral sensitisation. In: Turker H, Garcia Benavides L, Ramos Gallardo G, Méndez Del Villar M (eds). Peripheral Nerve Disorders and Treatment. London: IntechOpen, 2022. https://doi.org/10.5772/intechopen.90319 [ Links ]
32. Di Lernia D, Serino S, Riva G. Pain in the body. Altered interoception in chronic pain conditions: A systematic review. Neurosci Biobehav Rev 2016;71:328-341. https://doi.org/10.1016/j.neubiorev.2016.09.015 [ Links ]
33. Uddin LQ, Nomi JS, Hébert-Seropian B, Ghaziri J, Boucher O. Structure and function of the human insula. J Clin Neurophysiol 2017;34(4):300-306. https://doi.org/10.1097/wnp.0000000000000377 [ Links ]
34. Doan L, Manders T, Wang J. Neuroplasticity underlying the comorbidity of pain and depression. Neural Plast 2015;2015:1-16. https://doi.org/10.1155/2015/504691 [ Links ]
35. Das S, Barnwal P, Ramasamy A, Sen S, Mondal S. Lysergic acid diethylamide: A drug of 'use'? Ther Adv Psychopharmacol 2016;6(3):214-228. https://doi.org/10.1177/2045125316640440 [ Links ]
36. Haleem DJ. Targeting serotonin1a receptors for treating chronic pain and depression. Curr Neuropharmacol 2019;17(12):1098-1108. https://doi.org/10.2174/1570159x17666190811161807 [ Links ]
37. Ji R-R, Berta T, Nedergaard M. Glia and pain: Is chronic pain a gliopathy? J Pain 2013;154(suppl 1):S10-S28. https://doi.org/10.1016/j.pain.2013.06.022 [ Links ]
38. Edinoff AN, Fort JM, Singh C, et al. Alternative options for complex, recurrent pain states using cannabinoids, psilocybin, and ketamine: A narrative review of clinical evidence. Neurol Int 2022;14(2):423-436. https://doi.org/10.3390/neurolint14020035 [ Links ]
39. Ly C, Greb AC, Cameron LP, et al. Psychedelics promote structural and functional neural plasticity. Cell Rep 2018;23(11):3170-3182. https://doi.org/10.1016/j.celrep.2018.05.022 [ Links ]
40. Callard F, Margulies DS. What we talk about when we talk about the default mode network. Front Hum Neurosci 2014;8:619. https://doi.org/10.3389/fnhum.2014.00619 [ Links ]
41. Buckner RL, Andrews-Hanna JR, Schacter DL. The brain's default network: Anatomy, function, and relevance to disease. Ann N Y Acad Sci 2008;1124:1-38. https://doi.org/10.1196/annals.1440.011 [ Links ]
42. Tozzi L, Zhang X, Chesnut M, Holt-Gosselin B, Ramirez CA, Williams LM. Reduced functional connectivity of default mode network subsystems in depression: Meta-analytic evidence and relationship with trait rumination. NeuroImage: Clinical 2021;30:102570. https://doi.org/10.1016/j.nicl.2021.102570 [ Links ]
43. Hashmi JA, Baliki MN, Huang L, et al. Shape shifting pain: Chronification of back pain shifts brain representation from nociceptive to emotional circuits. J Brain 2013;136(9):2751-2768. https://doi.org/10.1093/brain/awt211 [ Links ]
44. Loggia ML, Kim J, Gollub RL, et al. Default mode network connectivity encodes clinical pain: An arterial spin labeling study. J Pain 2013;154(1):24-33. https://doi.org/10.1016/j.pain.2012.07.029 [ Links ]
45. Carhart-Harris RL. The entropic brain - revisited. J Neuropharmacol 2018;142:167-178. https://doi.org/10.1016/j.neuropharm.2018.03.010 [ Links ]
46. Carhart-Harris R, Nutt D. Serotonin and brain function: A tale of two receptors. J Psychopharmacol 2017;31(9):1091-120. https://doi.org/10.1177/0269881117725915 [ Links ]
47. Baliki MN, Baria AT, Apkarian AV. The cortical rhythms of chronic back pain. J Neurosci 2011;31(39):13981-13990. https://doi.org/10.1523/jneurosci.1984-11.2011 [ Links ]
48. Zhang G, Stackman RW. The role of serotonin 5-HT2A receptors in memory and cognition. Front Pharmacol 2015;6:225. https://doi.org/10.3389/fphar.2015.00225 [ Links ]
49. Suzuki R, Rygh LJ, Dickenson AH. Bad news from the brain: Descending 5-HT pathways that control spinal pain processing. Trends Pharmacol Sci 2004;25(12):613-617. https://doi.org/10.1016/j.tips.2004.10.002 [ Links ]
50. Szabo A. Psychedelics and immunomodulation: Novel approaches and therapeutic opportunities. Front Immunol 2015;6:358. https://doi.org/10.3389/fimmu.2015.00358 [ Links ]
51. Bardin L. The complex role of serotonin and 5-HT receptors in chronic pain. Behav Pharmacol 2011;22(5 and 6):390-404. https://doi.org/10.1097/fbp.0b013e328349aae4 [ Links ]
 Correspondence:
Correspondence:
J J N van der Walt
johanvanderwalt07@gmail.com
Accepted 28 September 2023


{kind=link}